Abstract
-
Objectives:
During the COVID-19 pandemic, the first seasonal influenza epidemic was
declared in the 37th week of 2022 in Korea and has continued through the
winter of 2023–2024. However, this finding has not been observed in
the United States and Europe. The present study aimed to determine whether
the prolonged influenza epidemic in Korea from 2022 to 2023 was caused by
using a different influenza epidemic threshold compared to the thresholds
used in the United States and Europe.
-
Methods:
Korea, the United States, and Europe use different methods to set seasonal
influenza epidemic thresholds. First, we calculated the influenza epidemic
thresholds for influenza seasons using the different methods of those three
regions. Using these epidemic thresholds, we then compared the duration of
influenza epidemics for the most recent three influenza seasons.
-
Results:
The epidemic thresholds estimated by the Korean method were lower than those
by the other methods, and the epidemic periods defined using the Korean
threshold were estimated to be longer than those defined by the other
regions’ thresholds.
-
Conclusion:
A low influenza epidemic threshold may have contributed to the prolonged
influenza epidemic in Korea, which was declared in 2022 and has continued
until late 2023. A more reliable epidemic threshold for seasonal influenza
surveillance needs to be established in Korea.
-
Keywords: Influenza; human; Sentinel surveillance; Epidemics; Seasons
Introduction
Background
Influenza is a communicable disease primarily caused by influenza A or B viruses.
It is a common acute respiratory illness that tends to spread during the winter
season in Korea. Transmission occurs through respiratory droplets emitted from
infected subjects. The basic reproduction number, which is defined as the
average number of secondary cases per case in a totally susceptible population,
has been observed to range from 1.27 to 1.8 in the four pandemics since the 20th
century and during seasonal influenza epidemics [
1]. Influenza poses a high risk of complications and can result in
serious clinical outcomes in vulnerable populations, such as those aged 65 and
above, children, and people with chronic diseases. It also increases absenteeism
rates at workplaces and schools, and rapidly increases the demand for medical
care, significantly impacting society from a public health perspective.
Influenza surveillance involves collecting data on influenza transmission trends
and circulating virus types to predict the timing and intensity of epidemics.
Surveillance helps maintain an appropriate level of preparedness, with the goal
of minimizing the socioeconomic impact during the influenza season. In Korea,
surveillance measures include monitoring outpatient illness, hospitalizations,
and virological factors to determine the onset and end of epidemics, analyze
their progression, and manage seasonal influenza based on pathogen
characteristics. Outpatient illness surveillance is carried out at approximately
200 sentinel sites nationwide as of October 2023, with 87 of these sites also
participating in virological surveillance. Additionally, influenza
hospitalizations and deaths are surveilled at secondary and tertiary hospitals
to monitor the severity of seasonal influenza [
2].
In Korea and the United States (U.S.), influenza surveillance among outpatients
collects information on influenza-like illness (ILI). The proportion of visits
with ILI among all outpatient visits is estimated and used as a monitoring tool
for influenza surveillance [
2,
3]. While the case definition of ILI varies
across countries and agencies, it generally consists of fever and respiratory
infection symptoms. Since ILI is a common clinical presentation of various
respiratory infections, it is used as a surrogate indicator for tracking
influenza epidemics even though it does not accurately estimate the incidence of
influenza [
4,
5]. The positivity rate of respiratory specimens for
influenza viruses is also used as a monitoring indicator, with the European
Centre for Disease Prevention and Control (ECDC) defining the start and end of
influenza epidemics based on a 10% positivity rate in respiratory samples
collected from sentinel sites [
6].
In Korea, unlike the U.S. and Europe, an influenza alert that was issued in the
37th week of 2022 has been in effect for 69 consecutive weeks as of December
2023 [
7]. This is the first occurrence of
such a phenomenon since the establishment of the influenza surveillance system
in Korea in 2000. It also deviates from the well-known epidemiological
characteristic that influenza typically spreads in the winter season in
temperate regions [
8–
10]. Therefore, a rigorous assessment is
necessary to determine whether this phenomenon can be interpreted as reflecting
an actual prolonged increase in influenza activity.
This study aimed to compare the duration of seasonal influenza epidemics
calculated using different influenza epidemic thresholds used in Korea, the
U.S., and Europe. The implications of the study findings will be discussed in
the context of the ongoing influenza epidemic in Korea that has lasted since
2022.
Methods
Ethics statement
This study was based on public data. Neither approval by the institutional review
board nor obtainment of informed consent was required.
Study design
This was a comparative study.
Setting
The epidemic periods for the three most recent seasons (2018–2019,
2019–2020, 2022–2023) were analyzed, excluding the two seasons
(2020–2021, 2021–2022) that did not experience influenza
epidemics. This analysis applied the epidemic thresholds established by Korea,
the U.S., and Europe.
Data sources and measurement
National influenza surveillance data in Korea were collected from the weekly
reports published by the Korea Disease Control and Prevention Agency (KDCA)
[
11]. Weekly data on ILI rates, the
number of respiratory specimens, and the number of influenza-positive specimens
from the 36th week of 2015 to the 35th week of 2023 were used. In Korea, ILI is
defined as the presence of fever of 38℃ or higher and respiratory
infection symptoms, such as cough and sore throat. Accordingly, this study
applied the Korean ILI definition to data to estimate the epidemic threshold for
Korea using the Korean and the U.S. methods [
2]. Data from the 2020–2021 and 2021–2022 seasons were
excluded from the analysis, as there was no influenza outbreak during these
seasons. The influenza season was defined as the period from the 36th week of
each year to the 35th week of the following year. Each week was defined as
starting on Sunday and ending on Saturday. For a week that spanned two years,
the week number was assigned based on the year in which the Sunday fell.
The influenza epidemic thresholds from the KDCA, the U.S. Centers for Disease
Control and Prevention (CDC), and the ECDC were chosen for a comparative
analysis. Korea and the U.S. use the sum of the mean and two standard deviations
of weekly ILI rates from non-influenza time periods as the epidemic threshold.
In Korea, data from the past 3 seasons are used for the calculation, whereas
data from the past 2 seasons are used in the U.S. [
2,
3]. Europe, in
contrast, uses a 10% influenza positivity rate in respiratory specimens as the
epidemic threshold (
Table 1) [
6]. For the Korean and U.S. methods, the
earlier of two consecutive weeks when the weekly ILI rate exceeds the epidemic
threshold is defined as the start of the influenza epidemic, and the week prior
to two consecutive weeks when the weekly ILI rate does not reach the epidemic
threshold is defined as the end of the epidemic. In the European method, the
epidemic period is determined based on the 10% influenza positivity rate.
Table 1.Epidemic thresholds for seasonal influenza
|
Country/region |
Epidemic threshold |
|
Korea (KDCA) |
-[Mean rate of ILI (per 1,000) during
non-influenza weeks for the most recent three
seasons+(2×SDs)]
-A non-influenza time period is
defined as two or more consecutive weeks in which influenza
positivity among respiratory laboratory samples is lower than
2% |
|
United States (CDC) |
-[Mean percentage of ILI during
non-influenza weeks for the most recent two
seasons+(2×SDs)]
-A non-influenza time period is
defined as two or more consecutive weeks in which each week
accounted for less than 2% of the season’s total number
of specimens that tested positive for influenza |
|
Europe (ECDC) |
-10% influenza positivity among
respiratory laboratory samples |
Bias
There was no bias in selecting target data.
Study size
There was no need to calculate the study size because known data were used.
Statistical methods
Descriptive statistics were used.
Results
Epidemic trends in Korea according to the Korean influenza epidemic
threshold
In total, 312 weeks of data from six influenza seasons were collected from the
KDCA's weekly reports. Despite using the same influenza surveillance
data, differences were observed in the epidemic thresholds and the durations of
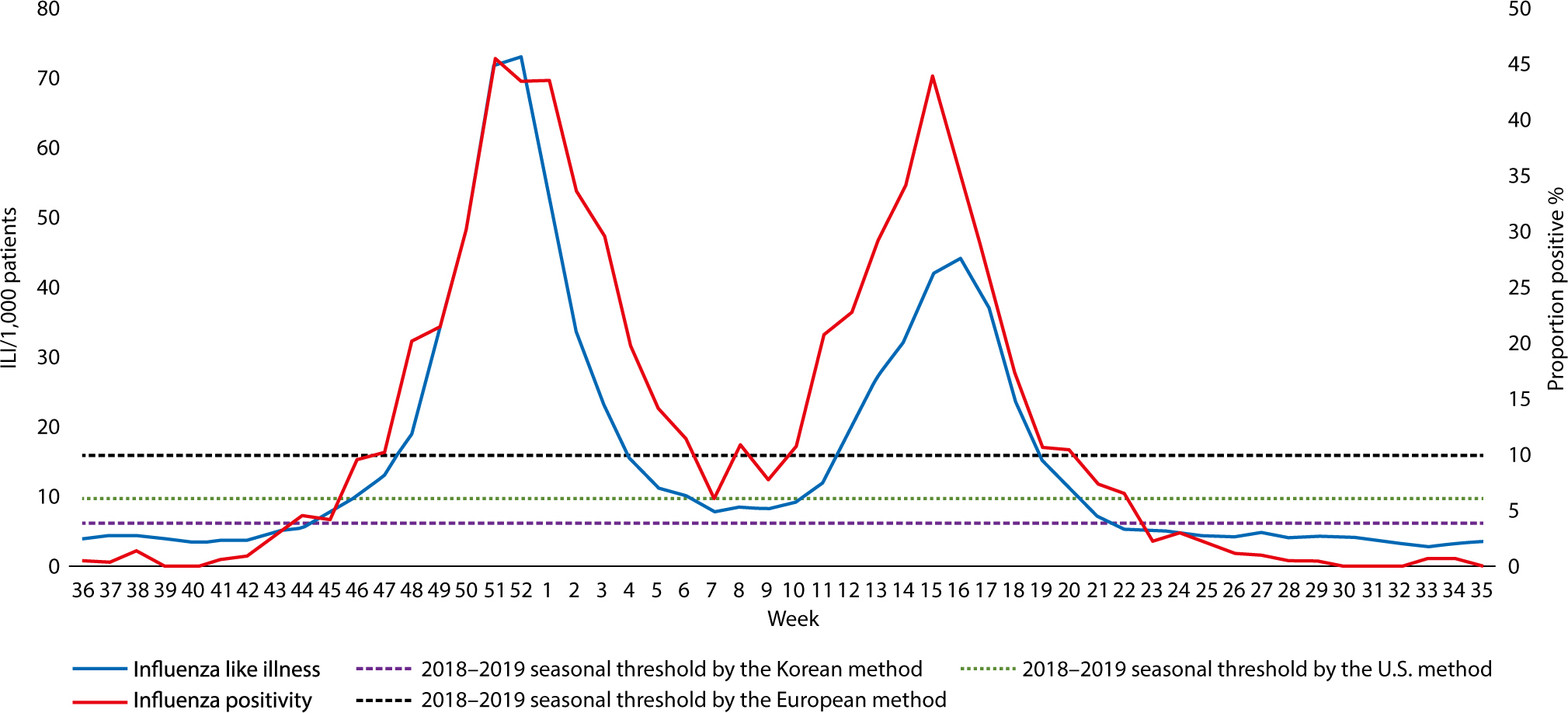
epidemics depending on the applied method. In the 2018–2019 season, two
influenza epidemic peaks were observed (
Fig.
1, Dataset 1), and in the 2019–2020 season, the epidemic ended
early due to the measures taken in response to the emergence of severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2), with no spring outbreak
observed (
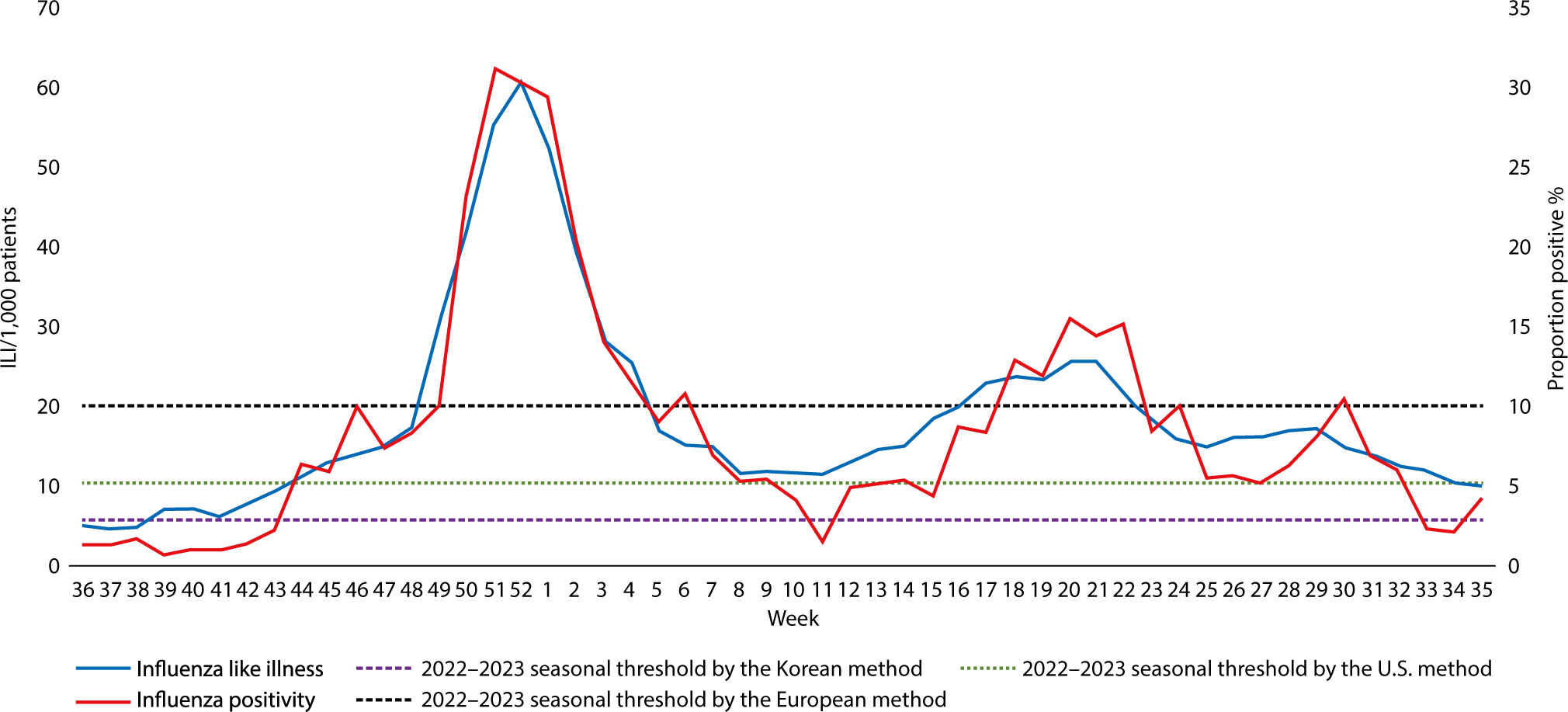
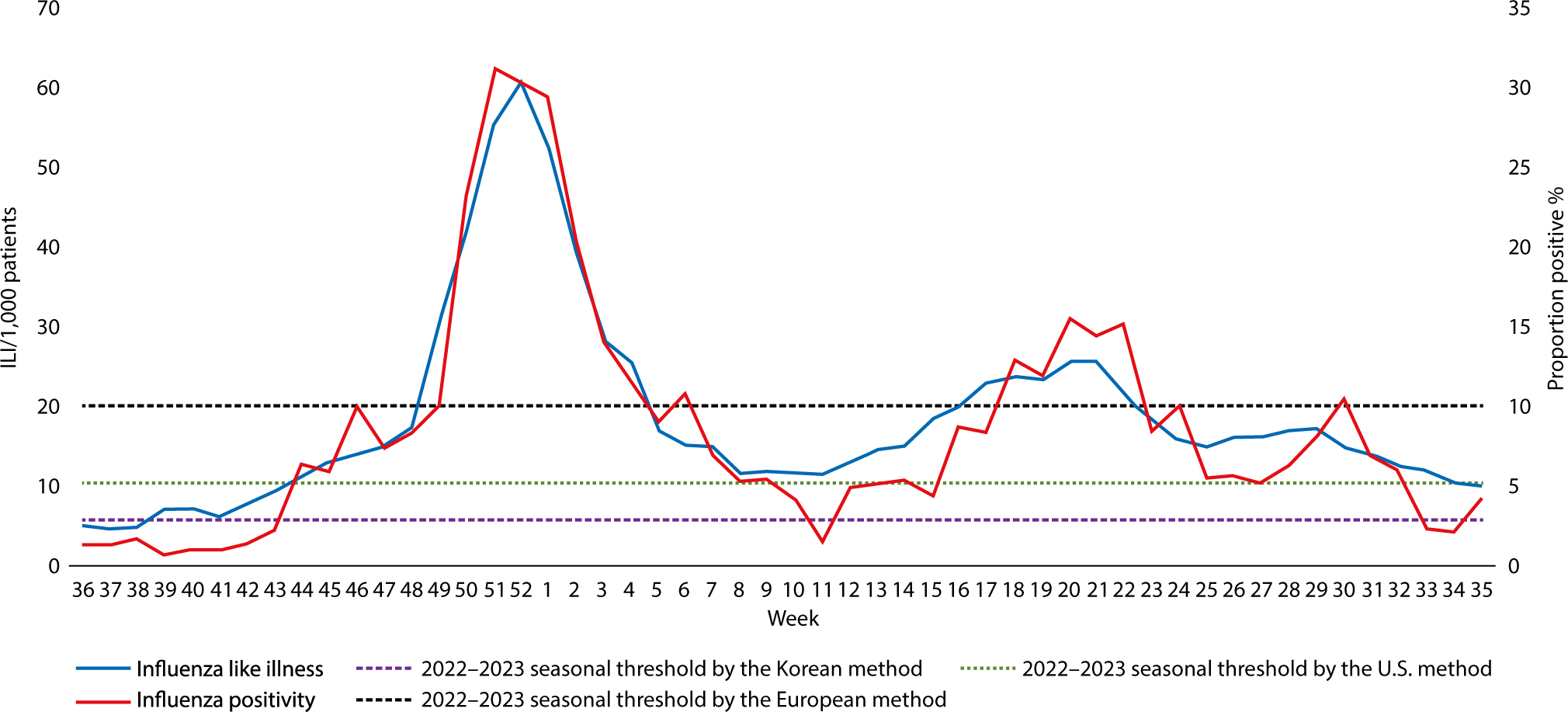
Fig. 2, Dataset 2). In the
2022–2023 season, elevated ILI rates were observed in general (
Fig. 3, Dataset 3).
Fig. 1.2018−2019 season influenza activity. ILI, influenza-like
illness.
Fig. 2.2019−2020 season influenza activity. ILI, influenza-like
illness.
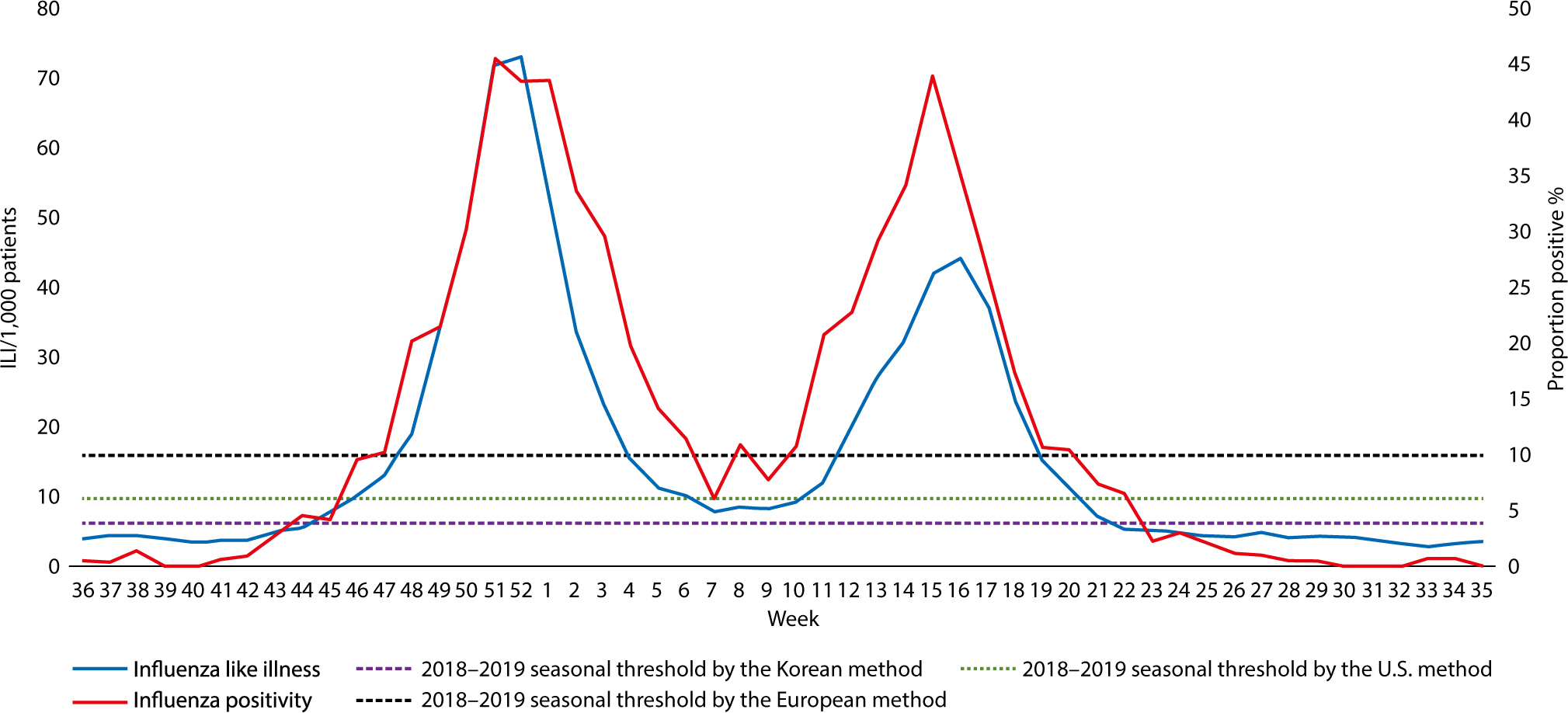
Fig. 3.2022−2023 season influenza activity. ILI, influenza-like
illness.
Non-influenza time periods
To calculate the epidemic threshold, the Korean method used ILI rates from
non-influenza periods in 156 weeks of the past 3 matching seasons, while the
U.S. method used ILI rates from non-influenza periods in 104 weeks of the past 2
matching seasons. For the Korean method, the non-influenza period for the
epidemic threshold calculations for the 2018–2019, 2019–2020, and
2022–2023 seasons comprised an average of 70.7 weeks (45.3%), while the
non-influenza period for the same seasons using the U.S. method was an average
of 74.7 weeks (71.8%). Since the non-influenza period defined by the Korean
method was shorter, lower ILI rates were used in the epidemic threshold
calculation than with the U.S. method. Accordingly, the mean and SD values
derived from the ILI rates for the non-influenza time periods used in the Korean
method were lower than those for the U.S. method (
Table 2).
Table 2.Characteristics of the influenza seasons used for epidemic threshold
calculation
|
Influenza season |
Korean method |
U.S. method |
|
Seasons used for the calculation
(length*) |
Length* of non-influenza period |
Mean rate of ILI during
non-influenza weeks |
SD of ILI during non-influenza
weeks |
Seasons used for the calculation
(length*) |
Length* of non-influenza period |
Mean rate of ILI during
non-influenza weeks |
SD of ILI during non-influenza
weeks |
|
2018−2019 |
2015−2016, 2016−2017,
2017−2018 (156) |
75 |
4.63 |
0.85 |
2016−2017, 2017−2018
(104) |
76 |
5.70 |
2.01 |
|
2019−2020 |
2016−2017, 2017−2018,
2018−2019 (156) |
64 |
4.38 |
0.79 |
2017−2018, 2018−2019
(104) |
74 |
5.87 |
2.62 |
|
2022−2023 |
2017−2018, 2018−2019,
2019−2020 (156) |
73 |
3.51 |
1.15 |
2018−2019, 2019−2020
(104) |
74 |
4.64 |
2.91 |
Influenza epidemic thresholds
The influenza epidemic thresholds estimated using the Korean method were 6.3 ILI
cases per 1,000 patients (2018–2019 season), 6.0 ILI cases per 1,000
patients (2019–2020 season), 5.8 ILI cases per 1,000 patients
(2022–2023 season), and 6.3 ILI cases per 1,000 patients
(2023–2024 season). The thresholds calculated using the U.S. method were
9.7 ILI cases per 1,000 patients (2018–2019 season), 11.1 ILI cases per
1,000 patients (2019–2020 season), 10.5 ILI cases per 1,000 patients
(2022–2023 season), and 18.7 ILI cases per 1,000 patients
(2023–2024 season). The Korean method yielded lower epidemic thresholds
than the U.S. method in all seasons. The largest difference was observed for the
2023–2024 season, which reflected the 2022–2023 season data during
the COVID-19 pandemic (
Table 3).
Table 3.Comparison of influenza epidemic thresholds according to different
methods
|
Season |
Threshold according to the Korean
method*
|
Threshold according to the U.S.
method*
|
European threshold |
|
2018−2019 |
6.3 |
9.7 |
10% influenza
positivity |
|
2019−2020 |
6.0 |
11.1 |
|
2022−2023 |
5.8 |
10.5 |
|
2023−2024 |
6.3 |
18.7 |
The epidemic period estimated using the thresholds of Korea, U.S., and
Europe
The estimated duration of the epidemic period using the Korean threshold was
longer than those calculated with the U.S. and European thresholds in all
seasons. The durations based on the Korean thresholds were 29 weeks
(2018–2019 season), 17 weeks (2019–2020 season), and 49 weeks
(2022–2023 season). In contrast, the durations based on the U.S.
thresholds were 23 weeks (2018–2019 season), 12 weeks (2019–2020
season), and 43 weeks (2022–2023 season). Durations calculated with the
European thresholds were the shortest, at 24 weeks (2018–2019 season), 13
weeks (2019–2020 season), and 16 weeks (2022–2023 season;
Table 4). The mean epidemic duration for
three seasons based on the Korean thresholds was 5.7 weeks (22%) longer per
season compared to that calculated using the U.S. method, and 14 weeks (79%)
longer compared to that calculated using the European method. The difference was
particularly prominent in the 2022–2023 season, where the duration based
on the Korean thresholds was 33 weeks longer than that based on the European
threshold.
Table 4.Comparison of epidemic period durations according to different
thresholds
|
Season |
Duration according to the Korean
threshold (weeks) |
Duration according to the U.S.
threshold (weeks) |
Duration according to the European
threshold (weeks) |
|
2018−2019 |
29 |
23 |
24 |
|
2019−2020 |
17 |
12 |
13 |
|
2022−2023 |
49 |
43 |
16 |
Discussion
Key results
This study compared the influenza epidemic periods in Korea during the
2018–2019, 2019–2020, and 2022–2023 seasons, utilizing
epidemic thresholds from Korea, the U.S., and Europe. The influenza epidemic
threshold calculated with the Korean method was approximately 49% lower than
that calculated using the U.S. method. Additionally, the epidemic durations
based on the Korean thresholds were longer than those based on the U.S. and
European thresholds.
Interpretation
The differences in epidemic thresholds between the Korean and the U.S. methods
primarily stemmed from the different definitions of the non-influenza time
period in both countries. In Korea, this period is defined as when the weekly
influenza positivity rate falls below 2%, a figure that is influenced by the
activity levels of other respiratory viruses. In contrast, the U.S. defines the
non-influenza period as the time when the number of weekly influenza-positive
specimens is less than 2% of the season's total count of
influenza-positive specimens, a measure that remains unaffected by the activity
of other respiratory viruses. It is important to note that the 2% influenza
positivity rate used in Korea's definition of the non-influenza period is
significantly lower than the European epidemic threshold of 10%. This
discrepancy results in the use of lower ILI rates from periods of relatively low
influenza activity to calculate the Korean epidemic threshold. Consequently,
this could lead to the earlier issuance and later lifting of influenza epidemic
alerts.
The largest difference between the epidemic durations determined by ILI
rate-oriented thresholds and those determined by influenza positivity
rate-oriented thresholds was observed in the 2022–2023 season. The
epidemic duration based on the Korean method was 49 weeks, which was roughly 3
times longer than the 16-week epidemic duration based on the European threshold.
This discrepancy can be partially attributed to changes in the incidence levels
of overall respiratory infectious diseases. During the COVID-19 pandemic, the
implementation of stringent social distancing measures and enhanced personal
hygiene practices led to a reduced incidence of respiratory infections. However,
this low incidence began to increase as public health measures were relaxed in
the latter half of 2022. Subsequently, a resurgence of various respiratory
infections elevated the overall ILI rates, which likely contributed to the
extended epidemic period by interacting with the lower epidemic threshold in the
2022–2023 season [
12,
13].
According to project reports from the Korea Respiratory Virus Integrated
Surveillance System, which tests respiratory samples from respiratory infection
patients, including cases of ILI, at sentinel sites, the influenza virus
detection rates in 2022 and 2023 were 5.5% and 16.1%, respectively. These rates
are similar to or lower than the rates of 17% and 14% observed in 2018 and 2019,
before the COVID-19 pandemic. In contrast, the detection rates of SARS-CoV-2 in
2022 and 2023 were 9.4% and 9.8%. The detection rates of other respiratory
viruses have also increased since 2021 (
Table
5) [
11,
14,
15]. This finding
is consistent with a report that the first post-pandemic influenza epidemic was
not considered unexpected in terms of extent and severity in most countries
[
16]. Therefore, the increase in ILI
rates in the 2022–2023 season is likely due to the increased activity of
SARS-CoV-2 and other respiratory viruses, rather than a significant increase in
influenza activity.
Table 5.Virological surveillance results of respiratory specimens
|
Year |
Total respiratory virus positivity
[% (n*)] |
Influenza virus positivity
[% (n*)] |
SARS-CoV-2 virus positivity [%
(n*)] |
Other respiratory virus†
positivity [% (n*)] |
|
2023 |
81.4 (Na) |
16.1 (Na) |
9.8 (Na) |
55.5 (Na) |
|
2022 |
72.7 (Na) |
5.5 (491) |
9.4 (Na) |
57.8 (5,205) |
|
2021 |
65.1 (3,009) |
0 (0) |
NA |
65.1 (3,009) |
|
2020 |
48.6 (2,830) |
12 (701) |
NA |
36.6 (2,129) |
|
2019 |
60.2 (7,311) |
14 (1,702) |
NA |
46.2 (5,609) |
|
2018 |
63.0 (Na) |
17 (Na) |
NA |
46.0 (Na) |
ILI is a widely used medical concept and a reliable indicator in influenza
surveillance [
17]. However, since the
clinical features of various respiratory infections often overlap, a rise in
influenza activity alone may not fully explain the increase in ILI rates. When
analyzing a rise in ILI rates, it is crucial to consider all circulating
respiratory pathogens collectively, in conjunction with laboratory test results,
to determine the extent to which each pathogen contributes to the increase
[
18]. The ongoing influenza epidemic
in Korea since the 37th week of 2022 appears to be a phenomenon resulting from
the combination of the lower influenza epidemic threshold in Korea and the
overall increase in ILI rates due to the increased activity of SARS-CoV-2 and
other respiratory viruses.
The study did not explore the characteristics of each epidemic threshold, such as
the sensitivity and specificity of its application. Merely comparing the
durations of epidemic periods does not determine which method should be
recommended for a specific country. The approach to setting the influenza
epidemic threshold should be assessed differently, taking into account each
country’s health system capacity and disease burden. In this study, the
influenza epidemic thresholds used in the U.S. and Europe were only compared
with those in Korea. Additional comparisons with other countries may increase
the generalizability of the study findings.
Conclusion
Influenza surveillance systems are designed to minimize the socioeconomic losses
caused by influenza epidemics, making the application of an appropriate epidemic
threshold crucial. This study noted variations in the duration of the epidemic
period based on the threshold applied. A low influenza epidemic threshold may have
contributed to the prolonged epidemic period, which was declared in the 37th week of
2022 and continued until the end of 2023 in Korea. The optimal epidemic threshold
should be examined from various perspectives, including the evolving epidemiological
characteristics of respiratory infectious diseases since the emergence of
SARS-CoV-2. Adopting multiple indicators could enable the issuance of more reliable
flu alerts and the implementation of more effective countermeasures.
Authors' contributions
-
Project administration: Lee J
Conceptualization: Lee J
Methodology & data curation: Lee J
Funding acquisition: not applicable
Writing – original draft: Lee J
Writing – review & editing: Lee J, Huh S, Seo H
Conflict of interest
-
No potential conflict of interest relevant to this article was reported.
Funding
-
Not applicable.
Data availability
-
The data used in this study are retrieved from the infectious diseases portal of
the KDCA available from: https://dportal.kdca.go.kr/pot/is/st/influ.do
Data files are available from Harvard Dataverse: https://doi.org/10.7910/DVN/9ZYE8N
Dataset 1. Research data used to draw Fig.
1, which shows seasonal influenza activity during the 2018−2019
season in Korea according to different influenza epidemic thresholds in Korea,
the United States, and Europe
Dataset 2. Research data used to draw Fig.
2, which shows seasonal influenza activity during the 2019−2020
season in Korea according to different influenza epidemic thresholds in Korea,
the United States, and Europe
Dataset 3. Research data used to draw Fig.
3, which shows seasonal influenza activity during the 2022−2023
season in Korea according to different influenza epidemic thresholds in Korea,
the United States, and Europe
Acknowledgments
Not applicable.
Supplementary materials
-
Not applicable.
References
- 1. Biggerstaff M, Cauchemez S, Reed C, Gambhir M, Finelli L. Estimates of the reproduction number for seasonal, pandemic, and
zoonotic influenza: a systematic review of the literature. BMC Infect Dis 2014;14:480
- 2. Korea Disease Control and Prevention Agency. Management strategies for seasonal influenza, 2023-24 season. Cheongju: Korea Disease Control and Prevention Agency; 2023.
- 3. Centers for Disease Control and Prevention
[CDC]. U.S. influenza surveillance: purpose and methods [Internet]. Atlanta (GA): CDC; c2024 [cited 2024 Jan 5]. Available from https://www.cdc.gov/flu/weekly/overview.htm
- 4. Brammer L, Budd A, Cox N. Seasonal and pandemic influenza surveillance considerations for
constructing multicomponent systems. Influenza Other Respir Viruses 2009;3(2):51-58.
- 5. Spencer JA, Shutt DP, Moser SK, Clegg H, Wearing HJ, Mukundan H, et al. Distinguishing viruses responsible for influenza-like
illness. J Theor Biol 2022;545:111145
- 6. European Centre for Disease Prevention and Control
[ECDC]. Seasonal influenza 2022-2023: annual epidemiological report for
2023. Stockholm: ECDC; 2023.
- 7. Korea Disease Control and Prevention Agency. Announcement of 2023-2024 influenza season initiation
[Internet]. Cheongju (KR): Korea Disease Control and Prevention Agency; c2023 [cited 2024 Jan 5]. Available from https://www.kdca.go.kr/board/board.es?mid=a20501010000&bid=0015&list_no=723470&cg_code=&act=view&nPage=1
- 8. Tamerius JD, Shaman J, Alonso WJ, Bloom-Feshbach K, Uejio CK, Comrie A, et al. Environmental predictors of seasonal influenza epidemics across
temperate and tropical climates. PLOS Pathog 2013;9(3):e1003194.
- 9. Korea Disease Control and Prevention Agency. 2022 Annual report on infectious disease reports [Internet]. Cheongju (KR): Korea Disease Control and Prevention Agency; c2022 [cited 2024 Feb 16]. Available from https://dportal.kdca.go.kr/pot/bbs/BD_selectBbs.do?q_bbsSn=1010&q_bbsDocNo=20230908669355443&q_clsfNo=1
- 10. Lee JW. Another flu season declaration… The first season continued for
more than a year [Internet]. Seoul (KR): The Dong-a Ilbo; c2023 [cited 2023 Sep 15]. Available from https://www.donga.com/news/Health/article/all/20230915/121190131/1
- 11. Korea Disease Control and Prevention Agency. Infectious diseases, sentinel surveillance report [Internet]. Cheongju (KR): Korea Disease Control and Prevention Agency; c2024 [cited 2024 Jan 5]. Available from https://dportal.kdca.go.kr/pot/bbs/BD_selectBbsList.do?q_bbsSn=1010&q_bbsDocNo=&q_clsfNo=2&q_searchKeyTy=&q_searchVal=&q_currPage=1&q_sortName=&q_sortOrder=
- 12. Cha J, Seo Y, Kang S, Kim I, Gwack J. Sentinel surveillance results for influenza and acute respiratory
infections during the coronavirus disease 2019 pandemic. Public Health Wkly Rep 2023;16(20):597-612.
- 13. Kim IH, Kang SK, Cha JO, Seo YJ, Gwack J, Lee NJ, et al. Changes in patterns of respiratory virus since the coronavirus
disease 2019 pandemic (until April 2023). Public Health Wkly Rep 2023;16(20):621-631.
- 14. Lee NJ, Woo S, Lee J, Rhee JE, Kim EJ. 2021-2022 Influenza and respiratory viruses laboratory
surveillance report in the Republic of Korea. Public Health Wkly Rep 2023;16(3):53-65.
- 15. Woo SH, Lee NJ, Lee JH, Rhee JE, Kim EJ. Korea 2022-2023 influenza and respiratory viruses laboratory
surveillance report. Public Health Wkly Rep 2024;17(2):455-469.
- 16. de Jong SPJ, Felix Garza ZC, Gibson JC, van Leeuwen S, de Vries RP, Boons GJ, et al. Determinants of epidemic size and the impacts of lulls in
seasonal influenza virus circulation. Nat Commun 2024;15(1):591
- 17. Fleming DM, Elliot AJ. Lessons from 40 years' surveillance of influenza in
England and Wales. Epidemiol Infect 2008;136(7):866-875.
- 18. Kelly H, Birch C. The causes and diagnosis of influenza-like
illness. Aust Fam Physician 2004;33(5):305-309.
Figure & Data
Citations
Citations to this article as recorded by

- Pertussis epidemic in Korea and implications for epidemic control
Joowon Lee
Infectious Diseases.2025; 57(2): 207. CrossRef - Invasive Group A Streptococcus infections in children during the post-pandemic period: results from a multicenter study in Italy
Elena Chiappini, Marco Renni, Maia De Luca, Samantha Bosis, Silvia Garazzino, Laura Dotta, Raffaele Badolato, Federica Zallocco, Daniele Zama, Antonella Frassanitto, Ilaria Liguoro, Danilo Buonsenso, Claudia Colomba, Lorenza Romani, Giulia Lorenzetti, Fed
Italian Journal of Pediatrics.2025;[Epub] CrossRef - The paradox of rapid and synchronized propagation of seasonal influenza ‘A’ outbreaks in contrast with COVID-19: a testable hypothesis
Uri Gabbay, Doron Carmi
Virus Research.2025; 362: 199670. CrossRef - Gender equity in medicine, artificial intelligence, and other
articles in this issue
Sun Huh
The Ewha Medical Journal.2024;[Epub] CrossRef