Abstract
Insulin autoimmune syndrome, a rare cause of endogenous hyperinsulinemic hypoglycemia, is characterized by insulin autoantibody, hyperinsulinemia and fasting hypoglycemia. It is well known that drugs containing a sulfhydryl group such as methimazole or α-mercaptopropionyl glycine can induce insulin autoimmune syndrome. However, insulin autoimmune syndrome caused by anti-tuberculosis treatment is very rare. We report a case of insulin autoimmune syndrome after anti-tuberculosis treatment with a review of the relevant literature.
-
Keywords: Hypoglycemia; Insulin autoimmune syndrome; Tuberculosis
Introduction
Endogenous hyperinsulinemic hypoglycemia is characterized by low blood glucose concentration due to excessive endogenous insulin secretion. Insulinoma is the most common cause of endogenous hyperinsulinemic hypoglycemia. Insulin autoimmune syndrome (IAS) is a rare cause of endogenous hyperinsulinemic hypoglycemia. IAS is also known as Hirata’s disease, because it was first reported by Hirata et al. [
1] in 1970. IAS is characterized by hypoglycemia, high serum insulin concentration, and the presence of autoantibodies to insulin or insulin receptor.
IAS has been reported to be associated with several factors including human leukocyte antigen (HLA) typing [
2] and drugs containing a sulfhydryl group such as methimazole and α-lipoic acid [
34]. Anti-tuberculosis drugs, which do not contain a sulfhydryl group, have only rarely been associated with IAS [
567]. In this report, we present a rare case of hypoglycemia caused by IAS after anti-tuberculosis treatment.
Case
A 65-year-old man presented to the emergency department with dysarthria and general weakness. He had pulmonary tuberculosis and had anti-tuberculosis treatment 30 years ago. He was diagnosed with colon cancer and underwent anterior resection 4 months ago, followed by adjuvant chemotherapy (oxaliplatin and 5-fluorouracil). At that time, an acid-fast bacillus (AFB) smear of his sputum was positive, and he started to take isoniazid, ethambutol, rifampin, and pyrazinamide. After 4 months of anti-tuberculosis treatment, the patient presented to the emergency department with acute onset of dysarthria and general weakness. At the time of admission, his serum glucose level was 41 mg/dL. Dextrose infusion improved his symptoms. He had no past history of diabetes mellitus or exposure to insulin or oral anti-diabetic drugs.
His blood pressure was 130/80 mmHg, with a pulse rate of 96 beats per minute and a respiratory rate of 20 breaths per minute. His body temperature was 36.3℃ and oxygen saturation was 98%. His height was 159.1 cm, and weight was 51.3 kg. There was no palpable goiter or thyroid mass. The cardiac and respiratory examination findings were unremarkable. The abdomen was soft and non-tender, without masses, and the bowel sound was normoactive.
The patient’s complete blood cell count showed white blood cell count of 6,240 cells/µL, hemoglobin level of 13.0 g/dL, and platelet count of 179,000 cells/µL. His biochemical profile was as follows: aspartate aminotransferase/alanine aminotransaminase 22/9 U/L, BUN/creatinine 14.3/0.7 mg/dL, total protein 7.1 g/dL, albumin 3.3 g/dL, total bilirubin 0.2 mg/dL, sodium 141 mmol/L, potassium 4.0 mmol/L, and chloride 109 mmol/L. The patient’s hemoglobin A1C level was 5.5%.
A rapid ACTH stimulation test was normal with baseline cortisol level of 14.6 µg/dL and stimulated cortisol level of 25.70 µg/dL. His thyroid stimulating hormone level was 0.242 µIU/ mL (normal range, 0.27 to 4.20 µIU/mL), free thyroxine level was 1.04 ng/dL (normal range, 0.93 to 1.71 ng/dL), triiodothyronine level was 1.07 ng/mL (normal range, 0.85 to 2.02 ng/mL).
During hospitalization, recurrent hypoglycemia was observed despite continuous intravenous administration of 10% dextrose solution. The patient’s blood glucose level was 39 mg/dL, serum insulin level was >1,000 µU/mL (normal range, 2.6 to 24.9 µU/mL), C-peptide level was 13.33 ng/mL (normal range, 1.1 to 4.4 ng/mL), insulin antibody level was 98.5% (normal range, <7.0%), and islet cell antibody was negative, suggesting endogenous hyperinsulinemia.
The brain magnetic resonance imaging and magnetic resonance angiography showed several chronic small vascular ischemic changes in both cerebrums, but there was no evidence of acute cerebral infarction or other lesion that could explain his dysarthria.
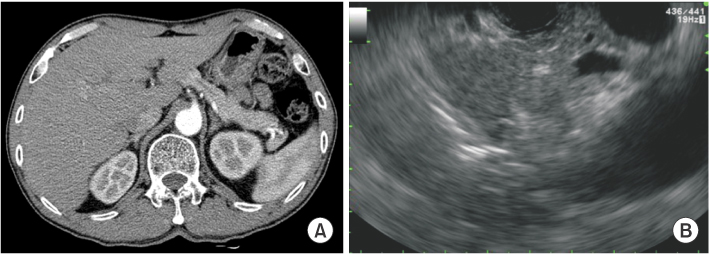
To rule out insulinoma, abdominal computed tomography and endoscopic ultrasonography were performed, but there was no intra-abdominal mass (
Fig. 1).
The patient was diagnosed with IAS. Anti-tuberculosis treatment was discontinued and daily intravenous administration of 60 mg of methylprednisolone was started. After 5 days of intravenous methylprednisolone administration, the patient no longer had hypoglycemic events. After gradually tapering the methylprednisolone, the patient was discharged on 40 mg prednisolone daily. Subsequently, the prednisolone was gradually tapered and stopped. The patient’s symptom was relieved, and there was no relapse of hypoglycemia. The patient is now being followed at an outpatient clinic. The resumption of anti-tuberculosis treatment was not considered, because his AFB smear and culture have been negative after 4 months of previous anti-tuberculosis medication.
Discussion
The prevalence of IAS is very low. From 1970 to 2013, more than 400 cases of IAS have been reported, and most cases have been made in Japan [
89]. Over 200 cases of IAS have been reported in Japan since 1970. The prevalence of IAS differs according to ethnic background, and Asian people exhibit a high prevalence [
910]. This difference may be associated with the prevalence of HLA DRB1*0406, which is higher in Asians than in Caucasians [
2]. As Woo et al. [
10] recently reported that 6% of endogenous hyperinsulinemic hypoglycemia was diagnosed with IAS in a tertiary referral center of Korea, the prevalence of IAS in Korea may be higher than previously thought. Improvements in medical technology and diagnostic methods may have contributed to the increase of IAS cases reported because idiopathic endogenous hyperinsulinemic hypoglycemia may be reclassified as IAS.
The peak age at onset was 60–69 years, and there was no predilection with respect to sex [
911]. IAS often accompanies other autoimmune disorders such as autoimmune thyroid disease and rheumatoid arthritis. Approximately 30% of patients with autoimmune thyroid disease have been reported to have insulin autoantibodies [
12].
Drugs containing a sulfhydryl group such as methimazole or α-mercaptopropionyl glycine have been cited as one of the common causes [
34911]. These drugs can interact with the disulfide bond of insulin and induce an autoimmune reaction, resulting in the formation of insulin autoantibodies [
1213]. However, anti-tuberculosis drugs did not have a sulfhydryl group. There have been only three case reports of IAS caused by anti-tuberculosis drugs worldwide, occurring mostly in the elderly [
567]. Whereas IAS has been reported to develop about 1 month after anti-tuberculosis treatment [
56], it took 4 months in our case. Among several anti-tuberculosis drugs (isoniazid, rifampin, ethambutol, and pyrazinamide), isoniazid was taken in all cases. Therefore, isoniazid is the most likely candidate for causing IAS, but the underlying mechanism of how anti-tuberculosis drugs cause IAS is unclear.
In IAS, hypoglycemia typically occurs during the late postprandial period. However, hypoglycemia can arise during fasting status, which makes it difficult to differentiate IAS from other causes of endogenous hyperinsulinemia. The mechanism by which insulin autoantibodies induce hypoglycemia in patients with IAS remains uncertain. After a meal, insulin is secreted from pancreas, but bound to insulin autoantibodies. Because insulin autoantibodies have a high binding capacity [
810], bioavailable insulin decreases triggering secretion of blizzard of insulin. And then, insulin bound to antibodies dissolved abruptly, resulting in hypoglycemia.
The duration of hypoglycemic attacks is usually short, and spontaneous remission can occur. It was reported that the duration was less than 1 month in 31%–46% of patients with IAS, and 82% of patients recovered spontaneously [
814]. In case of drug-induced IAS, hypoglycemia can be reversible when a causal drug is stopped. However, some patients need specific treatment. Frequent small meals, steroid, diazoxide, octreotide, and partial pancreatectomy have been discussed [
8], but no standard treatment was established. In our case, severe hypoglycemia continued after stopping the anti-tuberculosis treatment. Although the steroid therapy can increase the risk of activating the tuberculosis [
15], steroid therapy was attempted because of the life-threatening hypoglycemia. Fortunately, it resolved the hypoglycemia in our case. Our patient is now monitored routinely, and his tuberculosis has not been reactivated.
References
- 1. Hirata Y, Ishizu H, Ouchi N, Motomura S, Abe M, Hara Y, et al. Insulin autoimmunity in a case with spontaneous hypoglycemia. J Jpn Diabetes Soc 1970;13:312-320.
- 2. Uchigata Y, Kuwata S, Tokunaga K, Eguchi Y, Takayama-Hasumi S, Miyamoto M, et al. Strong association of insulin autoimmune syndrome with HLA-DR4. Lancet 1992;339:393-394.
- 3. Uchigata Y, Hirata Y, Iwamoto Y. Drug-induced insulin autoimmune syndrome. Diabetes Res Clin Pract 2009;83:e19-e20.
- 4. Roh E, Kim YA, Ku EJ, Bae JH, Kim HM, Cho YM, et al. Two cases of methimazole-induced insulin autoimmune syndrome in graves’ disease. Endocrinol Metab (Seoul) 2013;28:55-60.
- 5. Kim DJ, Lee JM, Lee SO, Kim NY, Lee JY, Kim HJ, et al. A case of autoimmune hypoglycemia during treatment with anti-tuberculosis drugs. Korean J Med 2008;74:574-577.
- 6. Ma WY, Won JG, Tang KT, Lin HD. Severe hypoglycemic coma due to insulin autoimmune syndrome. J Chin Med Assoc 2005;68:82-86.
- 7. Villaume C, Dollet JM, Beck B, Vaillant G, Drouin P, Debry G. Hyperinsulinemia associated with normal C-peptide levels in a woman treated with isoniazide. Biomed Pharmacother 1982;36:32-35.
- 8. Hirata Y, Uchigata Y. Insulin autoimmune syndrome in Japan. Diabetes Res Clin Pract 1994;24:Suppl. S153-S157.
- 9. Wang YL, Yao PW, Zhang XT, Luo ZZ, Wu PQ, Xiao F. Insulin autoimmune syndrome: 73 cases of clinical analysis. Chin Med J (Engl) 2015;128:2408-2409.
- 10. Woo CY, Jeong JY, Jang JE, Leem J, Jung CH, Koh EH, et al. Clinical features and causes of endogenous hyperinsulinemic hypoglycemia in Korea. Diabetes Metab J 2015;39:126-131.
- 11. Uchigata Y, Hirata Y, Iwamoto Y. Insulin autoimmune syndrome (Hirata disease): epidemiology in Asia, including Japan. Diabetol Int 2010;1:21-25.
- 12. Benson EA, Ho P, Wang C, Wu PC, Fredlund PN, Yueng RT. Insulin autoimmunity as a cause of hypoglycemia. Arch Intern Med 1984;144:2351-2354.
- 13. Ichihara K, Shima K, Saito Y, Nonaka K, Tarui S. Mechanism of hypoglycemia observed in a patient with insulin autoimmune syndrome. Diabetes 1977;26:500-506.
- 14. Uchigata Y, Eguchi Y, Takayama-Hasumi S, Omori Y. Insulin autoimmune syndrome (Hirata disease): clinical features and epidemiology in Japan. Diabetes Res Clin Pract 1994;22:89-94.
- 15. Lai CC, Lee MT, Lee SH, Lee SH, Chang SS, Lee CC. Risk of incident active tuberculosis and use of corticosteroids. Int J Tuberc Lung Dis 2015;19:936-942.
Fig. 1Images of pancreas. Abdominal computed tomography (A) and endoscopic ultrasonography (B) show no evidence of intra-abdominal mass.
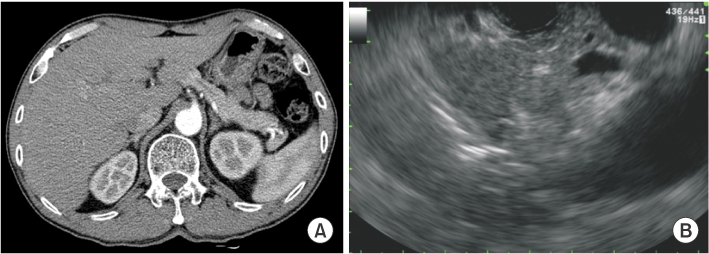
Figure & Data
Citations
Citations to this article as recorded by

- Drug-induced insulin autoimmune syndrome: a clinico-epidemiological analysis integrating pharmacovigilance data and case series
Xiuheng Yu, Min Li, Yi Liao, Yuqing Xie, Jing Xu, Youqi Long, Shixin Xiang
Diabetology & Metabolic Syndrome.2025;[Epub] CrossRef - Insulin Autoimmune Syndrome: A Systematic Review
MingXu Lin, YuHua Chen, Jie Ning, Tatsuya Kin
International Journal of Endocrinology.2023; 2023: 1. CrossRef - An Unusual Cause of Hypoglycemia: Insulin Autoimmune Syndrome
Yasemin AYDOĞAN ÜNSAL, Özen ÖZ GÜL, Soner CANDER, Canan ERSOY, Oktay ÜNSAL, Ensar AYDEMİR, Erdinç ERTÜRK
Turkish Journal of Internal Medicine.2021; 3(1): 30. CrossRef - Effects of Co‐administration of Sulfonylureas and Antimicrobial Drugs on Hypoglycemia in Patients with Type 2 Diabetes Using a Case‐Crossover Design
Sera Lee, Miyoung Ock, Hun‐Sung Kim, Hyunah Kim
Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy.2020; 40(9): 902. CrossRef - Insulin autoimmune syndrome: A rare cause of hypoglycemia
Tejas M. Maheshwari, Anurag Sharma, Bhagwani Bai Maheshwari
Journal of Family Medicine and Primary Care.2020; 9(9): 5046. CrossRef - Rare Cause of Recurrent Hypoglycemia: Insulin Autoimmune Syndrome
Rungsima Tinmanee, Rungpailin Buranagan, Sirirat Ploybutr, Raweewan Lertwattanarak, Apiradee Sriwijitkamol
Case Reports in Endocrinology.2017; 2017: 1. CrossRef - Isoniazid
Reactions Weekly.2017; 1634(1): 169. CrossRef