Department of Anesthesiology and Pain Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
Corresponding author: Jong-Yeon Lee, Department of Anesthesiology and Pain Medicine, CHA Bundang Medical Center, CHA University, 59 Yatap-ro, Bundang-gu, Seongnam 463-712, Korea. Tel: 82-31-780-5433, Fax: 82-31-701-9433, jongyeonl@yahoo.co.kr
• Received: June 8, 2012 • Accepted: June 27, 2012
A healthy 35-year-old man who was scheduled for closed reduction of nasal bone fracture developed atrial fibrillation during induction of general anesthesia after intravenous glycopyrrolate injection. During emergence of general anesthesia, atrial fibrillation was suddenly changed to paroxysmal supraventricular tachycardia with 200 beat per minute and lasted for about 10 seconds. Because blood pressure was stable, esmolol was used to reduce ventricular response. At recovery room, ventricular response reduction about 55 beat per minute was observed after intravenous injection of verapamil 5 mg. Thereafter, the rhythm was returned to normal sinus rhythm with bradycardia.
1. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285:2370-2375.
3. Olgin JE, Zipes DP. Braunwald E, Zipes DP, Libby P. Specific arrhythmias: diagnosis and tretment. Branwald's heart disease 2005;7th ed. Pennsylvania, Elsevier. 803-861.
4. Djousse L, Levy D, Benjamin EJ, Blease SJ, Russ A, Larson MG, et al. Long-term alcohol consumption and the risk of atrial fibrillation in the Framingham Study. Am J Cardiol 2004;93:710-713.
5. Vaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation: the Framingham Heart Study. Circulation 1994;89:724-730.
7. Wasmund SL, Li JM, Page RL, Joglar JA, Kowal RC, Smith ML, et al. Effect of atrial fibrillation and an irregular ventricular response on sympathetic nerve activity in human subjects. Circulation 2003;107:2011-2015.
11. Boriani G, Diemberger I, Biffi M, Domenichini G, Martignani C, Valzania C, et al. Electrical cardioversion for persistent atrial fibrillation or atrial flutter in clinical practice: predictors of long-term outcome. Int J Clin Pract 2007;61:748-756.
13. Testa L, Biondi-Zoccai GG, Dello Russo A, Bellocci F, Andreotti F, Crea F. Rate-control vs. rhythm-control in patients with atrial fibrillation: a meta-analysis. Eur Heart J 2005;26:2000-2006.
15. Waxman HL, Myerburg RJ, Appel R, Sung RJ. Verapamil for control of ventricular rate in paroxysmal supraventricular tachycardia and atrial fibrillation or flutter: a double-blind randomized cross-over study. Ann Intern Med 1981;94:1-6.
Atrial Fibrillation during General Anesthesia Induction and Paroxysmal Supraventricular Tachycardia on Emergence
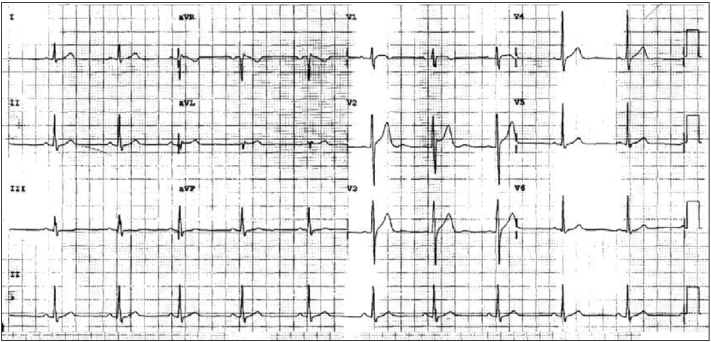
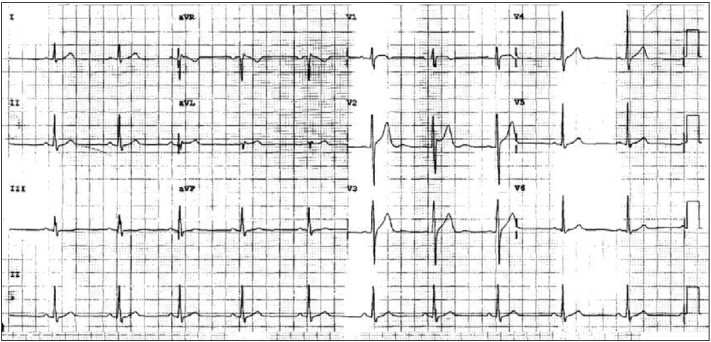
Fig. 1
Electrocardiographic finding before surgery. Normal sinus rhythm (64 beats/min) is observed.
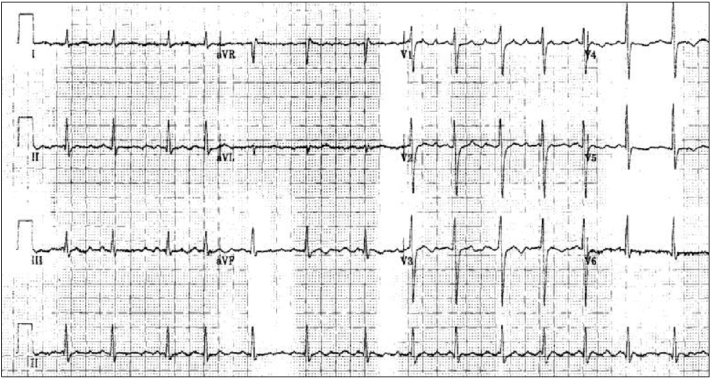
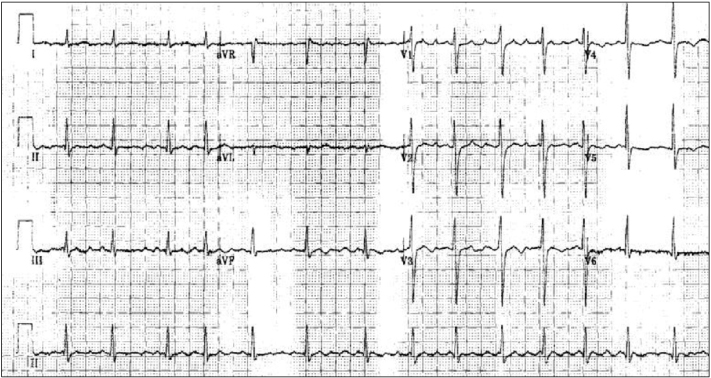
Fig. 2
Electrocardiographic finding at the recovery room. Atrial fibrillation with irregular ventricular response (95 beats/min) is observed.
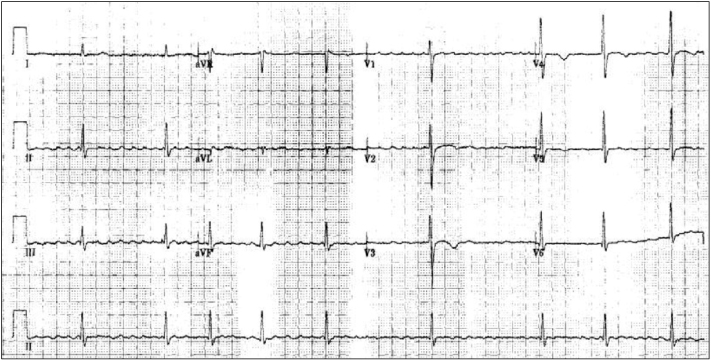
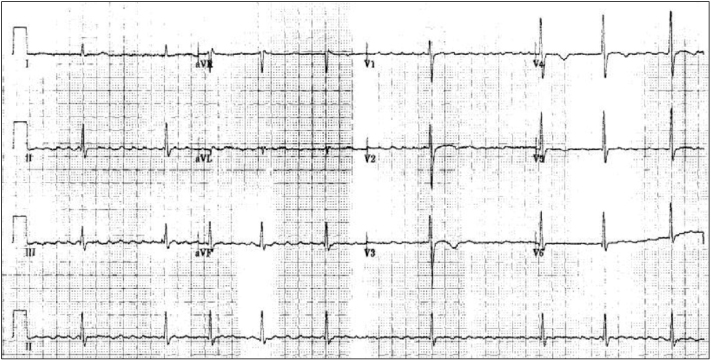
Fig. 3
Electrocardiographic finding after verapamil infusion. Slow ventricular response (55 beats/min) is observed, but atrial fibrillation is continued.
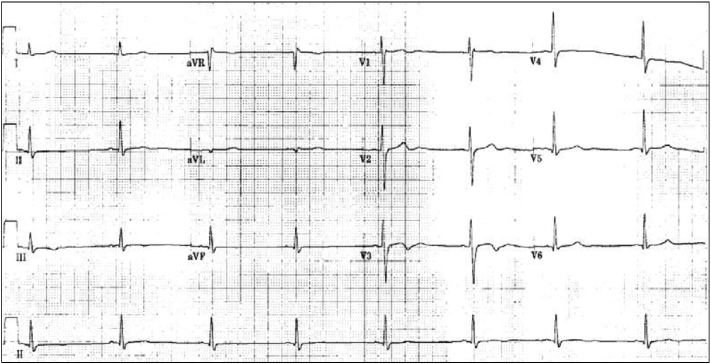
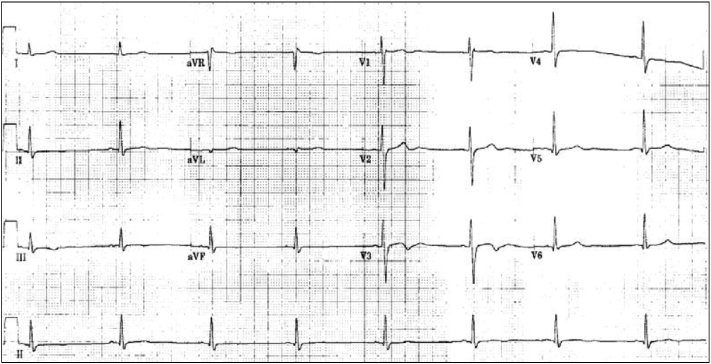
Fig. 4
Electrocardiographic findings on the 10th day after surgery. Normal sinus rhythm with bradycardia (46 beats/min) is observed.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Atrial Fibrillation during General Anesthesia Induction and Paroxysmal Supraventricular Tachycardia on Emergence