1Department of Rehabilitation Medicine, Ewha Womans University Mokdong Hospital, Ewha Womans University College of Medicine, Seoul, Korea
*Corresponding author: Jee Hyun Suh,
Department of Rehabilitation Medicine, Ewha Womans University Mokdong Hospital,
Ewha Womans University College of Medicine, 1071 An-Yang-Cheon Ro, Yang-Cheon
Gu, Seoul 07985, Korea, E-mail: jeehyun.suh1@gmail.com
• Received: December 10, 2024 • Revised: December 18, 2024 • Accepted: January 6, 2025
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Objectives: This study aimed to evaluate the effectiveness of a
multidisciplinary pulmonary rehabilitation program at Ewha Womans University
Mokdong Hospital, Korea that was designed to augment respiratory function,
promote patient recovery, and improve discharge outcomes.
Methods: This study was conducted as part of quality improvement
activities from March to August 2023. A multidisciplinary pulmonary
rehabilitation team was established, comprising specialists in rehabilitation
medicine, pulmonology, and thoracic surgery, as well as physical and
occupational therapists, and the nutrition team. We developed a comprehensive
rehabilitation program that included stretching, strengthening exercises,
aerobic training, and respiratory retraining, supplemented by individualized
treatments such as bedside and ambulatory physical therapy. Evaluations before
and after rehabilitation were performed using the Modified Medical Research
Council Dyspnea Scale and the Chronic Obstructive Pulmonary Disease Assessment
Test. The primary indicators of success were an increase of over 10% in
pulmonary rehabilitation consultations and an improvement in discharge-to-home
rates.
Results: The total number of pulmonary rehabilitation cases rose by
79.16%, from 24 to 43, while consultations saw a 21.15% increase, from 52 to 63.
Of the 63 pulmonary rehabilitation cases, 32 (50.8%) were transferred to other
hospitals, 25 (39.7%) were discharged home, and 6 (9.5%) remained
hospitalized.
Conclusion: The study demonstrated the effectiveness of a
multidisciplinary pulmonary rehabilitation approach in improving program
participation and achieving meaningful discharge outcomes. These findings
underscore the potential for expanding multidisciplinary efforts and highlight
the need for further studies to increase discharge-to-home rates and evaluate
the long-term impacts of such programs.
Pulmonary rehabilitation is a critical therapeutic and rehabilitative process
aimed at improving and maintaining respiratory function. It encompasses a
comprehensive and intensive treatment approach that includes education, various
techniques, and devices to alleviate and manage symptoms of respiratory
diseases, as well as to help prevent complications associated with these
disorders. Pulmonary rehabilitation enhances respiratory function, strengthens
respiratory muscles, and improves breathing techniques, ultimately optimizing
oxygen delivery. The goal of pulmonary rehabilitation is to enhance
patients' physical capacity and psychological stability, enabling them to
achieve optimal functional performance in their daily lives.
Pulmonary rehabilitation is particularly crucial for patients with diminished
respiratory capacity, including those suffering from chronic obstructive
pulmonary disease, restrictive lung disease, tuberculosis-related lung
conditions, or pulmonary arterial hypertension. It is equally crucial for
patients recovering from lung cancer surgery, lung volume reduction surgery, or
thoracic surgery, as well as for those in intensive care units. Although
pulmonary rehabilitation has been proven effective in treating various
respiratory diseases, its application in clinical practice is still not
widespread [1–3]. Research on the current state and development of
pulmonary rehabilitation in clinical settings has been conducted in several
countries, including the United States. However, in Korea, such research is
scarce, primarily due to a lack of awareness about the program [4–9]. A 2011 study revealed that only 20.9% of institutions in Korea
offered pulmonary rehabilitation [9].
However, since 2017, when the National Health Insurance Service (NHIS) began
covering pulmonary rehabilitation, there has been an increase in its
institutional implementation [10].
Despite this progress, the practice is mainly carried out by departments of
internal medicine or rehabilitation medicine, without a comprehensive,
multidisciplinary approach. At the tertiary university hospital where this study
was conducted, there were only 26 multidisciplinary pulmonary rehabilitation
consultations in the six months prior to the study, from March to August
2022.
Objectives
The aim of this study was to evaluate the effectiveness of a pulmonary
rehabilitation program, which involves a multidisciplinary team comprising
individuals from the departments of rehabilitation medicine, respiratory
medicine, thoracic surgery, and the nutrition team.
Methods
Ethics statement
This study evaluates a new program in the Department of Rehabilitation at Ewha
Medical University Mokdong Hospital. Only the number of patients was counted
from the electronic medical records; therefore, neither approval by the
institutional review board nor informed consent was required.
Study design
This was a case series analysis.
Setting
This study was carried out as part of the 2023 Quality Improvement (QI)
activities at Ewha Womans University Mokdong Hospital. It targeted inpatients at
the hospital from March to August 2023.
Subjects were patients who participated in the pulmonary rehabilitation program
from March to August 2023.
Interventions
Multidisciplinary pulmonary rehabilitation program
To establish a multidisciplinary pulmonary rehabilitation program, a
dedicated team was formed that included physicians from the Departments of
Rehabilitation Medicine, Pulmonology, and Thoracic Surgery, along with
physical therapists, occupational therapists, and nutritionists. Efforts to
promote this team were implemented throughout the hospital to enhance
awareness of the multidisciplinary approach to pulmonary rehabilitation. As
part of these promotional efforts, the program was highlighted as the theme
for the hospital's 2023 QI activities. Information about the program
was disseminated within the hospital to increase visibility. Additionally,
networking opportunities and collaborative meetings were organized to foster
stronger cooperation among the medical staff from the departments of
pulmonology, rehabilitation medicine, and thoracic surgery.
Furthermore, a comprehensive respiratory rehabilitation program was
developed, incorporating various components including stretching,
strengthening exercises, aerobic exercise, respiratory retraining, and
equipment-based training. Rehabilitation treatments were tailored to each
patient's condition, offering diverse approaches such as bedside
pulmonary physical therapy and ambulatory physical therapy. Additionally,
regular multidisciplinary patient meetings and follow-up consultations were
conducted.
An evaluation protocol for pre- and post-rehabilitation therapy was
established. Specifically, the protocol was enhanced by including not only
the conventional manual muscle test but also the Modified Medical Research
Council (mMRC) Dyspnea Scale and the Chronic Obstructive Pulmonary Disease
Assessment Test (CAT). This enhancement facilitated a more comprehensive
evaluation and treatment of respiratory conditions.
Outcomes
The key indicators for this QI activity were defined as an increase of more than
10% in the number of pulmonary rehabilitation consultations compared to the same
period in the previous year, and an enhancement in the discharge-to-home
rate.
Data sources/measurement
Data were obtained from the electronic medical records of pulmonary
rehabilitation cases before and after the introduction of the multidisciplinary
pulmonary rehabilitation program. The patient count was recorded.
Bias
Bias was not considered reportable because the findings were derived from
electronic medical records before and after the intervention.
Study size
All patients were included during the observational period; no sample size
estimation was conducted.
Statistical methods
A descriptive analysis was conducted to compare the total number of pulmonary
rehabilitation cases before and after the intervention.
Results
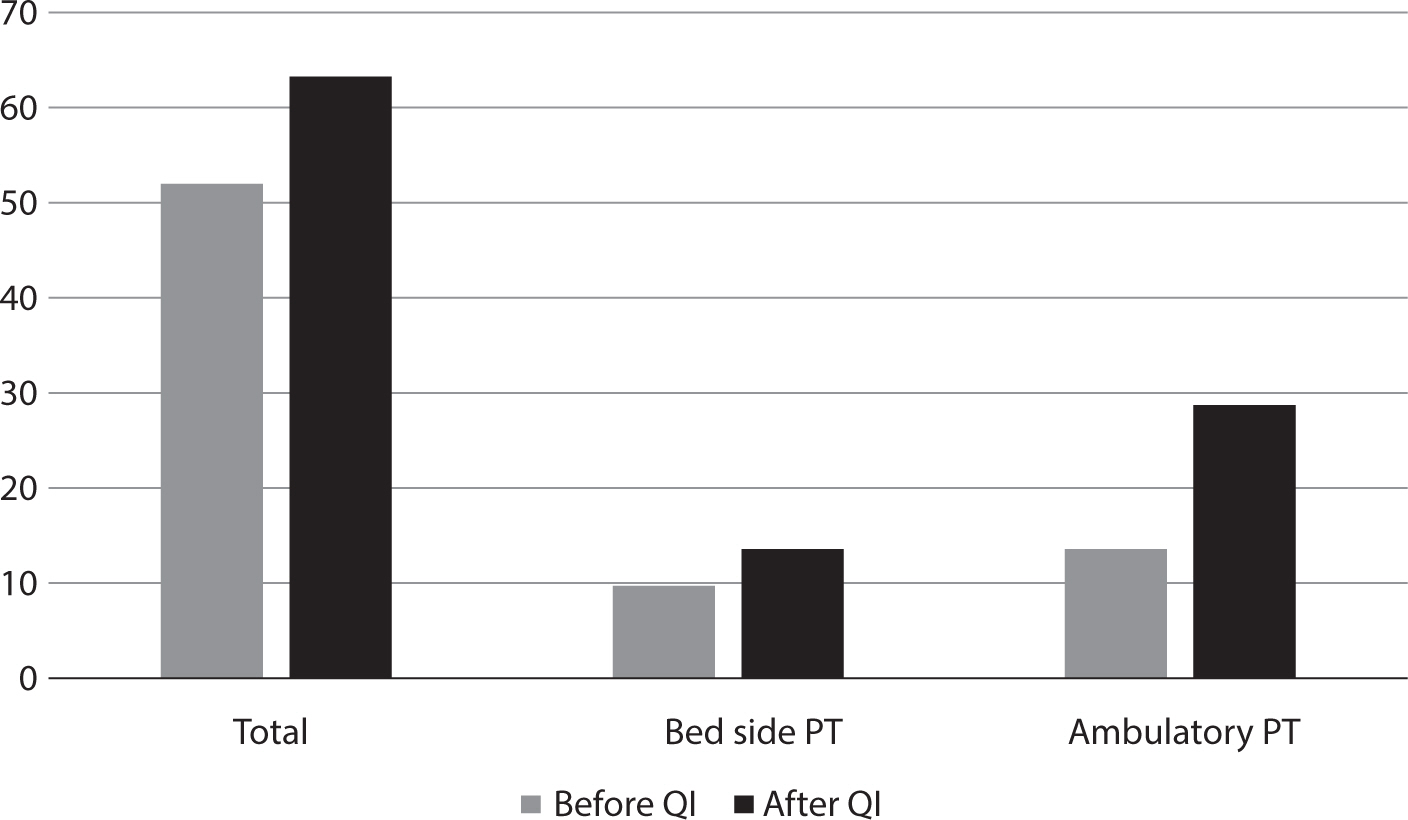
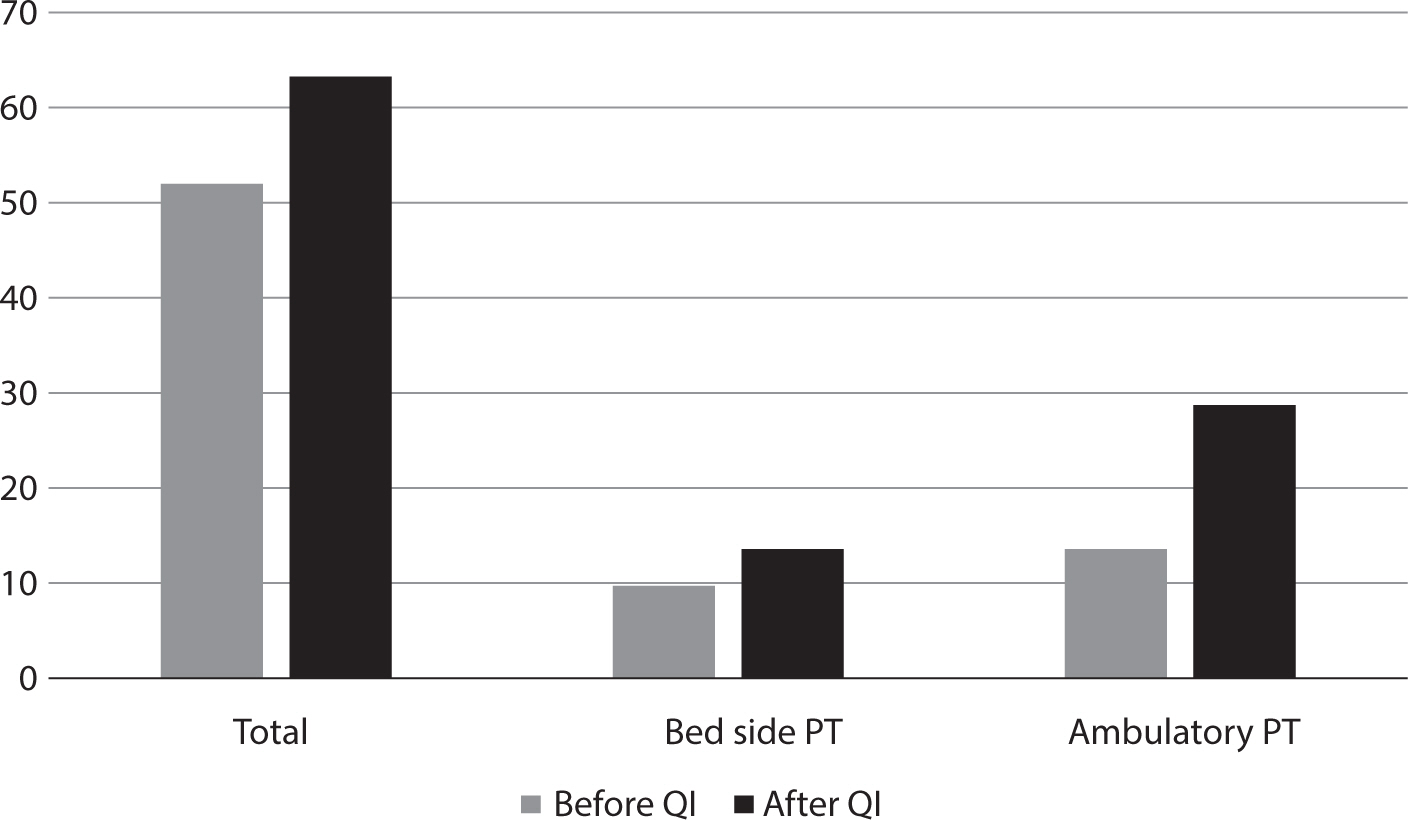
As a result of this QI activity, the total number of pulmonary rehabilitation cases
increased by 79.16%, from 24 to 43 cases, and the number of pulmonary rehabilitation
consultations rose by 21.15%, from 52 to 63 cases (Fig. 1). Of the 63 pulmonary rehabilitation cases, 32 (50.8%) were
transferred to other hospitals, 25 (39.7%) were discharged home, and 6 (9.5%)
remained hospitalized.
Fig. 1.
The number of pulmonary rehabilitation consultations and the number of
bedside and ambulatory pulmonary rehabilitation cases. PT, physical therapy;
QI, quality improvement.
Discussion
Key results
The number of pulmonary rehabilitation consultations exceeded the target of a 10%
increase, reaching a 21.15% increase and thereby achieving the goal.
Interpretation/comparison with previous studies
There was a significant increase of over 20% compared to 2022, a year that
already had a high number of respiratory-related inpatient cases due to
COVID-19. Additionally, this initiative provided an opportunity to enhance
awareness of the importance of pulmonary rehabilitation among other healthcare
professionals in the hospital, who previously had limited understanding of its
significance.
As of 2019, approximately 6,200 people in Korea died annually from chronic lower
respiratory diseases, which accounted for 2.1% of all deaths [11]. The mortality rate for these diseases
was 12.0 per 100,000 population, ranking them 9th among causes of death [11]. According to the World Health
Organization (WHO), chronic diseases are responsible for 71% of deaths globally,
with chronic respiratory diseases contributing to 5% of the total. This
indicates that chronic respiratory diseases account for 7% of deaths
attributable to chronic diseases worldwide [12]. The prevalence and mortality rates of respiratory diseases are
on the rise. Pulmonary rehabilitation is crucial in managing chronic lung
diseases and offers significant benefits. These include reducing exercise
intolerance, improving health-related quality of life, and alleviating dyspnea.
It is recognized as a highly effective therapeutic approach for enhancing the
overall well-being of patients with respiratory conditions [13]. A 2011 study in Korea found that only
20.9% of 43 tertiary and general hospitals offered pulmonary rehabilitation
[9]. When implemented, most programs
focused primarily on respiratory education, and it was very rare for them to
include the high-intensity pulmonary rehabilitation programs recommended by
guidelines [10]. However, pulmonary
rehabilitation should encompass more than just respiratory education. It should
also include exercise training, behavioral modifications, and education aimed at
improving both the physical and psychological conditions of patients with
chronic respiratory diseases.
According to the "Evaluation of the Effects and Improvement Plans for the
Phase 2 Pilot Program of Rehabilitation Medical Institution Fees"
conducted by the Health Insurance Review and Assessment Service (HIRA) in 2022,
the discharge-to-home rates were 66.1% for moderate patients, 39.8% for severe
patients, and 13.4% for very severe patients [14]. This study also included patients from the intensive care unit,
which likely influenced the overall discharge-to-home rate, estimated at
39.7%.
Limitations
First, the duration of the study was limited to only six months, which hindered a
clear evaluation of its long-term effects. Future research should extend over a
longer period, ideally on an annual basis. Second, there is a growing trend in
international studies toward outpatient or home-based pulmonary rehabilitation.
Consequently, future studies should concentrate on enhancing the quality of
home-based pulmonary rehabilitation for outpatient patients. Third, the study
did not evaluate quality of life, depression, or anxiety, focusing solely on
mMRC and CAT scores. Additional research in these areas would be valuable.
Conclusion
This study demonstrated a 79.16% increase in total pulmonary rehabilitation
cases, rising from 24 to 43, and a 21.15% increase in consultations, from 52 to
63, surpassing the target of a 10% improvement. However, the discharge-to-home
rate was 39.7%, which was lower than the 50.8% transfer-to-other-hospitals rate.
This indicates that while the multidisciplinary pulmonary rehabilitation
approach effectively increased participation, further efforts are necessary to
improve discharge-to-home outcomes. The significance of this study lies in its
implementation of a comprehensive, multidisciplinary approach to pulmonary
rehabilitation. Future interventions should focus on early rehabilitation and
targeted strategies to facilitate transitions back to home environments, which
could potentially improve these outcomes.
Authors' contributions
Project administration: Suh JH
Conceptualization: Han SJ, Suh JH
Methodology & data curation: Suh JH
Funding acquisition: not applicable
Writing – original draft: Suh JH
Writing – review & editing: Han SJ, Suh JH
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Foster S, Thomas HM 3rd. Pulmonary rehabilitation in lung disease other than chronic
obstructive pulmonary disease. Am Rev Respir Dis 1990;141(3):601-604.
2. Holland AE, Wadell K, Spruit MA. How to adapt the pulmonary rehabilitation programme to patients
with chronic respiratory disease other than COPD. Eur Respir Rev 2013;22(130):577-586.
3. Rokach A, Romem A, Arish N, Azulai H, Chen C, Bertisch M, et al. The effect of pulmonary rehabilitation on non-chronic obstructive
pulmonary disease patients. Isr Med Assoc J 2019;21(5):326-329.
4. Brooks D, Sottana R, Bell B, Hanna M, Laframboise L, Selvanayagarajah S, et al. Characterization of pulmonary rehabilitation programs in Canada
in 2005. Can Respir J 2007;14(2):87-92.
6. Garvey C, Casaburi R, Spruit MA, De Brandt J. Survey of exercise prescription in US pulmonary rehabilitation
programs. J Cardiopulm Rehabil Prev 2020;40(2):116-119.
9. Lee YS, Park YB, Oh YM, Lee SD. Survey on the reality of pulmonary rehabilitation in
Korea. Obstr Lung Dis 2013;(1):4-7.
10. Kim HJ, Choi HE, Jang HJ, Kim HK, Park JH, Lee JH, et al. Current status and trends of pulmonary rehabilitation in South
Korea: national level data analysis using Health Insurance Review and
Assessment Service (HIRA) database from 2016 to 2018. Medicine 2022;101(41):e31085.
11. GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence,
disability-adjusted life years, and years lived with disability for chronic
obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis
for the Global Burden of Disease Study 2015. Lancet Respir Med 2017;5(9):691-706.
14. Shin HI, Oh IH, Kim DA, Kim TW, Kim HB, You SD, et al. Evaluation of the effects and improvement plans for the phase 2 pilot
program of rehabilitation medical institution fees. Wonju: Health Insurance Review and Assessment Service
(HIRA); 2022.
Figure & Data
References
Citations
Citations to this article as recorded by
Knowledge and perception of pulmonary rehabilitation among physicians and physiotherapists in Southwest Nigeria: A mixed-method study Adebayo Ishola Omileye, Al-Furqan Abimbola Akinnibosun, Chioma Favour Enuma, Nse Odunaiya Journal of the Pan African Thoracic Society.2026; 0: 1. CrossRef
Effectiveness of a multidisciplinary pulmonary rehabilitation program
at Ewha Womans University Mokdong Hospital, Korea
Fig. 1.
The number of pulmonary rehabilitation consultations and the number of
bedside and ambulatory pulmonary rehabilitation cases. PT, physical therapy;
QI, quality improvement.
Fig. 1.
Effectiveness of a multidisciplinary pulmonary rehabilitation program
at Ewha Womans University Mokdong Hospital, Korea