1Division of Critical Care Medicine, Department of Surgery, Ewha Womans University Mokdong Hospital, Ewha Womans University College of Medicine, Seoul, Korea
2Division of Colorectal Surgery, Department of Surgery, Ewha Womans University College of Medicine, Seoul, Korea
*Corresponding author: Ryung-Ah Lee,
Division of Colorectal Surgery, Department of Surgery, Ewha Womans University
College of Medicine, 260 Gonghang-daero, Gangseo-gu, Seoul 07804, Korea E-mail:
ralee@ewha.ac.kr
• Received: May 12, 2024 • Accepted: April 18, 2024
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
The capabilities of artificial intelligence (AI) have recently surged, largely
due to advancements in deep learning inspired by the structure and function of
the neural networks of the human brain. In the medical field, the impact of AI
spans from diagnostics and treatment recommendations to patient engagement and
monitoring, considerably improving efficiency and outcomes. The clinical
integration of AI has also been examined in specialties, including pathology,
radiology, and oncology. General surgery primarily involves manual manipulation
and includes preoperative, intraoperative, and postoperative care, all of which
are critical for saving lives. Other fields have strived to utilize and adopt
AI; nonetheless, general surgery appears to have retrogressed. In this review,
we analyzed the published research, to understand how the application of AI in
general surgery differs from that in other medical fields. Based on previous
research in other fields, the application of AI in the preoperative stage is
nearing feasibility. Ongoing research efforts aim to utilize AI to improve and
predict operative outcomes, enhance performance, and improve patient care.
However, the use of AI in the operating room remains significantly understudied.
Moreover, ethical responsibilities are associated with such research,
necessitating extensive work to gather evidence. By fostering interdisciplinary
collaboration and leveraging lessons from AI success stories in other fields, AI
tools could be specifically tailored for general surgery. Surgeons should be
prepared for the integration of AI into clinical practice to achieve better
outcomes; therefore, the time has come to consider ethical and legal
implications.
Artificial intelligence (AI) has emerged as a revolutionary force in modern medicine,
significantly reshaping diagnostics and treatment planning across various
specialties [1,2]. In fields such as radiology and oncology, AI has had an unmistakable
impact on improving diagnostic accuracy, enabling early disease detection, and
optimizing treatment protocols [3,4]. For instance, in radiology, AI algorithms
have revolutionized image analysis, facilitating more accurate interpretations and
aiding in the early detection of illnesses [5].
The scope of AI integration ranges from diagnostics to patient management and care.
Predictive analytics utilizing sophisticated machine learning (ML) algorithms are
increasingly being employed to identify high-risk patients, predict complications,
and personalize care plans [6]. This approach
has ushered in a new era of proactive, patient-centric healthcare.
Moreover, AI is paving the way for precision medicine. By analyzing large datasets
that include genetic profiles and patient histories, AI systems can provide
treatments specifically tailored to the needs of individual patients. This approach
significantly improves therapeutic effectiveness and minimizes side effects [7].
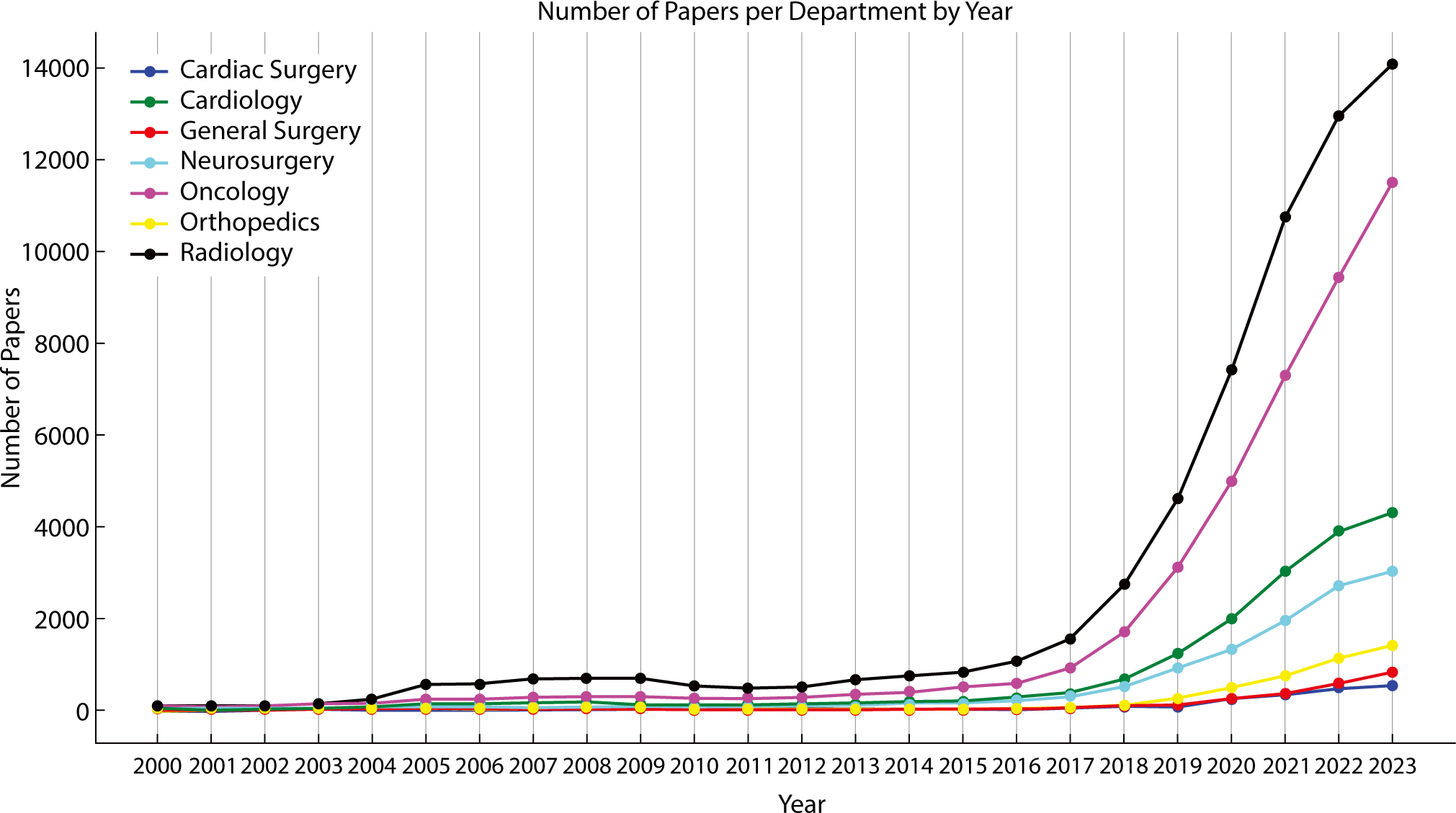
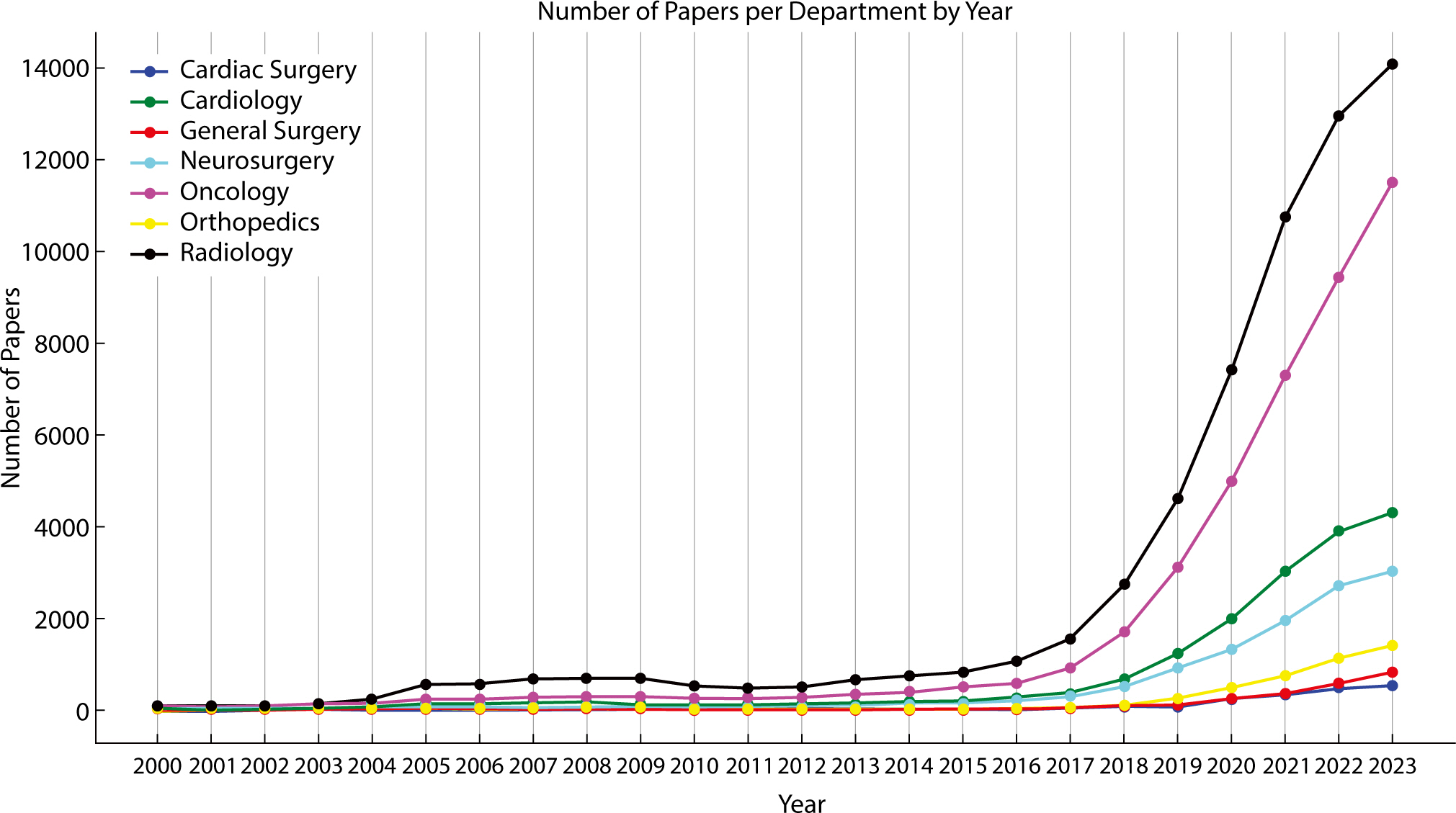
Despite these advances, general surgery lags significantly behind other medical
fields in both AI research and clinical applications. The volume of medical articles
published on the use of AI is markedly lower in the field of surgery, especially in
general surgery (Fig. 1).
Fig. 1.
Number of artificial intelligence papers published by each specialty from
2000 to 2023 is depicted.
While specialized fields such as neurosurgery and cardiology are increasingly
incorporating AI to improve surgical planning and robotic assistance, general
surgery has been notably slower in adopting these advanced technologies [8,9].
The reasons for this delay are multifactorial. One of these reasons relates to the
diversity and spontaneity of surgical procedures. General surgery is a dynamic field
where some operations are predictable and can be scheduled in advance, while others
are unpredictable and often rely on real-time decision-making in the operating room
[10]. The variability in case types
within general surgery complicates the collection of the extensive and consistent
data necessary to train AI systems [10]. This
issue is further exacerbated by the relative scarcity of focused research efforts
aimed at integrating AI into general surgical workflows [10]. Therefore, locating studies on the use of AI in general
surgery within databases like PubMed proves challenging.
This article summarizes the current state of research on the application of AI in
medicine and explores the future direction of general surgery as it adapts to a
rapidly changing medical environment. It includes a discussion on how AI can be
integrated into various aspects of general surgery, ranging from preoperative
analytics to postoperative care, as well as the steps required to overcome existing
challenges.
Ethics statement
It is a literature database-based review; therefore, neither approval by the
institutional review board nor obtainment of informed consent was required.
Pioneering artificial intelligence in the medical specialties of radiology,
oncology, and cardiology
In modern medicine, the integration of AI has been particularly pronounced in
specialties such as radiology, oncology, and cardiology. In radiology, AI algorithms
have revolutionized diagnostic processes and enhanced the accuracy of image
interpretation, which is crucial for early disease detection and treatment
planning.
Recent studies on AI in radiology have produced important findings. Lång et
al. compared the clinical safety of an AI-assisted screen reading protocol to that
of the conventional double reading method used in mammography screening. The study
involved 80,000 women and assessed early screening outcomes, including cancer
detection rates, retest rates, false-positive rates, positive predictive values of
the retests, and the types of cancers detected. In the intervention group, 244
tumors were detected, comprising 184 invasive tumors and 60 in situ
tumors. Meanwhile, in the control group, 203 tumors were identified, with 165 being
invasive and 38 in situ [11].
A randomized controlled trial conducted by Nam et al. demonstrated that AI-based,
computer-aided design software enhances the detection rate of actionable lung
nodules in chest radiographs of health-screening participants. The AI group
exhibited a higher detection rate of actionable nodules compared to the non-AI group
(0.59% vs. 0.25%). Additionally, the detection rate of malignant lung nodules was
also higher in the AI group than in the non-AI group (0.15% vs. 0.0%). The rates of
misdiagnosis and positive reporting were similar between the AI and non-AI groups
[12].
Sachpekidis et al. have demonstrated that a deep learning (DL)-based tool for
automatically assessing bone marrow metabolism in patients with multiple myeloma is
feasible and correlates with clinically relevant disease parameters. There is a
significant positive correlation between the visual analysis of PET/CT scans and the
metabolic tumor volume (MTV) and total lesion glycolysis (TLG) values, following the
application of all six 18F-fluorodeoxyglucose (FDG) uptake thresholds.
Additionally, significant differences in MTV and TLG values were observed between
patient groups across all applied thresholds.
The DL-based approach has demonstrated significant, moderate, positive correlations
between bone marrow plasma cell infiltration and plasma β2-microglobulin
levels, as well as with the automated quantitative PET/CT parameters, MTV and TLG
[13].
Similarly, oncology has benefited from the use of AI, especially in the realm of
personalized medicine. AI algorithms are employed to analyze patient data and
predict responses to treatment, which allows oncologists to customize therapies
based on the specific needs of individual patients. Clift et al. developed a
clinically useful model that estimates the 10-year risk of breast cancer-related
mortality for women at all stages of the disease. Additionally, they compared the
outcomes of regression analyses with those of ML approaches. The final Cox model
demonstrated good discriminatory power, evidenced by a Harrell’s C-index of
0.858 (95% CI, 0.853–0.864), and showed moderate calibration. The
model's performance varied across ethnic groups, exhibiting the highest
discriminatory power in Chinese women (Harrell’s C-index=0.931) and the
lowest in Bangladeshi women (Harrell’s C-index=0.794). Moreover, the model
generally performed well across various cancer stages, though its discriminatory
power decreased as the cancer stage advanced [14].
Alaimo et al. have developed and validated a ML model to predict the early recurrence
of intrahepatic cholangiocarcinoma following hepatectomy. The model, trained using
14 clinicopathological characteristics, demonstrates promising accuracy in
predicting recurrences occurring within 12 months after surgery. It identifies tumor
burden score as the most significant predictor of early recurrence, followed by
perineural involvement. Additionally, the model's predictions of early
recurrence strongly correlate with 3-year overall survival rates. Patients predicted
to experience early recurrence exhibit significantly lower 3-year overall survival
rates compared to those without such predictions [15]. A meta-analysis utilizing a substantial volume of recent data has
been conducted to assess the effectiveness of AI in diagnosing lung cancer. The
findings indicate that AI-assisted diagnostic systems achieve a sensitivity and
specificity of 0.87, with a missed diagnosis rate and misdiagnosis rate each at 13%.
The systems also show a positive likelihood ratio of 6.5, a negative likelihood
ratio of 0.15, a diagnostic ratio of 43, and a combined sum of areas under the
target operating characteristic curve of 0.93 [16].
Cardiology has kept pace with the AI revolution. AI systems in cardiology have been
crucial in predicting cardiac events, thereby improving preventive cardiac care. A
review has underscored the potential of AI for data interpretation and automated
analysis in interventional cardiology procedures. ML techniques are employed in
interventional cardiology for image reconstruction, interpretation, and analysis. ML
models, including the lasso-penalized Cox proportional hazards regression model and
the k-means clustering algorithm, have been utilized for predicting mortality and
detecting the QRS complex, respectively.
ML algorithms have been developed for angiographic recognition, coronary angiographic
interpretation, and intravascular ultrasonographic image segmentation. These
algorithms have demonstrated promising outcomes in terms of recall, precision,
accuracy, and agreement with expert analysts [17].
Another review has found that wearable devices, such as smartwatches and activity
trackers, can collect and analyze long-term, continuous data on behavioral or
physiological functions, providing healthcare providers with a more comprehensive
picture of a patient's health compared to the traditional, sporadic
measurements obtained through office consultations and hospitalizations. Wearable
devices have numerous clinical applications, including screening for arrhythmias in
high-risk populations and the remote management of chronic conditions like heart
failure or peripheral artery disease [18].
Ishii et al. have developed and validated an ML-based model to predict future adverse
events in patients with atrial fibrillation and stable coronary artery disease.
Using randomized survival forest and Cox regression models, they created an
integer-based risk score for all-cause mortality, myocardial infarction, stroke, and
major bleeding, collectively defined as net adverse clinical events. This scoring
system categorizes patients into three risk groups: low-risk (0–4 points),
intermediate (5–8 points), and high-risk (≥9 points). The
integer-based risk score has demonstrated strong performance in both the development
and validation cohorts, exhibiting good discriminatory and calibration power.
Decision curve analysis has shown a significant net benefit associated with this
score [19].
The widespread adoption of AI in these specialties stands in stark contrast to its
integration into general surgery, underscoring a significant gap in both research
and clinical applications.
Advancements in artificial intelligence across various surgical
departments
AI in neurosurgery has led to significant advancements in tumor identification and
surgical planning. ML algorithms are employed to delineate tumors precisely,
enhancing surgical accuracy and improving patient outcomes. Additionally, AI assists
in predicting risks and developing personalized treatment plans.
Njiwa et al. investigated whether increased preoperative white matter (WM)
18F-FDG uptake can be used to predict surgical outcomes and compared
the predictive performance of 11C-flumazenil (FMZ) and
18F-FDG–PET, using advanced ML techniques. They showed that at the
group level, patients who were non-seizure-free (NSF) had more pronounced
periventricular 11C-FMZ and 18F-FDG signal increases than
patients who were seizure-free (SF). Five out of eight patients who were NSF had a
periventricular WM signal increase in both 11C-FMZ and
18F-FDG, whereas only one out of eight patients who were SF had a
periventricular WM signal increase in 11C-FMZ; and four out of eight had
a periventricular WM signal increase in 18F-FDG, at the optimized
threshold. Random forest classification correctly identified seven out of eight SF
patients and seven out of eight NSF patients using 11C-FMZ images, but
only four out of eight SF patients and six out of eight NSF patients, using
18F-FDG. The presence of ipsilateral medial temporal lobe
hypometabolism predicted SF outcome status, while the absence thereof predicted NSF;
nonetheless, 11C-FMZ-based methods performed better than
18F-FDG-based methods [20].
Ma et al. developed a noninvasive ML model to assist in identifying the grade and
mutational status of molecular markers in intramedullary gliomas. This development
is significant, as invasive biopsies for histopathological analyses carry a high
risk of tissue damage. The results indicated that the Swin transformer-based model
achieved high accuracy and dice similarity coefficients in the automatic
segmentation of lesions during both the sagittal (SAG) and transverse (TRA) phases,
with values of 0.9929 and 0.8697 for the SAG phase and 0.9978 and 0.8738 for the TRA
phase. The neural network, based on the proposed multimodal fusion
(SAG–TRA–clinical) features, demonstrated superior performance in
predicting the grade and mutational status of molecular markers in intramedullary
gliomas. The area under the receiver operating characteristic curve (AUC) was 0.8431
for grade prediction, 0.7622 for alpha thalassemia/mental retardation syndrome,
X-linked (ATRX) status prediction, and 0.7954 for tumor protein p53 status
prediction. The WHO-Mind model achieved the highest AUC, with a value of 0.8431 in
the test task; both the WHO-Mind and ATRX-Mind models recorded the highest accuracy,
each with a value of 0.8889 [21].
AI, particularly robot-assisted surgery, increases the precision of cardiac surgery.
Liu et al. compared the clinical outcomes of robot-assisted cardiac surgery (RACS),
utilizing the da Vinci robotic surgery system, with those of traditional open-heart
surgery (TOHS). There were no statistically significant differences between the RACS
and TOHS groups in terms of reoperation rates due to postoperative bleeding,
mortality numbers, and treatment interruptions. The RACS group had shorter operative
times and intensive care unit stays, fewer postoperative hospital days, and a
quicker return to normal daily activities post-discharge than the TOHS group [22].
Fujita et al. compared minimally invasive direct mitral valve replacement via right
thoracotomy with robotic mitral valve replacement to determine the feasibility of
using robotic techniques for more complex lesions. They found that the mean
complexity score for robotic repairs was significantly higher than that for
thoracotomy. Additionally, the robotic group underwent a greater number of mitral
valve replacements using polytetrafluoroethylene and performed fewer ablations. The
overall cure rate was 100%, with no early mortalities or strokes observed in either
group. In both groups, the mean postoperative residual mitral regurgitation was 0.3.
The mean pressure gradient across the mitral valve was 2.4 mmHg in the robotic group
and 2.7 mmHg in the thoracotomy group [23].
Another review article examined 27 studies that applied AI and big data to cardiac
transplantation, categorizing them into four areas: etiology, diagnosis, prognosis,
and treatment. AI-based algorithms demonstrated potential in predicting patterns and
determining survival rates. However, the studies selected exhibited a significant
risk of bias. The accuracy of AI-based models in predicting survival following
cardiopulmonary transplantation and prognosis in thoracic organ transplantation was
found to surpass that of traditional statistical methods. ML and DL techniques have
improved diagnostic tools for detecting allograft rejection and predicting
post-transplant survival. Additionally, ML has been employed to monitor the
therapeutic levels of immunosuppressive drugs [24].
The role of AI in orthopedic surgery has been demonstrated in areas such as joint
replacement and outcome prediction. AI is utilized for the customization of
prosthetics and early diagnosis, thereby improving the success rates and
effectiveness of orthopedic interventions.
Houserman et al. assessed the viability of an AI prediction model for knee
arthroplasty, utilizing three-view radiography to determine if patients with knee
pain required total knee arthroplasty (TKA), unicompartmental knee arthroplasty
(UKA), or no arthroplasty at all. The AI model achieved an accuracy of 87.8% and a
quadratic-weighted Cohen's kappa score of 0.811 in the holdout test set. It
performed exceptionally well in determining whether a patient was a candidate for
surgery, reaching an accuracy of 93.8%. The multiclass AUC scores for the three
categories—TKA, UKA, and no surgery—were all above 0.95, specifically
0.974, 0.957, and 0.98, respectively. The AI/ML model, as well as AI models in
general, demonstrated potential in predicting whether patients are suitable
candidates for UKA, TKA, or no surgery [25].
Jang et al. utilized DL to automate the measurement of leg length discrepancy (LLD)
using pelvic radiographs and to compare the LLD based on different anatomical
landmarks. The DL algorithm has successfully measured LLD on pelvic radiographs by
utilizing various combinations of landmarks, achieving intraclass correlation
coefficients (ICCs) ranging from 0.73 to 0.98. Measurements of LLD using the
teardrop and greater trochanter landmarks have shown an acceptable level of
agreement, with an ICC of 0.72 [26].
Advancing artificial intelligence in general surgery: current research landscape
and future directions
Research on AI in general surgery is expanding into numerous areas, reflecting the
diverse applications of AI in this multifaceted field. The integration of AI into
laparoscopic surgery enhances visualization, accuracy, and decision-making during
procedures.
In robotic surgery, AI has been leveraged to improve the precision and autonomy of
robotic systems, marking a significant shift toward more advanced surgical
techniques.
Endo et al. discussed the impact of an AI system on identifying anatomical landmarks
associated with reduced bile duct injury during laparoscopic cholecystectomy. After
viewing a 20-second video where the AI highlighted landmarks, 26.9% of the images
were annotated differently, primarily along the gallbladder line of the extrahepatic
bile and cystic ducts. Of these changes, 70% were considered safe. The AI system
assisted both novices and experts in identifying landmarks such as the Rouviere
sulcus and the inferior border of the liver, S4. It encouraged changing perspectives
in 70% of cases, in a way that was considered safe [27].
Zhang et al. explored the feasibility of conditional autonomy in robotic surgery,
specifically focusing on robotic appendectomy. This approach involved using
demonstration data gathered from a human operator performing appendectomies in a
simulated robotic environment to teach the system the movements and trajectories of
the robotic instruments. Extensive validation in a simulated environment, utilizing
the da Vinci research kit, demonstrated that the proposed method can perform
appendectomies semi-automatically. A framework based on this method could decrease
the total working path length, completion time, and appendix stump length, while
preserving a high similarity to the demonstrated trajectories [28].
In addition, AI models for surgical risk assessment are currently being developed.
These models use patient data and preoperative indicators to predict postoperative
complications, aiming to tailor surgical approaches to the specific risks of
individual patients. Additionally, AI plays a crucial role in surgical planning,
especially in complex procedures. Here, AI-driven image interpretation aids surgeons
in making informed decisions.
El Moheb et al. demonstrated that the AI risk calculator, Predictive OpTimal Trees in
Emergency Surgery Risk (POTTER), surpassed the surgeon's gestalt in
predicting postoperative mortality and outcomes for patients undergoing emergency
surgery, except in cases of septic shock. Risk prediction for mortality, bleeding,
and pneumonia improved when surgeons used POTTER, although there was no significant
improvement for septic shock or ventilator dependence. The AUC was calculated to
evaluate the predictive performance of surgeons who used POTTER compared to those
who did not [29].
The postoperative phase has also benefited from AI, particularly in the areas of
wound analysis and care. AI applications here concentrate on analyzing images of
wounds and predicting healing outcomes, potentially leading to more personalized and
effective postoperative care strategies.
Tomé et al. highlighted the necessity of AI by demonstrating the challenges in
predicting postoperative infections using only correlated data. According to their
research, postoperative infections occurred in 24 out of 349 operations, which
accounts for 6.89% of all surgeries in their database. Correlation tests employing
Pearson and Spearman coefficients indicated a weak correlation between the risk
factors and the incidence of infection. An artificial neural network designed for
pattern recognition successfully predicted infections in 77.3% of cases, achieving
an AUC of 0.9050. Among the misclassifications, seven cases were incorrectly
identified as having an infection when none was present, representing 2.0% of the
data. Conversely, five cases were incorrectly identified as not having an infection
when one was present, representing 1.4% of the data [30].
Overall, these diverse areas of AI application in general surgery underscore the
potential of AI to transform various aspects of surgical practice, from preoperative
planning to postoperative care [31,32]. As research progresses, the role of AI in
general surgery is anticipated to grow, setting the stage for more innovative and
effective surgical practices.
Bridging the artificial intelligence gap in general surgery
The integration of AI into specialties like radiology and cardiology has
significantly improved diagnostic accuracy and patient care. This stands in stark
contrast to its use in general surgery. The disparity underscores the unique
challenges faced in general surgery, which include the variability of surgical
procedures and the difficulty in capturing comprehensive datasets for AI
training.
Understanding the challenges and successful strategies used in other specialties can
provide valuable insights for adapting AI applications in general surgery,
suggesting a more focused approach to research and development in this area. The
primary issue is the relative scarcity of research directed toward implementing AI
in general surgical environments. The inherent variability and complexity of general
surgical procedures pose significant challenges in standardizing AI applications,
which in turn complicates the integration of AI. Additionally, constructing
comprehensive and uniform datasets, crucial for training AI, continues to be a major
hurdle in this field [33].
Despite these challenges, there are significant opportunities in general surgery
where AI can make substantial contributions, such as in risk assessment and surgical
planning [34–36]. Success stories from other medical and surgical fields
offer a blueprint and valuable insights for integrating AI into general surgery. By
drawing on these experiences, general surgery can tailor AI tools to meet its unique
needs, potentially transforming patient care and surgical outcomes [36–38].
Promoting research on AI and the application of AI in general surgery requires
fostering interdisciplinary collaboration across various fields, establishing
standardized data collection and sharing protocols, securing dedicated funding, and
integrating AI education into medical training. It is necessary to address ethical
considerations and provide regulatory support to build trust in AI applications.
Pilot projects and clinical trials are essential to demonstrate the efficacy and
safety of AI technologies in clinical settings, paving the way for their integration
into general surgery to enhance outcomes and patient care.
Conclusion
The future of AI in general surgery is poised for transformative growth, driven by
emerging technologies. Surgical robotics are increasing precision and safety,
virtual reality simulations are providing unparalleled training experiences, and
predictive analytics are improving postoperative care.
Focusing research on these areas could significantly advance the field of general
surgery, aligning it with the successes observed in other medical fields and opening
new avenues for enhancing patient care. In radiology, oncology, and cardiology, AI
has already begun to transform patient care by improving diagnostic accuracy,
providing predictive analytics, and facilitating personalized treatment plans.
However, the field of general surgery stands at the threshold of a significant
technological evolution, facing unique challenges that hinder the integration of AI.
To effectively incorporate AI into general surgery and address delays in current
research and development, interdisciplinary collaboration is essential. This
requires forming partnerships among medical practitioners, AI technologists, data
scientists, and policymakers. These collaborative efforts are vital for managing the
complexities of general surgical procedures, standardizing AI applications, and
constructing the comprehensive datasets required for AI training.
By leveraging diverse expertise, AI tools can be tailored to meet the unique
requirements of general surgery, thereby improving surgical outcomes, procedural
efficiency, and patient care.
The path forward requires a concerted effort to bridge this gap, focusing on the
development of AI tools tailored to the specific needs of general surgery, from
preoperative planning to postoperative care. Embracing AI in general surgery not
only promises to improve surgical outcomes and efficiency but also represents a
critical step toward a future where healthcare fully leverages technology, marking a
new chapter in the quest for enhanced patient care.
Authors' contributions
Project administration: not applicable
Conceptualization: Lee RA
Methodology & data curation: Baik SM
Funding acquisition: not applicable
Writing – original draft: Baik SM
Writing – review & editing: Baik SM, Lee RA
Conflict of interest
Ryung-Ah Lee has been an associate editor of the Ewha Medical
Journal since August 2023. However, she was not involved in the
review process. No other potential conflict of interest relevant to this review
was reported.
Funding
Not applicable.
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Mehta V. Artificial intelligence in medicine: revolutionizing healthcare
for improved patient outcomes. J Med Res Innov 2023;7(2):e000292.
2. Manfred D. Artificial intelligence (AI): what are the impacts for
medicine? J Artif Intell Cloud Comput 2019;2(2):1-3.
3. Paudyal R, Shah AD, Akin O, Do RKG, Konar AS, Hatzoglou V, et al. Artificial intelligence in CT and MR imaging for oncological
applications. Cancers 2023;15(9):2573
4. Derevianko A, Pizzoli SFM, Pesapane F, Rotili A, Monzani D, Grasso R, et al. The use of artificial intelligence (AI) in the radiology field:
what is the state of doctor–patient communication in cancer
diagnosis? Cancers 2023;15(2):470
5. Ram S, Bodduluri S. Implementation of artificial intelligence–assisted chest
X-ray interpretation: it is about time. Am Thorac Soc 2023;20(5):641-642.
7. Demetriou DD, Hull R, Kgoebane-Maseko M, Lockhat Z, Dlamini Z. AI-enhanced digital pathology and radiogenomics in precision
oncology. In: In: Dlamini Z, editor. editor. Artificial intelligence and precision oncology: bridging cancer research
and clinical decision support. Cham:: 1Springer; 2023 p. p. 93-113.
8. Zeineldin RA, Junger D, Mathis-Ullrich F, Burgert O. Development of an AI-driven system for neurosurgery with a
usability study: a step towards minimal invasive robotics. at - Automatisierungstechnik 2023;71(7):537-546.
10. Voskens FJ, Abbing JR, Ruys AT, Ruurda JP, Broeders IAMJ. A nationwide survey on the perceptions of general surgeons on
artificial intelligence. Artif Intell Surg 2022;2(1):8-17.
11. Lång K, Josefsson V, Larsson AM, Larsson S, Högberg C, Sartor H, et al. Artificial intelligence-supported screen reading versus standard
double reading in the Mammography Screening with Artificial Intelligence
trial (MASAI): a clinical safety analysis of a randomised, controlled,
non-inferiority, single-blinded, screening accuracy study. Lancet Oncol 2023;24(8):936-944.
12. Nam JG, Hwang EJ, Kim J, Park N, Lee EH, Kim HJ, et al. AI improves nodule detection on chest radiographs in a health
screening population: a randomized controlled trial. Radiology 2023;307(2):e221894.
13. Sachpekidis C, Enqvist O, Ulén J, Kopp-Schneider A, Pan L, Jauch A, et al. Application of an artificial intelligence-based tool in [18F]FDG
PET/CT for the assessment of bone marrow involvement in multiple
myeloma. Eur J Nucl Med Mol Imaging 2023;50(12):3697-3708.
14. Clift AK, Dodwell D, Lord S, Petrou S, Brady M, Collins GS, et al. Development and internal-external validation of statistical and
machine learning models for breast cancer prognostication: cohort
study. BMJ 2023;381:e073800.
15. Alaimo L, Lima HA, Moazzam Z, Endo Y, Yang J, Ruzzenente A, et al. Development and validation of a machine-learning model to predict
early recurrence of intrahepatic xholangiocarcinoma. Ann Surg Oncol 2023;30(9):5406-5415.
16. Liu M, Wu J, Wang N, Zhang X, Bai Y, Guo J, et al. The value of artificial intelligence in the diagnosis of lung
cancer: a systematic review and meta-analysis. PLOS ONE 2023;18(3):e0273445.
17. Subhan S, Malik J, Haq A, Qadeer MS, Zaidi SMJ, Orooj F, et al. Role of artificial intelligence and machine learning in
interventional cardiology. Curr Probl Cardiol 2023;48(7):101698
19. Ishii M, Kaikita K, Yasuda S, Akao M, Ako J, Matoba T, et al. Risk prediction score for clinical outcome in atrial fibrillation
and stable coronary artery disease. Open Heart 2023;10(1):e002292.
20. Yankam Njiwa J, Gray KR, Costes N, Mauguiere F, Ryvlin P, Hammers A. Advanced [18F]FDG and [11C]flumazenil PET
analysis for individual outcome prediction after temporal lobe epilepsy
surgery for hippocampal sclerosis. Neuroimage Clin 2015;7:122-131.
21. Ma C, Wang L, Song D, Gao C, Jing L, Lu Y, et al. Multimodal-based machine learning strategy for accurate and
non-invasive prediction of intramedullary glioma grade and mutation status
of molecular markers: a retrospective study. BMC Med 2023;21(1):198
22. Liu Z, Zhang C, Ge S. Efficacy and safety of robotic-assisted versus median sternotomy
for cardiac surgery: results from a university affiliated
hospital. J Thorac Dis 2023;15(4):1861-1871.
23. Fujita T, Kakuta T, Kawamoto N, Shimahara Y, Yajima S, Tadokoro N, et al. Benefits of robotically-assisted surgery for complex mitral valve
repair. Interact Cardiovasc Thorac Surg 2021;32(3):417-425.
24. Palmieri V, Montisci A, Vietri MT, Colombo PC, Sala S, Maiello C, et al. Artificial intelligence, big data and heart transplantation:
actualities. Int J Med Inform 2023;176:105110
25. Houserman DJ, Berend KR, Lombardi AV Jr, Fischetti CE, Duhaime EP, Jain A, et al. The viability of an artificial intelligence/machine learning
prediction model to determine candidates for knee
arthroplasty. J Arthroplasty 2023;38(10):2075-2080.
26. Jang SJ, Kunze KN, Bornes TD, Anderson CG, Mayman DJ, Jerabek SA, et al. Leg-length discrepancy variability on standard anteroposterior
pelvis radiographs: an analysis using deep learning
measurements. J Arthroplasty 2023;38(10):2017-2023. E3.
27. Endo Y, Tokuyasu T, Mori Y, Asai K, Umezawa A, Kawamura M, et al. Impact of AI system on recognition for anatomical landmarks
related to reducing bile duct injury during laparoscopic
cholecystectomy. Surg Endosc 2023;37(7):5752-5759.
28. Zhang R, Chen J, Wang Z, Yang Z, Ren Y, Shi P, et al. A step towards conditional autonomy - robotic
appendectomy. IEEE Robot Autom Lett 2023;8(5):2429-2436.
29. Moheb M, Gebran A, Maurer LR, Naar L, El Hechi M, Breen K, et al. Artificial intelligence versus surgeon gestalt in predicting risk
of emergency general surgery. J Trauma Acute Care Surg 2023;95(4):565-572.
33. Rimmer L, Howard C, Picca L, Bashir M. The automaton as a surgeon: the future of artificial intelligence
in emergency and general surgery. Eur J Trauma Emerg Surg 2021;47(3):757-762.
35. Mangano A, Valle V, Dreifuss NH, Aguiluz G, Masrur MA. Role of artificial intelligence (AI) in surgery: introduction,
general principles, and potential applications. Surg Technol Int 2020;38:17-21.
38. Bar O, Neimark D, Zohar M, Hager GD, Girshick R, Fried GM, et al. Impact of data on generalization of AI for surgical intelligence
applications. Sci Rep 2020;10(1):22208