Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
Corresponding author: Jae Myung Cha, Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, 892 Dongnam-ro, Gangdong-gu, Seoul 134-727, Korea. Tel: 82-2-440-6113, Fax: 82-2-440-6295, drcha@khu.ac.kr
• Received: June 14, 2012 • Accepted: July 16, 2012
Surgery is the primary treatment for adenocarcinoma originating from the esophagogastric junction. However, many physicians attempt various endoscopic treatments for the cases of early adenocarcinoma and high-grade dysplasia of esophagogastric junction in order to avoid the high risk of complications associated with surgical resection. Recently, there is an increasing tendency to use endoscopic mucosal resection for the management of early esophageal cancer due to low morbidity and mortality rates. We report here on a case of early adenocarcinoma at esophagogastric junction successfully treated with endoscopic mucosal resection.
2. Nunobe S, Nakanishi Y, Taniguchi H, Sasako M, Sano T, Kato H, et al. Two distinct pathways of tumorigenesis of adenocarcinomas of the esophagogastric junction, related or unrelated to intestinal metaplasia. Pathol Int 2007;57:315-321.
4. Rice TW, Blackstone EH, Rusch VW. 7th edition of the AJCC Cancer Staging Manual: esophagus and esophagogastric junction. Ann Surg Oncol 2010;17:1721-1724.
8. Abraham SC, Singh VK, Yardley JH, Wu TT. Hyperplastic polyps of the esophagus and esophagogastric junction: histologic and clinicopathologic findings. Am J Surg Pathol 2001;25:1180-1187.
9. Heitmiller RF, Redmond M, Hamilton SR. Barrett's esophagus with high-grade dysplasia: an indication for prophylactic esophagectomy. Ann Surg 1996;224:66-71.
11. Crumley AB, Going JJ, McEwan K, McKernan M, Abela JE, Shearer CJ, et al. Endoscopic mucosal resection for gastroesophageal cancer in a U.K. population: long-term follow-up of a consecutive series. Surg Endosc 2011;25:543-548.
12. Ell C, May A, Gossner L, Pech O, Gunter E, Mayer G, et al. Endoscopic mucosal resection of early cancer and high-grade dysplasia in Barret'ts esophagus. Gastroenterology 2000;118:670-677.
13. Kodama M, Kakegawa T. Treatment of superficial cancer of the esophagus: a summary of responses to a questionnaire on superficial cancer of the esophagus in Japan. Surgery 1998;123:432-439.
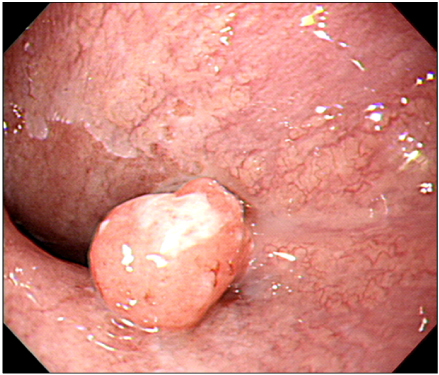
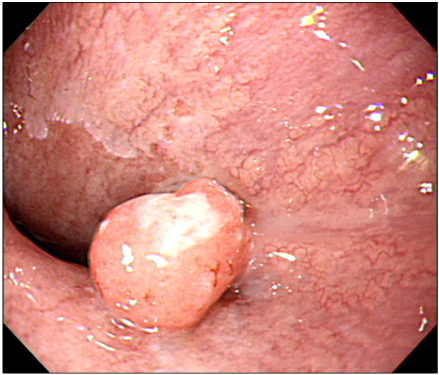
An endoscopic finding. Endoscopy finding shows a 10×15 mm sized polyp, which mimics a sentinel polyp at the esophagogastric junction. White exudate is noted at the top of polyp, however, any ulcer or bleeding is not noted at the surface of polyp.
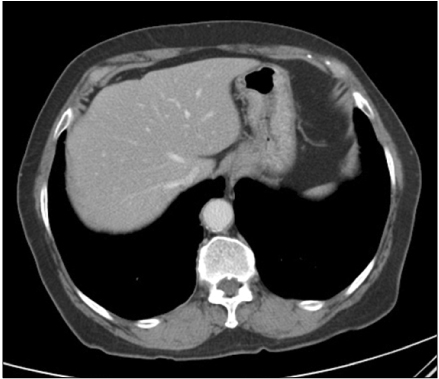
Fig. 2
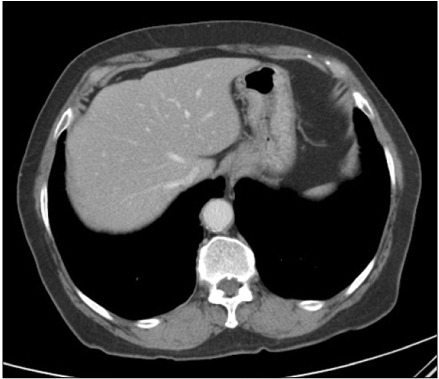
Abdominal computed tomography. It does not show a demonstrable mass or abnormal wall thickening at the esophagogastric junction.
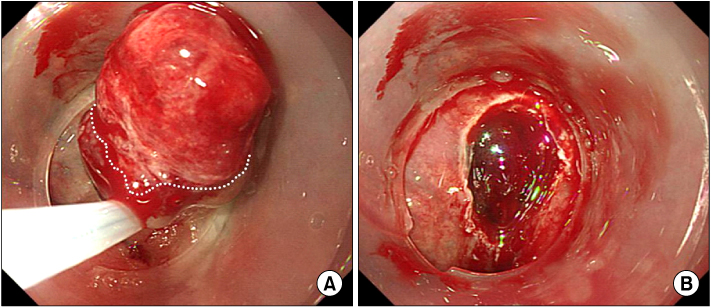
Fig. 3
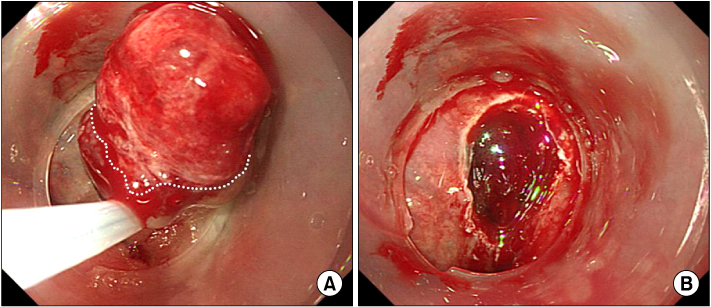
Endoscopic findings. (A) Early cancer of esophagogastic junction, which is completely resected with cap-pitted endoscopic mucosal resection. Sufficient amount of normal mucosa (white dot line) is secured under the base of malignant polyp. (B) Endoscopic resection is complete without any remnant lesions.
Fig. 4
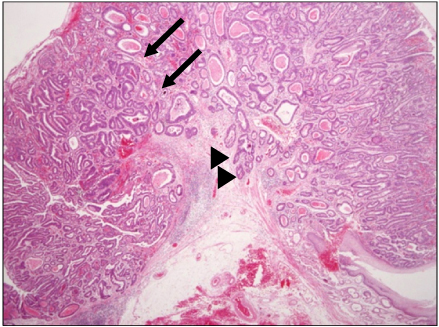
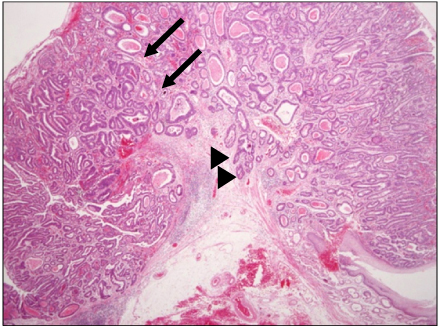
Pathologic findings. The specimen shows moderate differentiated adenocarcinoma (arrows) with negative deep and lateral margins (H&E, ×20). The adenocarcinoma is confined within the mucosal layer, however, focal 500 µm submucosal invasion is noted (arrow heads).
A Case of Early Adenocarcinoma at Esophagogastric Junction Treated with Cap-pitted Endoscopic Mucosal Resection
Fig. 1
An endoscopic finding. Endoscopy finding shows a 10×15 mm sized polyp, which mimics a sentinel polyp at the esophagogastric junction. White exudate is noted at the top of polyp, however, any ulcer or bleeding is not noted at the surface of polyp.
Fig. 2
Abdominal computed tomography. It does not show a demonstrable mass or abnormal wall thickening at the esophagogastric junction.
Fig. 3
Endoscopic findings. (A) Early cancer of esophagogastic junction, which is completely resected with cap-pitted endoscopic mucosal resection. Sufficient amount of normal mucosa (white dot line) is secured under the base of malignant polyp. (B) Endoscopic resection is complete without any remnant lesions.
Fig. 4
Pathologic findings. The specimen shows moderate differentiated adenocarcinoma (arrows) with negative deep and lateral margins (H&E, ×20). The adenocarcinoma is confined within the mucosal layer, however, focal 500 µm submucosal invasion is noted (arrow heads).
Fig. 1
Fig. 2
Fig. 3
Fig. 4
A Case of Early Adenocarcinoma at Esophagogastric Junction Treated with Cap-pitted Endoscopic Mucosal Resection