
| In Sook Kang | 6 Articles |
|
[English]
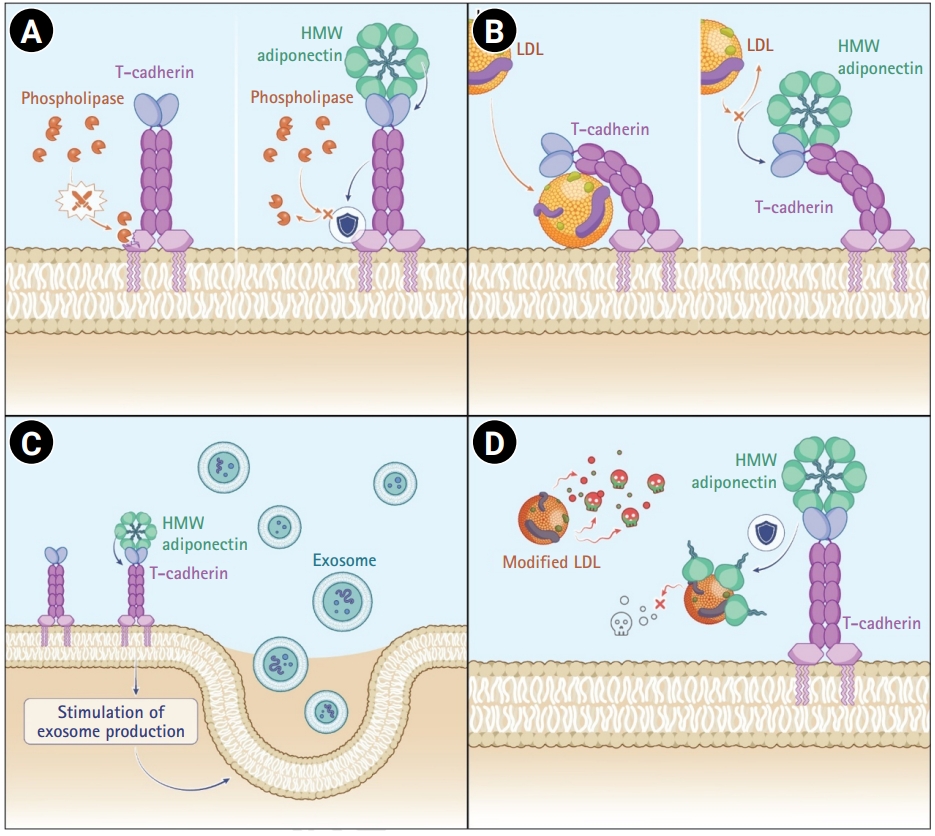
Cardiovascular disease, particularly ischemic heart disease, remains a leading cause of death worldwide. Although advances in pharmacological and device-based therapies have improved clinical outcomes, effective strategies for myocardial repair and regeneration remain limited. T-cadherin, a glycosylphosphatidylinositol-anchored atypical cadherin, has recently been identified as a functional receptor for both low-density lipoprotein cholesterol and adiponectin, a cardioprotective adipokine. Notably, the interaction between T-cadherin and adiponectin has emerged as a key regulator of exosome biogenesis and paracrine signaling within cardiovascular tissues. Exosomes are nanosized extracellular vesicles that carry protective molecular cargo, including microRNAs and proteins, and contribute to anti-inflammatory, antifibrotic, and angiogenic effects in the ischemic myocardium. However, their clinical translation is challenged by factors such as variability in yield, heterogeneity of exosome populations, and inefficient tissue targeting. Enhancing endogenous exosome production through the T-cadherin–adiponectin pathway may therefore offer a novel cell-free therapeutic strategy. This review explores the biological roles of T-cadherin and adiponectin in cardiovascular diseases, their regulatory influence on exosome formation, and the future potential of leveraging this axis for myocardial repair and regeneration.
[English]
[English]
Amiodarone has been widely used for supraventricular and ventricular arrhythmias and many patients benefit from its effectiveness in treating potentially life-threatening arrhythmias. However, this drug can cause multi-organ toxicity, including amiodarone-induced pulmonary toxicity (APT). Not only does amiodarone have a long half-life but also is lipophilic and therefore can easily accumulate in tissues. Hence, it is difficult to monitor therapeutic levels and side effects, making it difficult to predict toxicities. In this case, we describe multi-organ complications secondary to amiodarone use, especially APT combined with pneumonia with atypical pathogens and pulmonary hemorrhage. The patient reached a high cumulative dose of amiodarone despite a low maintenance dose of amiodarone. This case highlights an unusual presentation of APT with multi-organ toxicity and we review articles regarding the association between the cumulative dose of amiodarone and amiodarone-induced toxicities. Citations Citations to this article as recorded by
[English]
Antiphospholipid antibody syndrome (APS) is characterized by raised levels of antiphospholipid antibodies (aPL), in association with thrombosis, recurrent fetal loss, and thrombocytopenia. Development of APS is related with idiopathic origin, autoimmune disease, malignancy and, on rare occasions, infection. However, in secondary APS combined with bacterial infections, aPL is usually shown with low titer and rarely associated with thrombotic events. A 52-year-old male was admitted due to pneumonia and multiple hepatosplenic abscesses. He had been treated with proper antibiotics, but he presented ascites and sudden variceal bleeding because of portal vein thrombosis. The bleeding was controlled by endoscopic variceal ligation. Acute portal vein thrombosis was successfully managed by low molecular weight heparin and hepatosplenic abscesses were completely resolved by antibiotics. This case suggests that systemic bacterial infection in immunocompetent patients possibly develops into secondary APS.
[English]
This study designed to find the differences of left ventricular (LV) geometry in acute myocardial infarction (AMI) between ST elevation myocardial infarction (STEMI) and non ST elevation myocardial infarction (NSTEMI) and the occurrences of adverse outcome according to the LV geometry. Comprehensive echocardiographic analyses were performed in 256 patients with AMI. The left ventricular mass index (LVMI) and relative wall thickness (RWT) were calculated. LV geometry were classified into 4 groups based on RWT and LVMI: normal geometry (normal LVMI and normal RWT), concentric remodeling (normal LVMI and increased RWT), eccentric hypertrophy (increased LVMI and normal RWT), and concentric hypertrophy (increased LVMI and increased RWT). Cox proportional hazards models were used to evaluate the relationships among LV geometry and clinical outcomes. Patients with NSTEMI were more likely to have diabetes mellitus, hypertension, heart failure, stroke and previous myocardial infarction. By the geometric type, patients with NSTEMI were more likely to have eccentric hypertrophy (n=51, 34.7% vs. n=24, 22.0%, P=0.028). There was no significantly different adverse outcome between STEMI and NSTEMI patients. Fifteen patients (5.9%, 7 female [46.7%]) died and the median duration of survival was 10 days (range, 1 to 386 days). Concentric hypertrophy carried the greatest risk of all cause mortality (hazard ratios, 5.83; 95% confidence interval, 1.04 to 32.7). NSTEMI patients had more likely to have eccentric hypertrophy but adverse outcome after AMI was not different between STEMI and NSTEMI patients. Concentric hypertrophy had the greatest risk of short term mortality.
[English]
Bechet's disease(BD) is a chronic inflammatoroy condition involving several organs including gastrointestinal tract. Gastrointestinal tracts involvement in BD has been identified throughout the entire alimentary tract and commonly accompanies ulcerative lesions in the small and large bowel. It is debatable whether BD could be included among seronegative spondyloarthropathy (SPA).SPA usually occurs without overt sign of intestinal inflammation, but significant number of patients have asymptomatic intestinal inflammation, usually affecting ileum. Since most patients with SPA including BD are treated with NSAIDS. However, NSAID may play a role in aggravation or provocation of intestinal inflammation. Special attention to asymptomatic intestinal inflammation is needed, especially when NSAIDs are used for management of arthritic symptom in SpA. We experienced a case of BD which was complicated by a massive small bowel bleeding precipitated by NSAID use.
|
|

