
Department of Neurology, Ewha Womans University School of Medicine, Seoul, Korea
1Departments of Neurology, Yonsei University College of Medicine, Seoul, Korea
2Department of Neurology, Hallym University College of Medicine, Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea
33Department of Neurology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
Copyright © 2017 Ewha Womans University School of Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
| Variable | Causes for other determined etiology (n=37) |
|---|---|
| Arterial dissection | 21 (56.8) |
| Extracranial internal carotid artery | 8 (21.6) |
| Intracranial internal carotid artery* | 1 (2.7) |
| Extracranial vertebral artery | 6 (16.2) |
| Intracranial vertebral artery | 3 (8.1) |
| Middle cerebral artery | 3 (8.1) |
| Vasculitis meningitis | 4 (10.8) |
| Moyamoya diseases | 4 (10.8) |
| Takayasu’s diseases | 3 (8.1) |
| Systemic lupus erythematosus | 3 (8.1) |
| Sneddon’s syndrome | 1 (2.7) |
| Familial protein C, S deficiency | 1 (2.7) |
| Variable | mRS<3 (n=95) | mRS≥3 (n=27) | Total (N=122) | P-value | |
|---|---|---|---|---|---|
| Male sex | 61 (64.2) | 15 (55.6) | 76 (62.3) | 0.413 | |
| Age (yr) | 25.1±3.8 | 24.8±3.3 | 25.1±3.7 | 0.646 | |
| Risk factor | |||||
| Hypertension | 12 (12.6) | 3 (11.1) | 15 (12.3) | 0.832 | |
| Diabetes mellitus | 1 (1.1) | 0 | 1 (0.8) | 0.592 | |
| Dyslipidemia | 8 (8.4) | 0 | 8 (6.6) | 0.119 | |
| Smoking | 45 (47.4) | 9 (33.3) | 54 (44.3) | 0.195 | |
| Regular alcohol intake | 23 (24.2) | 7 (25.9) | 30 (24.6) | 0.855 | |
| Recent alcohol intake | 8 (8.4) | 0 | 8 (6.6) | 0.126 | |
| Atrial fibrillation | 2 (2.1) | 5 (18.5) | 7 (5.7) | 0.001 | |
| Occupation situation | 0.140 | ||||
| Without routine job | 13 (13.7) | 7 (25.9) | 20 (16.4) | ||
| White collar | 37 (38.9) | 4 (18.9) | 41 (33.6) | ||
| Soldier | 22 (23.2) | 6 (22.2) | 28 (23.0) | ||
| Student | 20 (21.1) | 9 (33.3) | 29 (23.8) | ||
| Blue collar | 3 (3.2) | 1 (3.7) | 4 (3.3) | ||
| Activity at stroke occurrence | 0.183 | ||||
| Resting | 68 (71.6) | 23 (85.2) | 91 (74.6) | ||
| Vigour activity | 17 (17.9) | 1 (3.7) | 18 (14.8) | ||
| Wake-up stroke | 10 (10.5) | 3 (11.1) | 13 (10.7) | ||
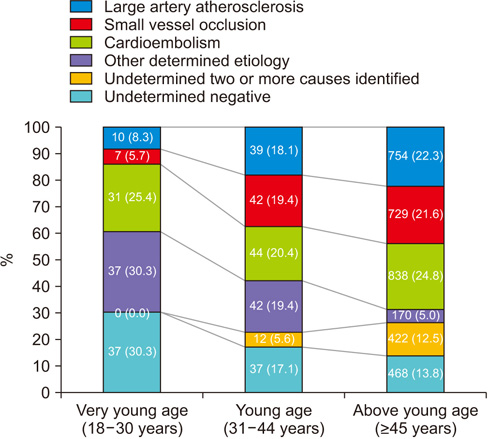
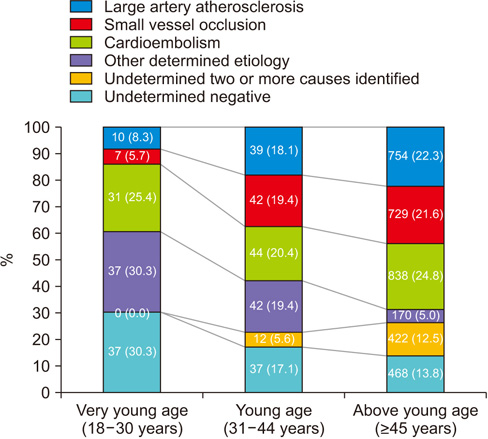
| Stroke classification | 0.028 | ||||
| Large artery atherosclerosis | 8 (8.4) | 2 (7.5) | 10 (8.3) | ||
| Small vessel occlusion | 7 (7.4) | 0 | 7 (5.7) | ||
| Cardioembolism | 18 (18.9) | 13 (48.1) | 31 (25.4) | ||
| Other determined etiology | 30 (31.6) | 7 (25.9) | 37 (30.3) | ||
| Undetermined negative | 32 (33.7) | 5 (18.5) | 37 (30.3) | ||
| NIHSS | 3 (1–5) | 12 (9–14) | 4 (2–8) | 0.001 | |
| Variable | Causes for other determined etiology (n=37) |
|---|---|
| Arterial dissection | 21 (56.8) |
| Extracranial internal carotid artery | 8 (21.6) |
| Intracranial internal carotid artery |
1 (2.7) |
| Extracranial vertebral artery | 6 (16.2) |
| Intracranial vertebral artery | 3 (8.1) |
| Middle cerebral artery | 3 (8.1) |
| Vasculitis meningitis | 4 (10.8) |
| Moyamoya diseases | 4 (10.8) |
| Takayasu’s diseases | 3 (8.1) |
| Systemic lupus erythematosus | 3 (8.1) |
| Sneddon’s syndrome | 1 (2.7) |
| Familial protein C, S deficiency | 1 (2.7) |
| Variable | Adjusted OR (95% confidence interval) | P-value |
|---|---|---|
| Male sex | 1.41 (0.56–3.54) | 0.455 |
| Age (yr) | 0.96 (0.84–1.09) | 0.564 |
| NIHSS | 2.94 (1.61–5.37) | 0.001 |
| Stroke subtype | ||
| Large artery atherosclerosis | 1.53 (0.23–9.91) | 0.652 |
| Small vessel occlusion | No case | |
| Cardioembolism | 4.68 (1.42–15.48) | 0.011 |
| Other determined etiology | 1.37 (0.38–4.86) | 0.626 |
| Undetermined negative | Reference |
Values are presented as mean±standard deviation, number (%), or median (interquartile range). mRS, modified Rankin scale at 3 months after index stroke; NIHSS, National Institute of Health Stroke Scale.
Values are presented as number (%). One patient had both right intracranial internal carotid artery and middle cerebral artery dissection.
mRS, modified Rankin scale; OR, odds ratio; NIHSS, National Institute of Health Stroke Scale.
