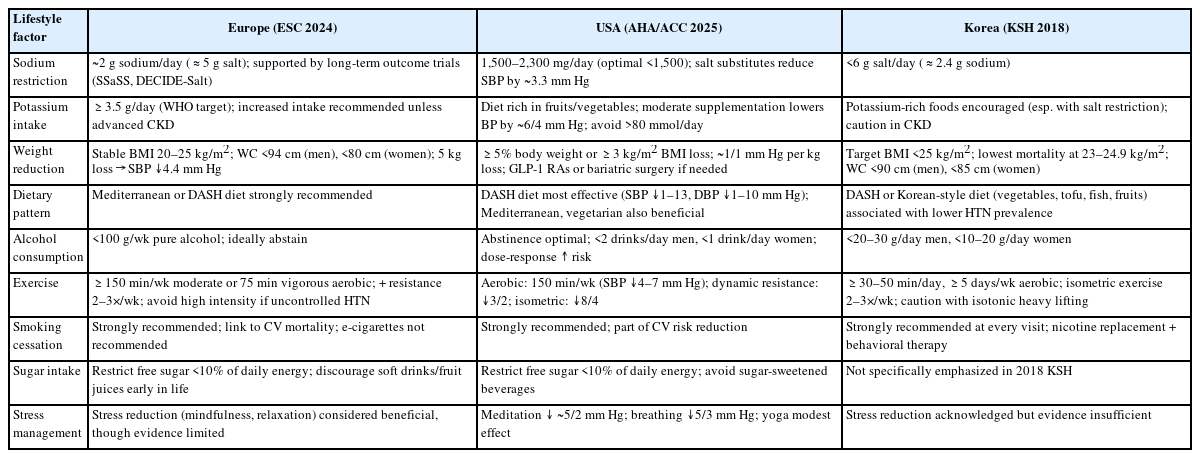
Hypertension is one of the leading chronic diseases globally and a major contributor to cardiovascular morbidity and mortality. Despite advances in pharmacological therapy, medication alone remains limited in achieving optimal control. This review synthesizes recent hypertension management guidelines, including those from the European Society of Cardiology (ESC, 2024), American Heart Association/American College of Cardiology (AHA/ACC, 2025), Taiwan Society of Cardiology/Hypertension Society (2022), and Korean Society of Hypertension (KSH, 2018). All guidelines consistently emphasize sodium restriction, weight reduction, regular exercise, moderation of alcohol intake, smoking cessation, and adoption of healthy dietary patterns such as the Dietary Approaches to Stop Hypertension, Mediterranean, or culturally adapted diets. The ESC 2024 guideline elevates lifestyle modification to Class I, Level A, specifying targets for sodium (<2 g/day) and potassium (≥3.5 g/day). The AHA/ACC 2025 guideline provides quantitative estimates, reporting approximately 1/1 mm Hg blood pressure reduction per kilogram of weight loss, and incorporates newer strategies such as glucagon-like peptide-1 receptor agonists and bariatric surgery when lifestyle measures alone are insufficient. Taiwan’s 2022 guideline frames recommendations under the S-ABCDE (sodium restriction, alcohol limitation, body weight reduction, cigarette cessation, diet adaptation, exercise adoption) mnemonic and uniquely includes genetic factors such as ALDH2 polymorphisms. The KSH 2018 guideline emphasizes salt restriction (<6 g/day), maintaining a body mass index <25 kg/m2, and adherence to traditional Korean diets. Lifestyle modification remains the cornerstone of hypertension prevention and management, particularly in primary care. Future directions should focus on integrating these approaches with pharmacotherapy, digital health strategies, and personalized prescriptions.
Citations
Citations to this article as recorded by
Association of Lifestyle Factors With Blood Pressure Control Among Hypertensive U.S. Adults: An Analysis of the National Ambulatory Medical Care Survey (NAMCS) 2010–2015 Moses C Odoeke, Afi T Djaba, Adedoyin Olawoye, Taiwo G Adekanmbi, Hillary C Ugwu, O. B Bomide, Kosisochi E Achara Cureus.2026;[Epub] CrossRef
Lifestyle Interventions for Blood Pressure Control: A Narrative Review of Global Evidence and Indonesian Perspectives Hery Kurniawan, Avril Bella Audyna Journal of Tropical Pharmacy and Chemistry .2026; 10(1): 57. CrossRef
Nutraceuticals for the Management of Cardiovascular Health: A Mechanistic and Evidence-Based Review Focusing on Atherosclerosis and Hypertension Phaniendra Alugoju, Charanraj Goud Alladi, Nyshadham Chaitanya, Luxitaa Goenka, Kishoree Kumaree, Sudarshan SJ, Krishnaswamy Duraisamy, Naeem Ullah Nutrients.2026; 18(14): 2226. CrossRef
Diabetes mellitus is a complex chronic disease with a rapidly increasing global prevalence. For this condition, non-pharmacological lifestyle modification is as important as pharmacological treatment. This review aims to comprehensively examine lifestyle prescriptions for diabetes across multiple domains to integrate current insights and understanding. In medical nutrition therapy, which is central to diabetes treatment and management, excessive carbohydrate intake should be restricted, while individualized consumption of high-quality carbohydrates, protein, and unsaturated fatty acids is recommended. Intake of added sugars and sodium should also be limited. Physical activity should similarly be tailored to the individual, with a combination of aerobic exercise and resistance training recommended. Careful consideration of hypoglycemia risk and diabetes complications is essential. Additional strategies include limitations on uninterrupted sedentary time to less than 30 minutes, maintenance of a healthy body weight, smoking cessation, alcohol abstinence, sleep health improvements, and attention to psychosocial care. In primary care settings, patient-specific assessment, multidisciplinary lifestyle prescriptions, and education to support behavior modification are expected to play a pivotal role in the treatment and management of diabetes.
Citations
Citations to this article as recorded by
Knowledge, attitude, and practice of allied healthcare professionals about lifestyle medicine for diabetes: A cross-sectional study Mona Mohamed Taha, Shaima A Alothman, Rana Alawafi, Rahaf Mohammed Alshareef, Sarah Mohammed Al-Subaie, Najd Abdullah AlKhushaiban, Najd A Al-Salem, Asmaa Rafeeq, Ali Mohamed Ali Ismail WORK: A Journal of Prevention, Assessment & Rehabilitation.2026;[Epub] CrossRef
Objectives: There is limited knowledge regarding the impact of
lifestyle changes on cardiovascular events and mortality among individuals with
prehypertension or prediabetes.
Methods: This was a serial retrospective cohort study utilizing data
from the Korean National Health Insurance Service Health Screening Cohort. The
primary outcome considered in the study was major adverse cardiovascular events
(MACE).
Results: A higher risk of MACE was found in men with prehypertension
whose unhealthy lifestyle deteriorated (hazard ratio [HR], 1.13; 95% CI,
1.04–1.23; P=0.004), those who gained weight (HR, 1.15; 95% CI,
1.03–1.28; P=0.010), and those who began smoking (HR, 1.34; 95% CI,
1.17–1.55; P<0.001). Conversely, a reduced risk of MACE was
observed in men with prehypertension who improved their unhealthy lifestyle,
quit smoking, reduced alcohol consumption, or increased the frequency of
physical activity. In men with prediabetes, the risk of MACE was higher in those
whose unhealthy lifestyle worsened (HR, 1.23; 95% CI, 1.12–1.35;
P<0.001), those who gained weight (HR, 1.19; 95% CI, 1.06–1.33;
P=0.003), those who started smoking (HR, 1.41; 95% CI, 1.22–1.64;
P<0.001), and those who decreased their physical activity frequency (HR,
1.21; 95% CI, 1.09–1.35; P<0.001).
Conclusion: Preventive lifestyle changes reduce cardiovascular
events and mortality, particularly in men at risk of developing hypertension or
type 2 diabetes.
Citations
Citations to this article as recorded by
Assessment of Cardiovascular Risk in Prehypertensive Subjects in Kisangani (DR Congo): An Analytical Cross-Sectional Study Using the ISH/WHO Score Ossinga Bassandja, Kayembe Tshilumba, Batina Agasa World Journal of Cardiovascular Diseases.2025; 15(04): 199. CrossRef

 , Gyu Bae Lee
, Gyu Bae Lee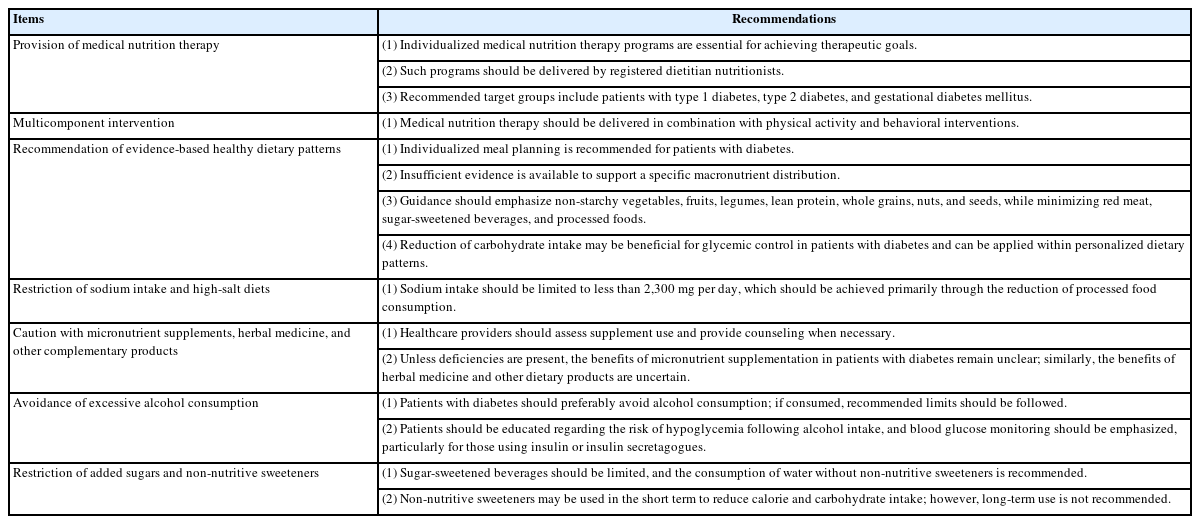
 First
First Prev
Prev

