Department of Neurology, Ewha Womans University School of Medicine, Seoul, Korea.
Corresponding author: Jee Hyang Jeong. Department of Neurology, Ewha Womans University School of Medicine, 1071 Anyangcheon-ro, Yangcheon-gu, Seoul 158-710, Korea. Tel: 82-2-2650-2776, Fax: 82-2-2650-5958, jjeong@ewha.ac.kr
• Received: August 15, 2013 • Accepted: February 24, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Vertebral artery dissection (VAD) is one of important causes of posterior circulation strokes in young age patients. Typical presentations of VAD are occipital headache or posterior neck pain, with various signs arising from brainstem or cerebellar infarctions. Muscular weakness or sensory change of an ipsilateral arm owing to cervical nerve root involvement in association with the VAD has been reported very rarely. Herein we describe two unusual manifestations of extracranial VAD, which presented with monoplegia of single upper limb.
5. Hetzel A, Berger W, Schumacher M, Lucking , Dissection of. Lucking, Dissection of the vertebral artery with cervical nerve root lesions. J Neurol 1996;243:121-125.
6. Kang HG, Lee HS, Kim SS, Jeong J, Jo JH, Yi MJ, et al. Brachial plexopathy caused by vertebral artery dissection. J Korean Neurol Assoc 2011;29:64-66.
7. McGillion SF, Weston-Simons S, Harvey JR. Vertebral artery dissection presenting with multilevel combined sensorimotor radiculopathy: a case report and literature review. J Spinal Disord Tech 2009;22:456-458.
8. Tabatabai G, Schober W, Ernemann U, Weller M, Kruger R. Vertebral artery dissection presenting with ispilateral acute C5 and C6 sensorimotor radiculopathy: a case report. Cases J 2008;1:139.
9. Park KW, Park JS, Hwang SC, Im SB, Shin WH, Kim BT. Vertebral artery dissection: natural history, clinical features and therapeutic considerations. J Korean Neurosurg Soc 2008;44:109-115.
13. Rolfe B. Surgical disorders of the peripheral nerves. 2nd ed. London: Churchill Livingstone; 2011.
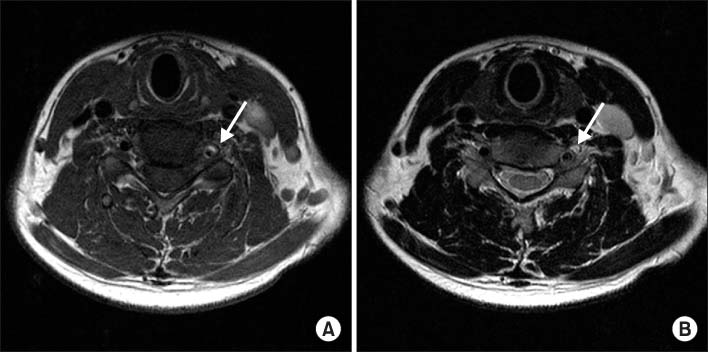
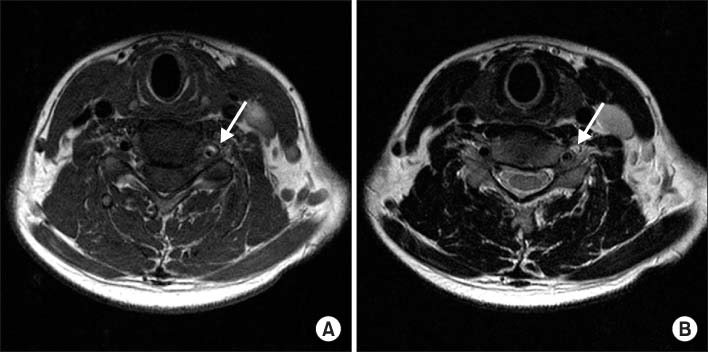
Fig. 1
(A) T1 weighted and (B) T2 weighted C-spine magnetic resonance imaging (MRI) of patient 1. Cervical MRI study shows high and isosignal intensity of the wall thickening in left vertebral artery (arrow) and combined luminal narrowing. Definite spinal cord lesion is not observed.
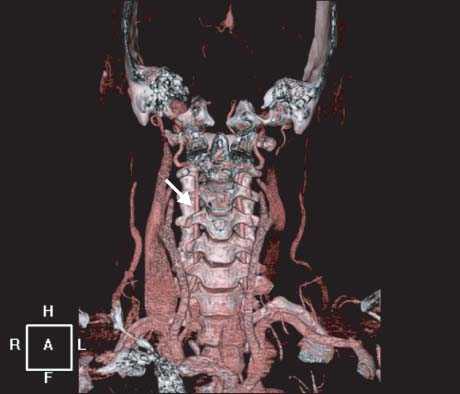
Fig. 2
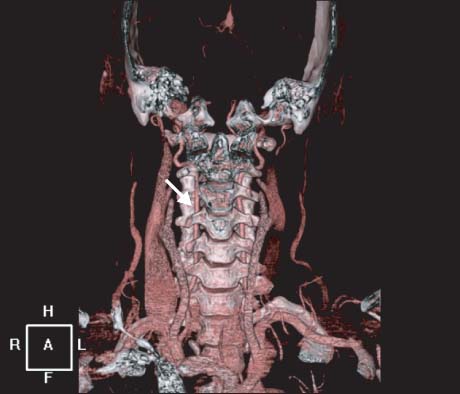
Three-dimensional computed tomography angiography of patient 1. Compared with a diameter of the right vertebral artery, left vertebral artery at the levels from the C6 to the C2 (arrow) is diffusely narrowed.
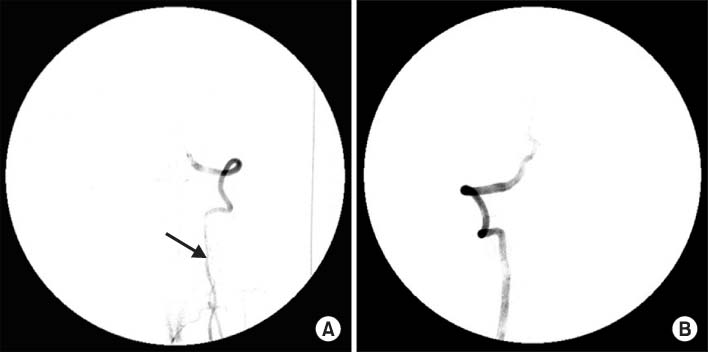
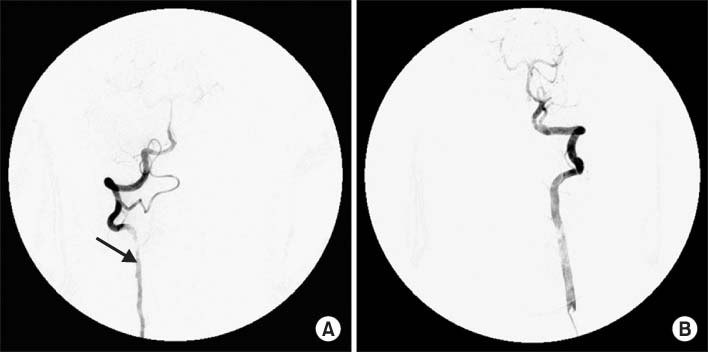
Fig. 3
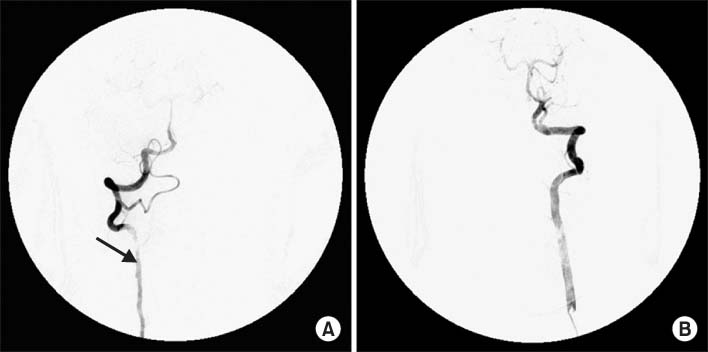
Cerebral angiography of patient 1. Cerebral 4-vessel angiography shows diffuse narrowing of left vertebral artery (A. arrow) compared with the diameter of right vertebral artery (B). These results are suggestive of left vertebral artery dissection.
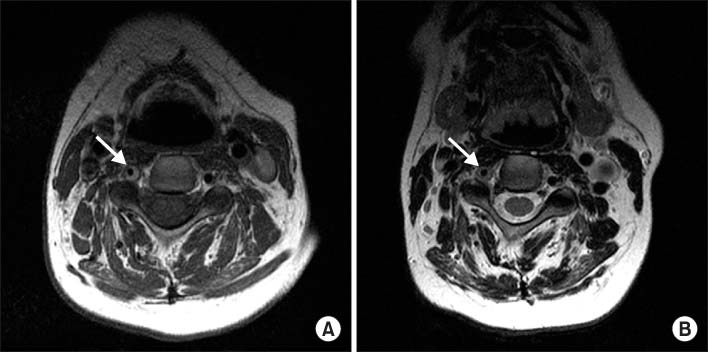
Fig. 4
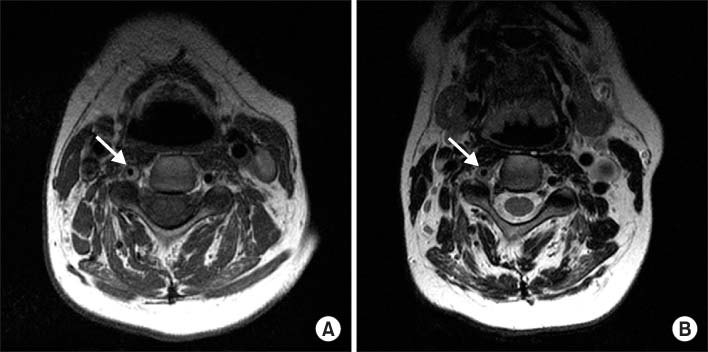
(A) T1 weighted and (B) T2 weighted cervical spine MRI images of patient 2. In T1 weighted image, signal voiding of right vertebral artery (arrow) is narrower than that of left vertebral artery. Thickening with high signal intensity (arrow) is also noted on T2 weighted image.
Fig. 5
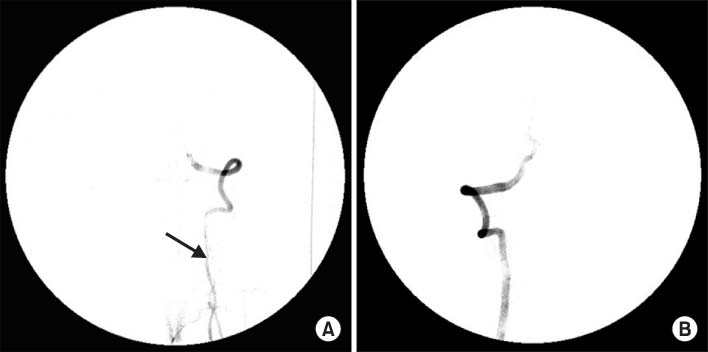
Cerebral angiography of patient 2. This study reveals the luminal irregularity and narrowing of right vertebral artery (A, arrow) compared with the diameter of left vertebral artery (B), which are compatible with the arterial dissection.
Fig. 6
Follow-up 3-dimensional computed tomography (CT) angiography of patient 2. After anticoagulation treatment, reconstructed cerebral CT angiography shows a recovery of the luminal narrowing of right vertebral artery (arrow).
Vertebral Artery Dissection Presented with Monoplegia by Cervical Radiculopathy
Fig. 1
(A) T1 weighted and (B) T2 weighted C-spine magnetic resonance imaging (MRI) of patient 1. Cervical MRI study shows high and isosignal intensity of the wall thickening in left vertebral artery (arrow) and combined luminal narrowing. Definite spinal cord lesion is not observed.
Fig. 2
Three-dimensional computed tomography angiography of patient 1. Compared with a diameter of the right vertebral artery, left vertebral artery at the levels from the C6 to the C2 (arrow) is diffusely narrowed.
Fig. 3
Cerebral angiography of patient 1. Cerebral 4-vessel angiography shows diffuse narrowing of left vertebral artery (A. arrow) compared with the diameter of right vertebral artery (B). These results are suggestive of left vertebral artery dissection.
Fig. 4
(A) T1 weighted and (B) T2 weighted cervical spine MRI images of patient 2. In T1 weighted image, signal voiding of right vertebral artery (arrow) is narrower than that of left vertebral artery. Thickening with high signal intensity (arrow) is also noted on T2 weighted image.
Fig. 5
Cerebral angiography of patient 2. This study reveals the luminal irregularity and narrowing of right vertebral artery (A, arrow) compared with the diameter of left vertebral artery (B), which are compatible with the arterial dissection.
Fig. 6
Follow-up 3-dimensional computed tomography (CT) angiography of patient 2. After anticoagulation treatment, reconstructed cerebral CT angiography shows a recovery of the luminal narrowing of right vertebral artery (arrow).
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Vertebral Artery Dissection Presented with Monoplegia by Cervical Radiculopathy