Department of Surgery, Seoul National University College of Medicine, Seoul, Korea
*Corresponding author : Nam-Joon Yi, Department of
Surgery, Seoul National University College of Medicine, 103 Daehak-ro,
Jongno-gu, Seoul 03080, Korea. Tel: 82-2-2072-2318, Fax: 82-2-766-3975, E-mail:
gsleenj@snu.ac.kr
• Received: February 28, 2022 • Revised: April 14, 2022 • Accepted: April 14, 2022
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Small-for-size syndrome (SFSS) is a critical complication of partial liver
transplantation, particularly in adult-to-adult living donor liver
transplantation (ALDLT) using a small graft. Minimally required liver graft size
for a successful ALDLT is classically 40% of a standard recipient’s liver
volume or 0.8% of recipient body weight. Recent progress in perioperative care
and technical improvement push the lower limit of safe graft size to 25% of the
recipient’s standard liver volume or 0.6% of the graft versus recipient
weight ratio although this is an ongoing debate. The clinical manifestations of
SFSS include various symptoms and signs related to graft dysfunction and portal
hypertension in patients with small grafts. The risk factors for SFSS include
poor preoperative patient condition, including portal pressure, surgical
techniques to reduce portal pressure, and graft quality and size. Hence, various
approaches have been explored to modulate inflow and pressure to a small graft
and to decrease the outflow block to alleviate this SFSS as well as the
selection of a patient and graft. Additionally, recent research and efforts to
prevent and treat SFSS are reviewed. (Ewha Med J
2022;45(2):29-34)
Liver transplantation (LT) is a definite and ultimate treatment alternative for
end-stage and metabolic liver diseases [1-3]. Donor shortages push the
boundaries of marginal donors in deceased donor liver transplantation and living
donors worldwide. In living donor liver transplantation (LDLT), the safety of both
recipients and donors is in line [4].
Definitions of Small for Size Syndrome
Small-for-size syndrome (SFSS) is a critical complication of LT using a partial
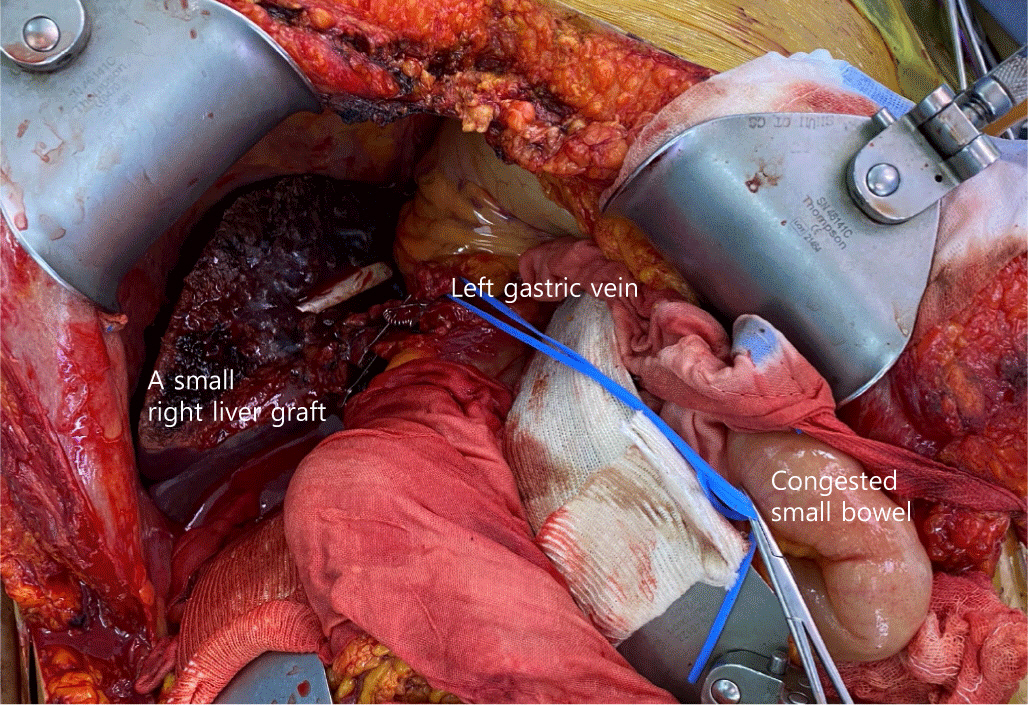
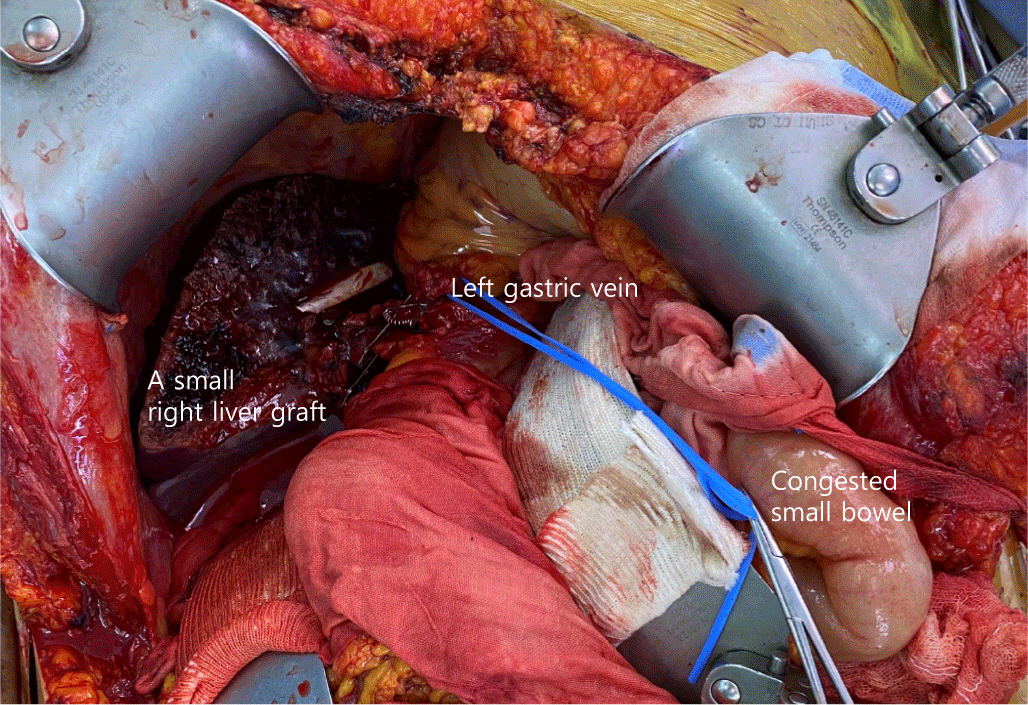
graft, particularly in cases of adult-to-adult ALDLT using a small graft (Fig. 1). In general, small-for-size graft (SFSG)
corresponds to a graft weight <0.8% of recipient weight or a graft volume
<40% of recipient’s standard liver volume (SLV) [5-8]. Recent progress in
perioperative care and technical improvement in partial LT, minimally required liver
graft volume for successful transplantation is an ongoing debate and has decreased
to 0.6% graft versus recipient weight ratio (GRWR) (approximately 25% of the
recipient’s SLV).
Fig. 1.
A small partial graft during adult-to-adult living donor liver
transplantation. The patient has undergone a small right liver graft with a
0.7% graft-versus-recipient weight ratio.
The definition of SFSS varies among transplant centers. Persistent portal
hypertension and hyperperfusion after SFSG transplantation have been identified as
the main factors in this clinical syndrome [9,10]. Nevertheless, the SFSS is
a multifaceted event. Typical clinical manifestations of SFSS are consequences of
portal hypertension and graft dysfunction, presenting as more than two of the
following on 3 consecutive days: (1) long-standing uncontrolled ascites (>1
L/day), (2) hyperbilirubinemia (total bilirubin >5 mg/dL), (3) coagulopathy
(International normalized ratio >2), and (4) encephalopathy (≥grade 3)
during the first postoperative week after transplantation and after the exclusion of
other causes, such as vascular or biliary complications or rejection. Other symptoms
or signs of portal hypertension can also be addressed. These manifestations can
disappear or improve compared with the pre-transplantation status after graft
functioning.
The factors associated with SFSS include preoperative patient condition, the natural
development of varices, medical or surgical efforts to reduce portal pressure, no
pressure gradient between the hepatic vein and inferior vena cava (or right atrium),
graft quality, and graft size.
Small for Size Syndrome Pathophysiology
The main pathophysiology of SFSS is shear stress, which leads to sinusoidal
microcirculatory disturbances caused by excessive portal pressure [11]. In the case of a small graft, repair and
regeneration cannot overcome the damage and maintain liver function very early after
transplantation. If this damage is permanent or severe, the outcome of SFSS is poor,
leading to graft failure and patient death.
The early microscopic features of SFSS are ischemia related to arterial vasospasm
and/or thrombosis and render hepato-cytes vulnerable to the subsequent oxidative
stress leading to endothelial damage, cholestasis, hepatocyte ballooning, and
ductular reaction, as well as bile duct necrosis. The late features include nodular
regenerative hyperplasia [8,12,13].
Outcomes of Small for Size Syndrome
Early reports on SFSS demonstrated poor patient and graft survival outcomes. Patients
with both elevated portal pressure (≥20 [range 18-25] mmHg) and SFSG
(≤0.8% GRWR) showed significantly worse survival outcomes, bacteremia, and
longer hospital stays. If the pre-transplant patient’s condition is worse,
such as old age and high model for end-stage liver disease (MELD) score,
post-transplant outcomes would be much worse [5,8,11,14].
Recent reports regarding the outcomes of SFSG have shown promising results (Table 1). Small grafts are associated with poor
short-term outcomes. However, the long-term outcome was not inferior in patients
with small grafts [15]. Therefore,
prevention, early detection, and interventions to attenuate SFSS are important.
Various approaches have been explored to modulate inflow and pressure to a small
graft and to decrease the outflow block to alleviate this SFSS. Along with these
efforts, strict matching criteria for patient and donor pairs are also
important.
Table 1.
The outcomes of liver transplantations using a SFSG
SFSG, small for size graft; SFSS, small for size syndrome; OR, odds
ratio; CI, confidence interval; GRWR, graft-versus-recipient weight
ratio; GV, graft volume; SLV, standard liver volume.
*3-yr follow up.
Prevention and Management to Improve the Outcome of Small for Size Graft
1. Prevention of small for size syndrome
The management goal of the SFSS is to avoid SFSS. SFSS does not always occur in
patients with SFSG. This can be prevented by cautiously matching the donor and
recipient and applying surgical or medical modifications. Prevention of
damage-related SFSG on portal hypertension is an ideal solution [8,16].
The principles for avoiding SFSS are as follows: First, it does not consider
multiple risks of SFSS at once. There are several known factors related to SFSS:
aged donor, graft steatosis, longer ischemic time, left small liver than right
small liver, and recipient with a high MELD score [8,14,16]. For example, if the patient’s
condition is poor, sufficient graft volume from a young donor with a short
ischemic time rather than a small left liver graft is a better alternative
[11,14,17].
Second, portal pressure is attenuated after accurate measurement of portal
pressure during transplantation [14,16,17-20]. Several surgical
procedures can reduce the portal pressure and alleviate potential SFSS.
Remaining natural varices or creating transient portosystemic shunts can reduce
portal hypertension during the early period of graft regeneration. However,
portal steal syndrome can sometimes ruin sufficient inflow to the graft.
Accurate measurement of portal pressure and flow via the inferior mesenteric
vein or the direct portal puncture technique helps decide whether to proceed
with these procedures [18]. After
regeneration of a small graft, surgical or interventional shunt occlusion can be
performed to improve the long-term graft outcomes and prevent variceal
complications. An indirect method to reduce portal pressure is to reduce splenic
venous inflow to the portal vein. Splenomegaly and splenic artery hypertrophy
are common in patients with end-stage liver disease and portal hypertension. In
that case, splenectomy, splenic artery ligation, or splenic devascularization
can reduce portal pressure [9,16,21,22].
Third, we used the entire transplanted graft without ischemia or congestion, as
possible [9,23,24]. To avoid
ischemia of the small graft, the surgeon should reconstruct all the inflows.
During hepatectomy and graft implantation, meticulous surgery is mandatory to
prevent the use of inotropic agents. To avoid congestion of the small graft,
drain all the outflow of the area >20% of the graft, segment 5 veins,
segment 8 veins, and right inferior hepatic veins in the right graft, and
segment 1 vein in the left graft with the caudate lobe. To improve outflow, the
outlet of the hepatic vein should be sufficiently large to transfer the
oscillation of the heartbeat. Additionally, physiological obstruction related to
hemodynamic changes such as high right atrial pressure or central venous
pressure should be properly managed during the reperfusion period.
Finally, dual graft implantation and auxiliary orthotopic partial liver
transplantation (APOLT) or heterotopic auxiliary partial liver transplantation
(HALT) with future native liver hepatectomy, the so-called resection and partial
liver segment 2/3 transplantation with delayed total hepatectomy (RAPID), can be
another option to avoid SFSS [24-32]. The APOLT technique was applied to
chronic liver disease in the late 90s during ALDLT to avoid SFSS and to protect
donor safety using a small graft for sufficient future remnant volume in Asian
countries (Fig. 2). Recently, this
technique has been applied to patients with colorectal liver-only metastasis
without portal hypertension who do not receive an adequate volume of deceased
donor graft but can get a split left lateral section.
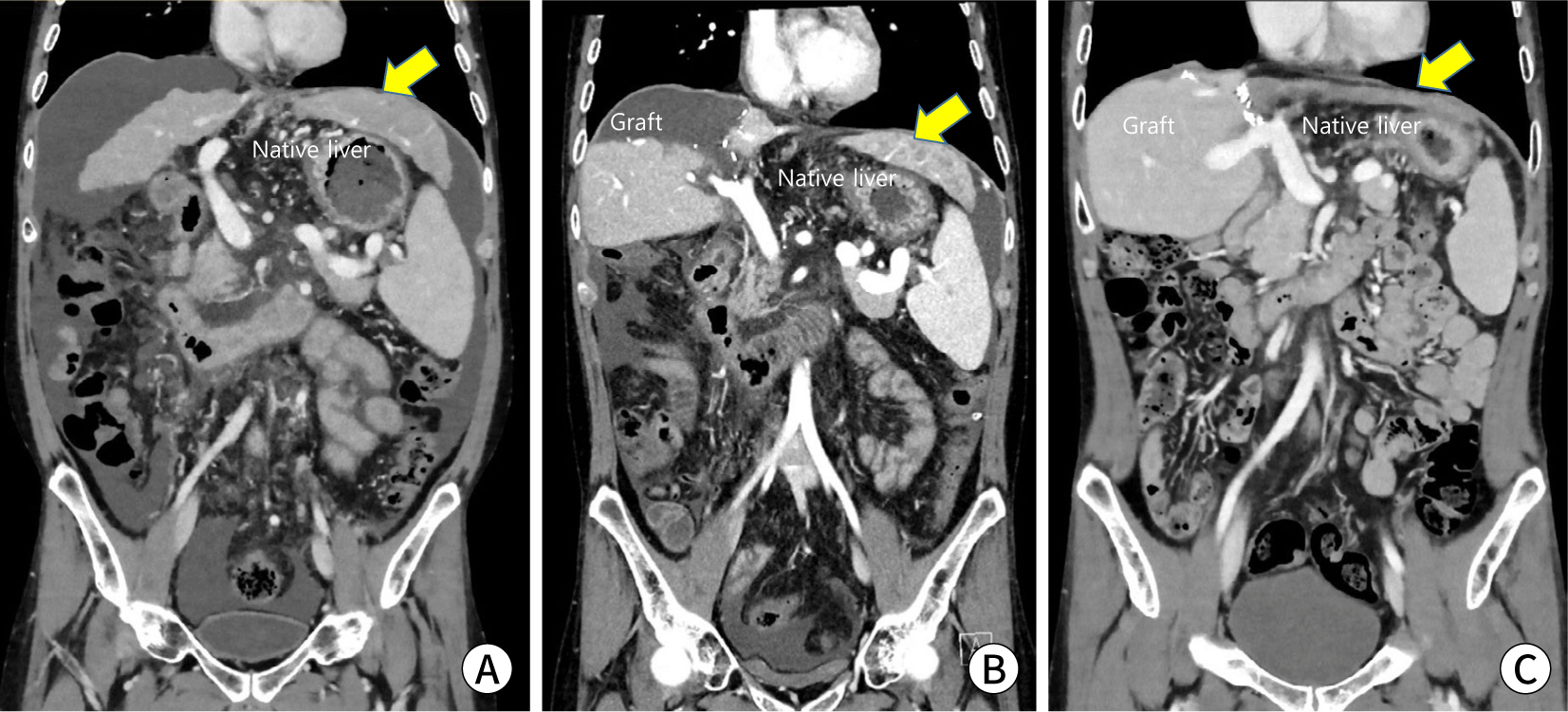
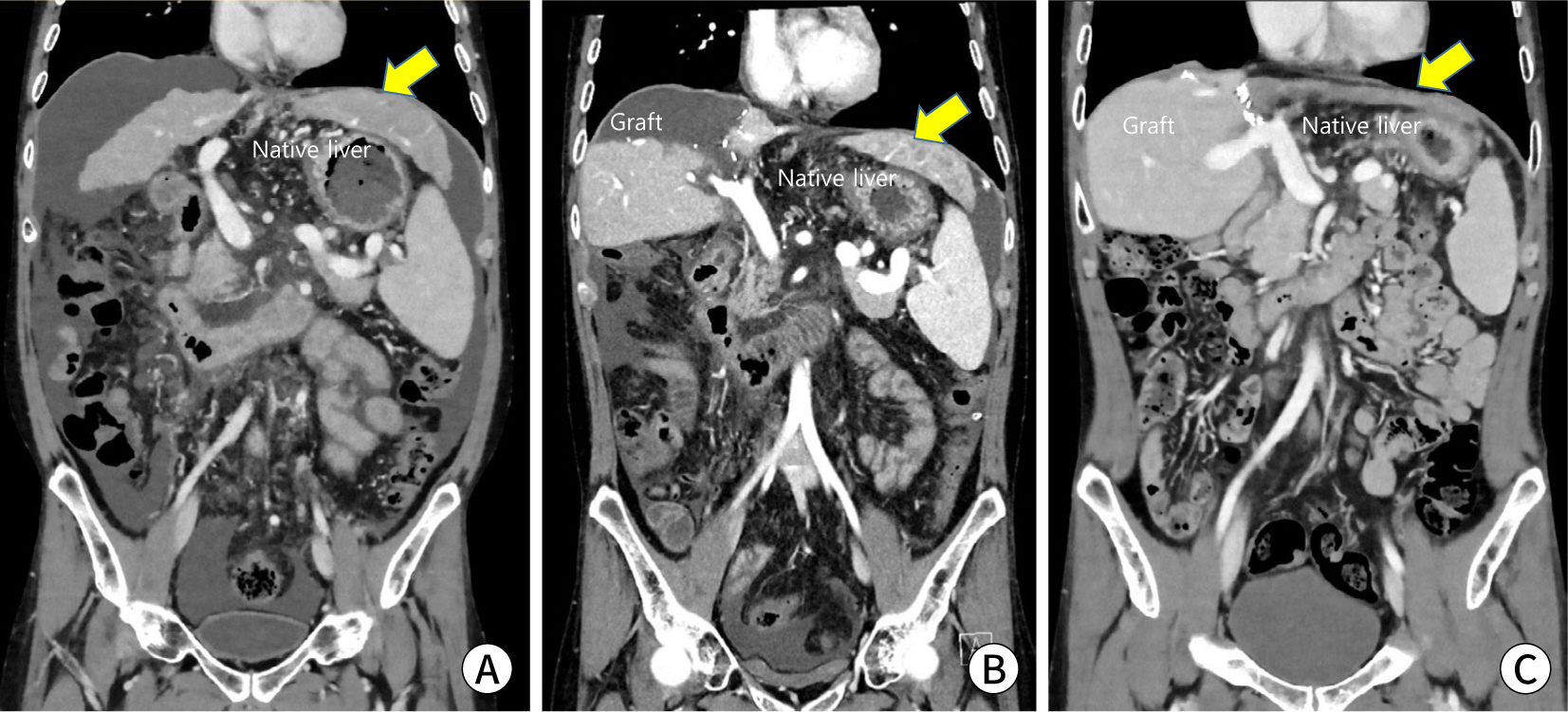
Fig. 2.
Auxiliary partial orthotopic liver transplantation to prevent the
small-for-size syndrome. A 36-yr-old patient with Wilson’s
disease has undergone living-donor liver transplantation from a
54-yr-old mother using a right posterior section graft. The
graft-versus-recipient weight ratio is 0.64%. He has undergone a native
liver hepatectomy 11 mo after transplantation. (A) A preoperative
recipient computed tomography (CT) scan. (B) A CT scan of postoperative
day 9. (C) A CT scan of postoperative 11 mo.
2. Management after small for size syndrome development
Regardless of these efforts during the operation, the SFSS can develop.
Management goals include medical management of portal hypertension and graft
support for acute liver failure. The medical reduction of portal pressure is
similar to that of the pretransplant management of portal hypertension. Fluid
balance and ascites control are basic concepts. Intervention radiology can play
a role in splenic artery embolization by reducing portal pressure via flow
reduction (Fig. 3).
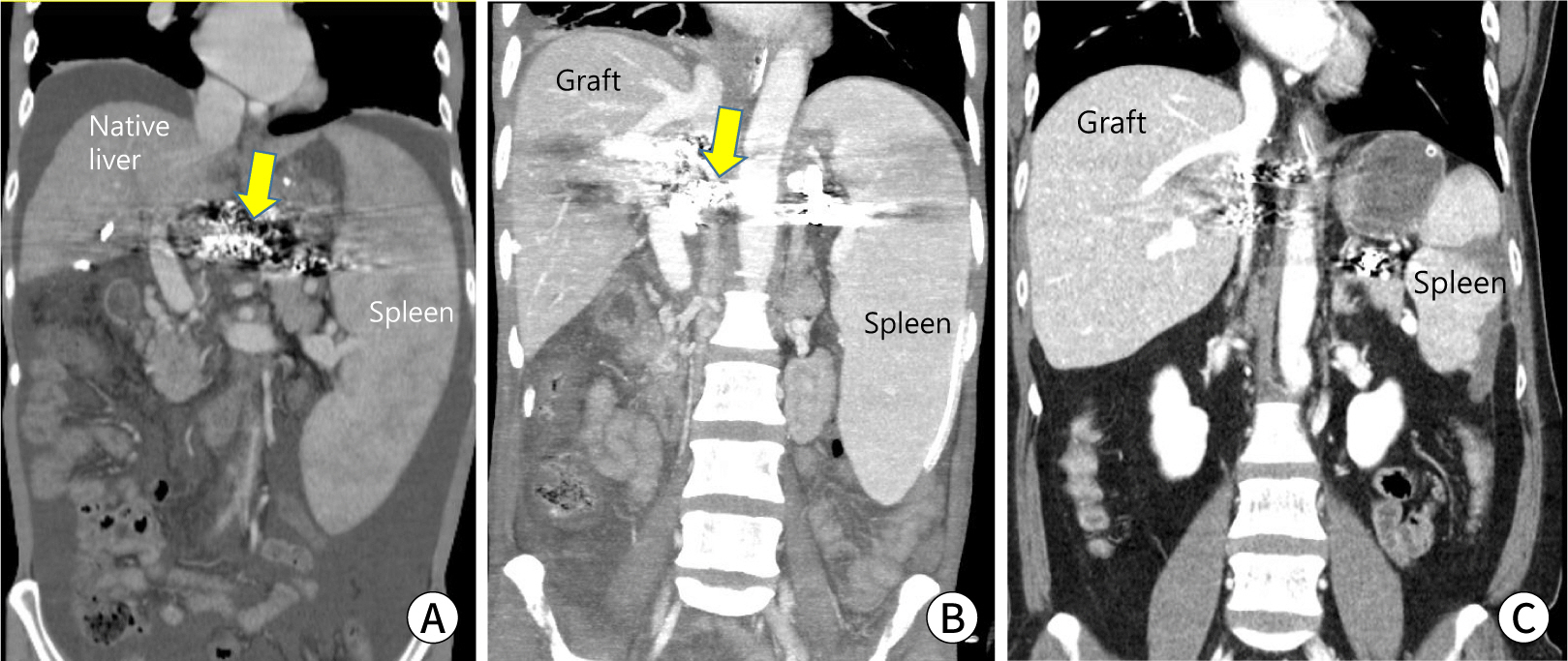
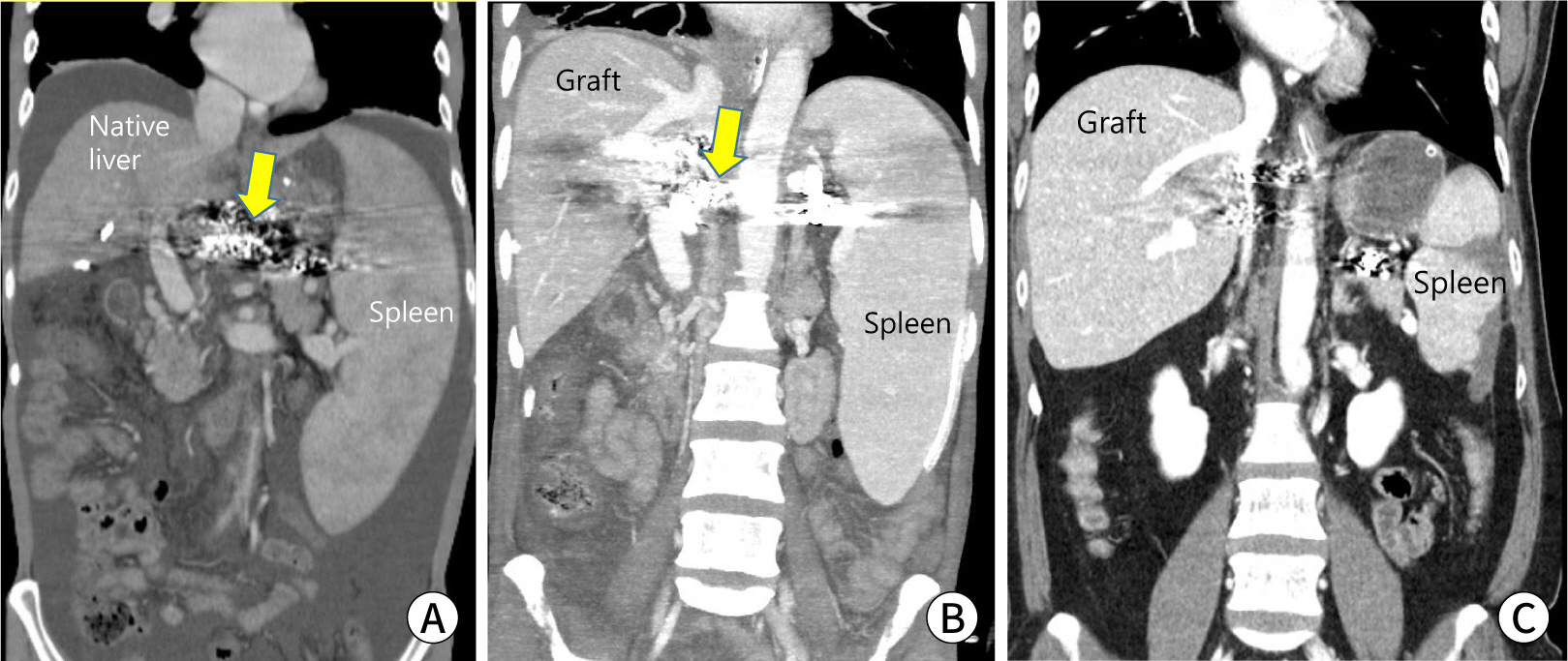
Fig. 3.
Post-transplant splenic arterial embolization to reduce portal
hypertension. A 40-yr-old woman with hepatitis B-related liver cirrhosis
with the hepatorenal syndrome and uncontrolled ascites underwent
living-donor liver transplantation from his 35-yr-old wife using a right
liver graft. He underwent gastrorenal shunt occlusion before
transplantation to control variceal bleeding and encephalopathy. One mo
after transplantation, the patient underwent partial occlusion of the
splenic artery because of uncontrolled ascites related to small-for-size
syndrome (arrow, material for gastrorenal shunt occlusion). (A) A
preoperative recipient computed tomography (CT) scan. (B) A CT scan of
postoperative day 7. (C) A CT scan 2 yrs after transplantation.
The SFSS can be overcome after the early period of graft regeneration. If varices
or shunt flow remains, we should wait for a minimum of 2 weeks (10-21 days after
transplantation) for graft regeneration. Delayed closure would be helpful for
the restoration of graft function. Delayed native liver hepatectomy in cases of
APOLT (or HALT, RAPID) can be performed during this period [25-31].
Conclusion
SFSS can occur in any case when using a small partial graft. However, a better
understanding of SFSS and the recent progress in perioperative management and
surgical techniques can push the boundary of a small graft. Before permanent damage
of a small graft, prevention and early detection of SFSS can save patients with only
the alternative for a small graft.
References
1. Chen CL, Fan ST, Lee SG, Makuuchi M, Tanaka K. Living-donor liver transplantation: 12 years of experience in
Asia. Transplantation 2003;75:S6-S11.
2. Hashikura Y, Makuuchi M, Kawasaki S, Matsunami H, Ikegami T, Nakazawa Y, et al. Successful living-related partial liver transplantation to an
adult patient. Lancet 1994;343:1233-1234.
3. Tanaka K, Uemoto S, Tokunaga Y, Fujita S, Sano K, Nishizawa T, et al. Surgical techniques and innovations in living related liver
transplantation. Ann Surg 1993;217:82-91.
5. Kiuchi T, Kasahara M, Uryuhara K, Inomata Y, Uemoto S, Asonuma K, et al. Impact of graft size mismatching on graft prognosis in liver
transplantation from living donors. Transplantation 1999;67:321-327.
6. Kiuchi T, Tanaka K, Ito T, Oike F, Ogura Y, Fujimoto Y, et al. Small-for-size graft in living donor liver transplantation: how
far should we go? Liver Transpl 2003;9:S29-S35.
7. Lo CM, Fan ST, Liu CL, Chan JK, Lam BK, Lau GK, et al. Minimum graft size for successful living donor liver
transplantation. Transplantation 1999;68:1112-1116.
8. Masuda Y, Yoshizawa K, Ohno Y, Mita A, Shimizu A, Soejima Y. Small-for-size syndrome in liver transplantation: definition,
pathophysiology and management. Hepatobiliary Pancreat Dis Int 2020;19:334-341.
9. Ben-Haim M, Emre S, Fishbein TM, Sheiner PA, Bodian CA, Kim-Schluger L, et al. Critical graft size in adult-to-adult living donor liver
transplantation: impact of the recipient’s disease. Liver Transpl 2001;7:948-953.
11. Yi NJ, Suh KS, Cho YB, Lee HW, Cho EH, Cho JY, et al. The right small-for-size graft results in better outcomes than
the left small-for-size graft in adult-to-adult living donor liver
transplantation. World J Surg 2008;32:1722-1730.
12. Emond JC, Renz JF, Ferrell LD, Rosenthal P, Lim RC, Roberts JP, et al. Functional analysis of grafts from living donors: implications
for the treatment of older recipients. Ann Surg 1996;224:544-554.
13. Demetris AJ, Kelly DM, Eghtesad B, Fontes P, Wallis Marsh J, Tom K, et al. Pathophysiologic observations and histopathologic recognition of
the portal hyperperfusion or small-for-size syndrome. Am J Surg Pathol 2006;30:986-993.
14. Yi NJ, Suh KS, Lee HW, Shin WY, Kim J, Kim W, et al. Improved outcome of adult recipients with a high model for
end-stage liver disease score and a small-for-size graft. Liver Transpl 2009;15:496-503.
15. Ma KW, Wong KHC, Chan ACY, Cheung TT, Dai WC, Fung JYY, et al. Impact of small-for-size liver grafts on medium-term and
long-term graft survival in living donor liver transplantation: a
meta-analysis. World J Gastroenterol 2019;25:5559-5568.
17. Chan SC, Fan ST, Lo CM, Liu CL. Effect of side and size of graft on surgical outcomes of
adult-to-adult live donor liver transplantation. Liver Transpl 2007;13:91-98.
18. Ito T, Kiuchi T, Yamamoto H, Oike F, Ogura Y, Fujimoto Y, et al. Changes in portal venous pressure in the early phase after living
donor liver transplantation: pathogenesis and clinical
implications. Transplantation 2003;75:1313-1317.
19. Troisi R, Cammu G, Militerno G, De Baerdemaeker L, Decruyenaere J, Hoste E, et al. Modulation of portal graft inflow: a necessity in adult
living-donor liver transplantation? Ann Surg 2003;237:429-436.
20. Botha JF, Langnas AN, Campos BD, Grant WJ, Freise CE, Ascher NL, et al. Left lobe adult-to-adult living donor liver transplantation:
small grafts and hemiportocaval shunts in the prevention of small-for-size
syndrome. Liver Transpl 2010;16:649-657.
21. Moon DB, Lee SG, Hwang S, Ahn CS, Kim KH, Ha TY, et al. Splenic devascularization can replace splenectomy during adult
living donor liver transplantation: a historical cohort
study. Transpl Int 2019;32:535-545.
22. Ito K, Akamatsu N, Ichida A, Ito D, Kaneko J, Arita J, et al. Splenectomy is not indicated in living donor liver
transplantation. Liver Transpl 2016;22:1526-1535.
23. Yi NJ, Suh KS, Lee HW, Cho EH, Shin WY, Cho JY, et al. An artificial vascular graft is a useful interpositional material
for drainage of the right anterior section in living donor liver
transplantation. Liver Transpl 2007;13:1159-1167.
24. Lee SG. A complete treatment of adult living donor liver transplantation:
a review of surgical technique and current challenges to expand indication
of patients. Am J Transplant 2015;15:17-38.
25. Kasahara M, Kiuchi T, Uryuhara K, Takakura K, Egawa H, Asonuma K, et al. Auxiliary partial orthotopic liver transplantation as a rescue
for small-for-size grafts harvested from living donors. Transpl Proc 1998;30:132-133.
26. Kasahara M, Takada Y, Egawa H, Fujimoto Y, Ogura Y, Ogawa K, et al. Auxiliary partial orthotopic living donor liver transplantation:
Kyoto University experience. Am J Transplant 2005;5:558-565.
27. Lee SG, Hwang S, Park KM, Kim KH, Ahn CS, Lee YJ, et al. Seventeen adult-to-adult living donor liver transplantations
using dual grafts. Transpl Proc 2001;33:3461-3463.
28. Soejima Y, Taketomi A, Ikegami T, Yoshizumi T, Uchiyama H, Yamashita Y, et al. Living donor liver transplantation using dual grafts from two
donors: a feasible option to overcome small-for-size graft
problems? Am J Transplant 2008;8:887-892.
29. Konigsrainer A, Templin S, Capobianco I, Konigsrainer I, Bitzer M, Zender L, et al. Paradigm shift in the management of irresectable colorectal liver
metastases: living donor auxiliary partial orthotopic liver transplantation
in combination with two-stage hepatectomy (LD-RAPID). Ann Surg 2019;270:327-332.
30. Lim C, Turco C, Balci D, Savier E, Goumard C, Perdigao F, et al. Auxiliary liver transplantation for cirrhosis: from APOLT to
RAPID: a scoping review. Ann Surg 2022;275:551-559.
31. Ravaioli M, Brandi G, Siniscalchi A, Renzulli M, Bonatti C, Fallani G, et al. Heterotopic segmental liver transplantation on splenic vessels
after splenectomy with delayed native hepatectomy alter graft regeneration:
a new technique to enhance liver transplantation. Am J Transplant 2021;21:870-875.
32. Cho JY, Suh KS, Kwon CH, Yi NJ, Kim MA, Jang JJ, et al. Auxiliary partial orthotopic living donor liver transplantation
in a patient with alcoholic liver cirrhosis to overcome donor
steatosis. Transpl Int 2006;19:424-429.
Prevention and Management of Small-for-Size Syndrome of Liver
Transplantation
Fig. 1.
A small partial graft during adult-to-adult living donor liver
transplantation. The patient has undergone a small right liver graft with a
0.7% graft-versus-recipient weight ratio.
Fig. 2.
Auxiliary partial orthotopic liver transplantation to prevent the
small-for-size syndrome. A 36-yr-old patient with Wilson’s
disease has undergone living-donor liver transplantation from a
54-yr-old mother using a right posterior section graft. The
graft-versus-recipient weight ratio is 0.64%. He has undergone a native
liver hepatectomy 11 mo after transplantation. (A) A preoperative
recipient computed tomography (CT) scan. (B) A CT scan of postoperative
day 9. (C) A CT scan of postoperative 11 mo.
Fig. 3.
Post-transplant splenic arterial embolization to reduce portal
hypertension. A 40-yr-old woman with hepatitis B-related liver cirrhosis
with the hepatorenal syndrome and uncontrolled ascites underwent
living-donor liver transplantation from his 35-yr-old wife using a right
liver graft. He underwent gastrorenal shunt occlusion before
transplantation to control variceal bleeding and encephalopathy. One mo
after transplantation, the patient underwent partial occlusion of the
splenic artery because of uncontrolled ascites related to small-for-size
syndrome (arrow, material for gastrorenal shunt occlusion). (A) A
preoperative recipient computed tomography (CT) scan. (B) A CT scan of
postoperative day 7. (C) A CT scan 2 yrs after transplantation.
Fig. 1.
Fig. 2.
Fig. 3.
Prevention and Management of Small-for-Size Syndrome of Liver
Transplantation
The outcomes of liver transplantations using a SFSG
Year of study
Study
Country
Definition
Number of SFSG group
Number of control group
Incidence of SFSS (%)
Short-term mortality in SFSG
Long-term mortality (OR, 90% CI)
2008
Yi
Korea
<0.8% GRWR
29
-
-
0% in Right 33% in Left
-
2008
Ikegami
Japan
<35% GV/SLV
33
87
0
12.5% (1 yr)
3.25 (1.29-8.18)
2009
Selzner
Canada
<0.8% GRWR
22
249
9
4.5% (30 days)
0.82 (0.27-2.60)
2010
Moon
Korea
<0.8% GRWR
35
392
5.7
-
1.33 (0.60-2.95)
2014
Lee
Korea
<0.8% GRWR
50
267
8
2% (1 yr)
1.61 (0.72-3.63)*
2015
Au
HongKong
<35% GV/SLV
21
212
-
-
1.61 (0.51-5.15)
2015
Liu
China
<0.8% GRWR
65
181
11
7.7% (30 days)
1.23 (0.65-2.34)
2016
Ikegami
Japan
<35% GV/SLV
88
119
11.4
-
0.69 (0.28-1.72)
SFSG, small for size graft; SFSS, small for size syndrome; OR, odds
ratio; CI, confidence interval; GRWR, graft-versus-recipient weight
ratio; GV, graft volume; SLV, standard liver volume.
*3-yr follow up.
Table 1.
The outcomes of liver transplantations using a SFSG
SFSG, small for size graft; SFSS, small for size syndrome; OR, odds
ratio; CI, confidence interval; GRWR, graft-versus-recipient weight
ratio; GV, graft volume; SLV, standard liver volume.