Abstract
A 30-year-old man visited the emergency room for chest pain, dyspnea and fever. Despite increased serum cardiac enzymes, ST segment elevation and inferior wall akinesis in electrocardiography and echocardiography, no atherosclerosis was evident in the coronary angiography. However, radionuclide myocardial perfusion image at day 2 showed a persistent perfusion defect in the left ventricular (LV) inferior wall. At day 3, prominent myocardial edema and severe LV systolic dysfunction developed with signs of heart failure. In this case, fulminant myocarditis seemed to originate from the right coronary artery territory and simulated a ST segment elevation myocardial infarction without coronary artery obstruction. The pathogenesis of the localized perfusion defect was unlcear.
-
Keywords: Coronary artery vasospasm; Myocardial infarction; Myocardial perfusion image; Myocarditis
Introduction
Myocarditis may present with a wide range of symptoms, ranging from mild dyspnea or chest pain that resolves without specific therapy to cardiogenic shock and death. In the clinical setting, acute myocarditis may occasionally present with clinical manifestations mimicking that of acute myocardial ischemia, such as chest pain, electrocardiographic abnormalities, serum creatine kinase (CK-MB) elevation and hemodynamic instability. We report the case of a patient who had transient myocarditis clinically mimicking acute coronary syndrome with an evidence of a persistent perfusion defect in the left ventricular (LV) inferior wall by myocardial perfusion image (MPI).
Case
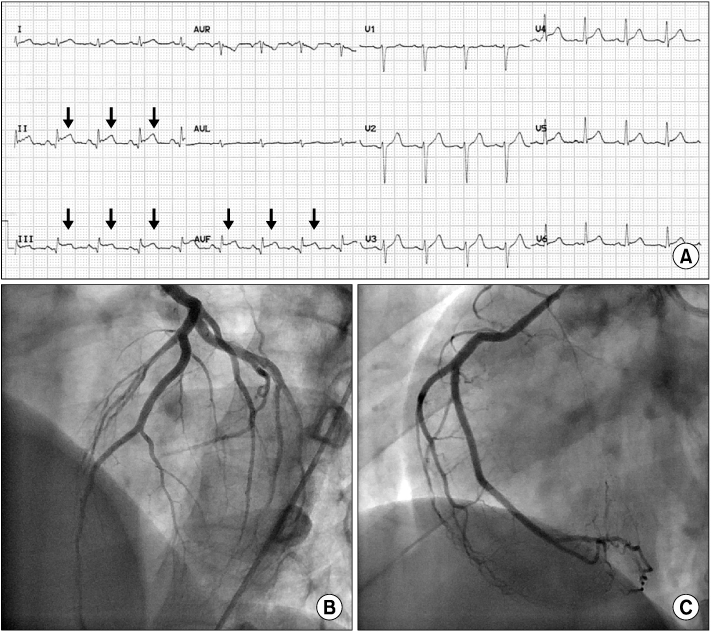
A 30-year-old man visited the emergency room with three days history of chest pain, dyspnea and fever. Chest pain was substernal and crushing in nature. The patient had never smoked and denied any kind of significant disease. He had not been exposed to any drugs or toxic materials. Family history was benign, too. Blood pressure and heart rate were 130/80 mmHg and 109/min, respectively. The patient was mildly dyspneic (respiratory rate: 28/min) and febrile (body temperature: 38.1℃). Physical examination revealed no apparent abnormality and chest roentgenogram showed no pulmonary congestion. However, standard 12-lead electrocardiography (ECG) showed small Q waves and ST segment elevations in leads II, III and aVF (
Fig. 1A). In the laboratory findings, serum liver aminotransferase was mildly elevated, with 54 IU/L of aspartate transminase and 31 IU/L of alanine transaminase. Cardiac enzymes were also elevated in concentration, with a CK-MB level of 23.81 ng/mL and troponin T level of 0.98 ng/mL.
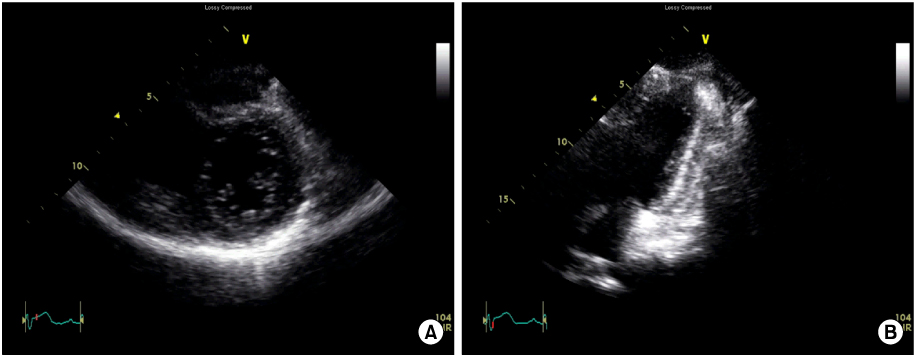
Two-dimensional (2D) echocardiography revealed akinesis in basal-to-mid inferior wall of the left ventricle (LV) with normal sized LV end-diastolic dimension (48 mm) and preserved LV ejection fraction (LVEF, 55%). The septal and the posterior wall thickness were 10.5 mm and 10.8 mm, respectively. Because of akinesis in LV inferior wall, acute ST segment elevation myocardial infarction (STEMI) was strongly suggested (
Fig. 2). However, emergent coronary angiography showed normal coronary arteries (
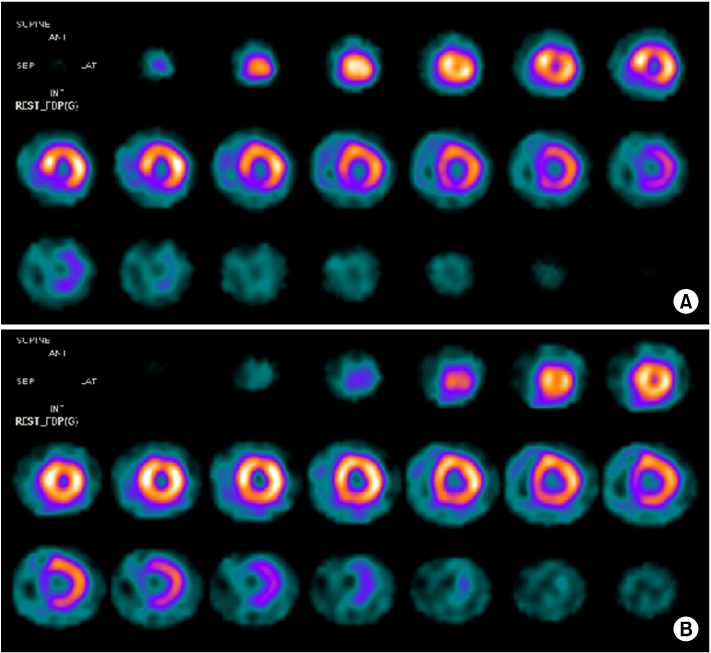
Fig. 1B and 1C). As myocardial infarction due to transient right coronary artery (RCA) vasospasm was proposed as a tentative diagnosis, oxygen, aspirin and intravenous diltiazem were administered. At day 2, however, radionuclide MPI with Tc
99m-sestamibi showed persistent perfusion defects localized in the basal-to-mid inferior segments, which indicated ongoing myocardial ischemia, despite patent coronary blood flow in the RCA (
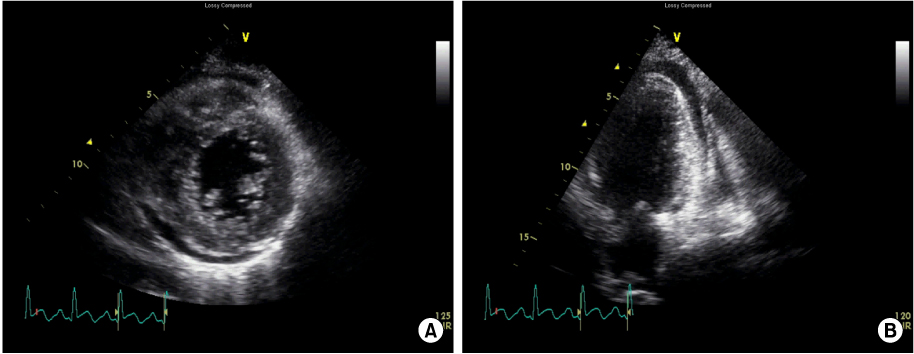
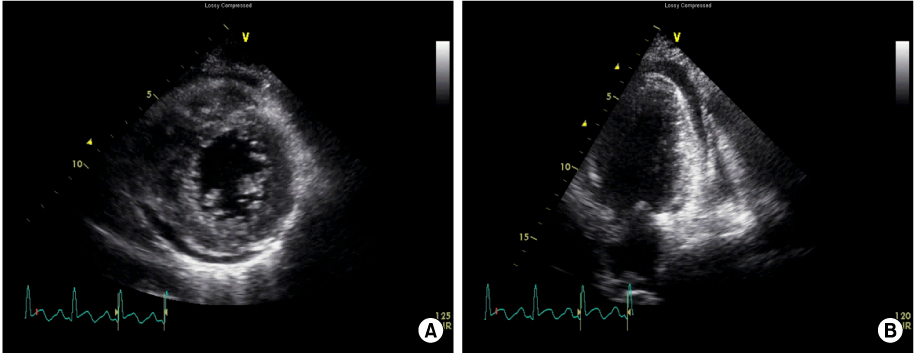
Fig. 3A). At day 3, dyspnea was aggravated and rales were audible in both lung fields. Follow-up 2D echocardiography showed prominent myocardial edema and severe diffuse hypokinesis in both ventricles with mild circumferential pericardial effusion. LVEF was 20%, while the septal and the posterior wall thickness were 13.2 mm and 12.5 mm, respectively (
Fig. 4). Cardiac enzymes were elevated continuously. At that point, fulminant course of acute myocarditis was considered and supportive treatment was decided. Loop diuretics and angiotensin converting enzyme (ACE) inhibitor improved symptoms of heart failure and the patient could be discharged at day 6. A 2D echocardiography and MPI 2 weeks later showed complete normalization of LVEF and wall thickness (septal and posterior wall thickness were 10.9 mm and 10.5 mm, respectively) and normal homogenous perfusion in the LV (
Fig. 3B). In ECG, small Q waves and ST elevation in leads II, III and a VF disappeared.
The patient was finally diagnosed with fulminant myocarditis, initially simulating STEMI. At the 6-month follow-up, the patient had been asymptomatic and was well.
Discussion
This is a case of fulminant myocarditis presented with symptoms and signs similar to STEMI. The unique finding in the present case was an ongoing perfusion defect demostrated by MPI during maintenance of normal coronary flow. Althouth ST segment elevation in myocarditis has been explained by transient vasospasm of epicardial coronary artery, we believe direct viral invasion in the local microvasculature caused transmural ischemia without coronary artery vasospasm, simulating STEMI. This may have important clinical implications because commonly used coronary arteriodilator such as nitrates and calcium channel blockers may not be effective in preventing myocardial ischemia in this clinical setting.
Myocarditis is thought to result from viral infections and post-viral immune-mediated responses (e.g., clonal expansion of B lymphocytes and production of anti-heart autoantibodies). Although ventricular dysfunction in most patients with myocarditis recovers without sequelae, persistent autoimmune processes can lead to irreversible dilated cardiomyopathy [
1-
3]. While coxackie group B serotype in enterovirus and adenovirus have been long perceived as the predominant cause of viral myocarditis, the progress of molecular technique such as polymerase chain reaction and in situ hybridization demonstrated the presence of parvovirus B19 (PVB19) and human herpesvirus 6 in endomyocardial biopsies more frequently than previously appreciated [
1,
3,
4].
Because the patient in the present case had prodromes of upper respiratory infection and completely recovered without collateral abnormality, viral infection was considered as the most likely cause among the various etiologies of myocarditis.
Fulminant myocarditis can present with a manner similar to acute coronary syndrome and vasospasm of the epicardial coronary arteries is regarded as the most responsible mechansim [
5,
6]. However, there has been uncertainty concerning the mechanism of coronary artery vasospasm associated with myocarditis and there are opinions that coronary vasospasm depends on the property of the invading virus [
7-
9].
Mahrholdt et al. [
10] reported PVB19 and human herpesvirus 6 (HHV6) were the most frequent viruses in their cohort of myocarditis. They also demonstrated that PVB19 infection tended to manifest like myocardial infarction, while HHV6 infection was likely to present with heart failure [
11]. This notion was supported by a study with biopsy-proven myocarditis, where coronary artery vasospasm was more frequent in PVB19 myocarditis as compared with HHV6 myocarditis [
9], and by reports that PVB19 preferentially invades vascular endothelial cells preferably, while HHV6 targets immune cells [
12-
14].
In the present case, myocarditis started in a small area corresponding to the RCA territory and propagated to both ventricles. From the present case, we could hypothesize a certain viral infection (e.g., PVB19) started in distal small branches of the RCA and subsequent vascultitis in microvessels lead to persistent transmural ischemia without vasospasm, which manifested as a syndrome mimicking STEMI.
The lack of immunohistological evidence of inflammatory infiltrates in the myocardium and unproven viral etiology are caveats of this case report. However, because endomyocardial biopsy is generally reserved for progressive heart failure refractory to standard managment or cardiomyopathies associated with conduction system abnormality [
15], endomyocardial biopsy was not performed in this case. Furthermore, because viral genome was detected in less than half of subjects' endomyocardial biopsies [
16], we thought the endomyocardial biospy for the surveillance of viral genome was not essential, considering quick recovery of ventricular function and the potential harm of the invasive procedure.
Contrast-enhanced magnetic resonance image (MRI) seems promising for accurately diagnosing myocarditis and could have been very helpful in the current case. However, definite diagnosis of myocarditis remains unsettled and MRI has not yet been routinely recommended for the diagnosis of fulminant myocarditis [
3].
References
- 1. Magnani JW, Dec GW. Myocarditis: current trends in diagnosis and treatment. Circulation 2006;113:876-890.
- 2. Liu PP, Mason JW. Advances in the understanding of myocarditis. Circulation 2001;104:1076-1082.
- 3. Kindermann I, Barth C, Mahfoud F, Ukena C, Lenski M, Yilmaz A, et al. Update on myocarditis. J Am Coll Cardiol 2012;59:779-792.
- 4. Pankuweit S, Lamparter S, Schoppet M, Maisch B. Parvovirus B19 genome in endomyocardial biopsy specimen. Circulation 2004;109:e179.
- 5. McCully RB, Cooper LT, Schreiter S. Coronary artery spasm in lymphocytic myocarditis: a rare cause of acute myocardial infarction. Heart 2005;91:202.
- 6. Silva D, Marques P, Martins S, Bordalo E Sa AL, Nobrega J, Duarte J, et al. Coronary artery vasospasm and acute myocarditis: a rare association. Rev Port Cardiol 2010;29:1879-1888.
- 7. Shimokawa H. Cellular and molecular mechanisms of coronary artery spasm: lessons from animal models. Jpn Circ J 2000;64:1-12.
- 8. Gibelli G, Devizzi S, Brioschi P, Rimini A, Biasi S. Sudden ST elevation with angina-like pain in myocarditis. An uncommon course of a common disease: strategic role of cardiac magnetic resonance. J Cardiovasc Med (Hagerstown) 2009;10:264-266.
- 9. Yilmaz A, Mahrholdt H, Athanasiadis A, Vogelsberg H, Meinhardt G, Voehringer M, et al. Coronary vasospasm as the underlying cause for chest pain in patients with PVB19 myocarditis. Heart 2008;94:1456-1463.
- 10. Mahrholdt H, Goedecke C, Wagner A, Meinhardt G, Athanasiadis A, Vogelsberg H, et al. Cardiovascular magnetic resonance assessment of human myocarditis: a comparison to histology and molecular pathology. Circulation 2004;109:1250-1258.
- 11. Mahrholdt H, Wagner A, Deluigi CC, Kispert E, Hager S, Meinhardt G, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006;114:1581-1590.
- 12. Kandolf R. Virus etiology of inflammatory cardiomyopathy. Dtsch Med Wochenschr 2004;129:2187-2192.
- 13. Bultmann BD, Klingel K, Sotlar K, Bock CT, Baba HA, Sauter M, et al. Fatal parvovirus B19-associated myocarditis clinically mimicking ischemic heart disease: an endothelial cell-mediated disease. Hum Pathol 2003;34:92-95.
- 14. Prober C. Sixth disease and the ubiquity of human herpesviruses. N Engl J Med 2005;352:753-755.
- 15. Cooper LT, Baughman KL, Feldman AM, Frustaci A, Jessup M, Kuhl U, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. J Am Coll Cardiol 2007;50:1914-1931.
- 16. Bowles NE, Ni J, Kearney DL, Pauschinger M, Schultheiss HP, McCarthy R, et al. Detection of viruses in myocardial tissues by polymerase chain reaction. evidence of adenovirus as a common cause of myocarditis in children and adults. J Am Coll Cardiol 2003;42:466-472.
Fig. 1Electrocardiography and coronary angiography data. Q waves and ST segment elevation are indicated by arrows (A). Coronary angiography shows normal coronary arteries (B, C).
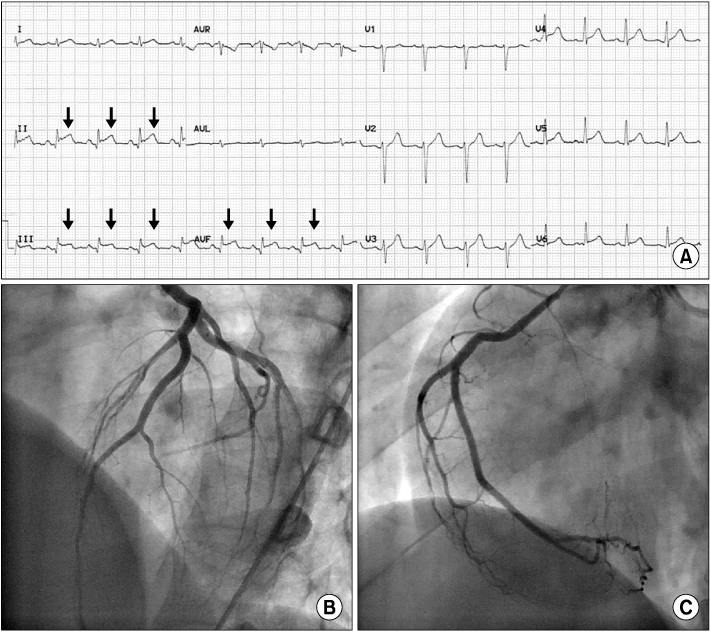
Fig. 2
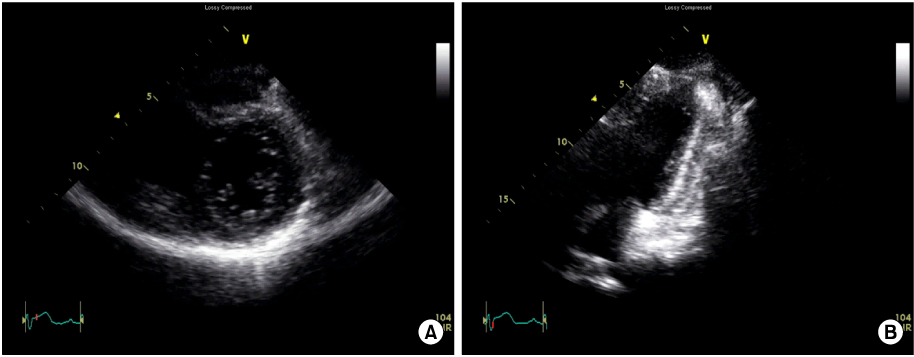
Fig. 3Radionuclide myocardial perfusion image. (A) Perfusion defect in basal to mid inferior left ventricular segment is noted at day 2. (B) Perfusion defect disappears in 2 weeks.
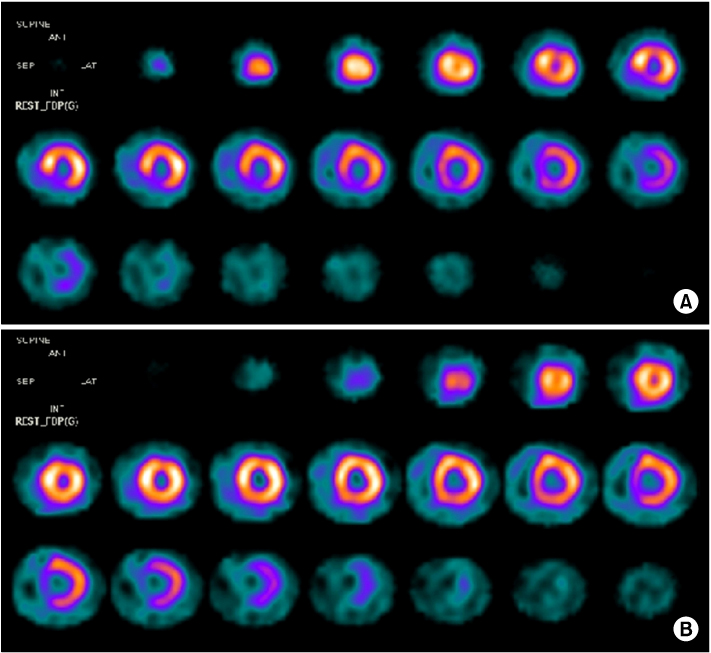
Fig. 4Two-dimensional echocardiography at day 2 showing diffuse hypokinesis of left ventricle with severe systolic dysfunction. Mild pericardial effusion is noted. (A) Parasternal short axis image. (B) Apical two chamber image (Video clip of this figure is available at
http://emj.ewhamed.ac.kr/journal/view.html?Vol=035&Num=02&page=129).
Citations
Citations to this article as recorded by