This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
This review describes a psychological support service designed to address
post-traumatic stress disorder in workers impacted by workplace injuries,
assisting in their recovery and facilitating their return to work. It explores
the rationale and context behind establishing trauma counseling centers for
these individuals, along with the status, roles, future directions, and
recommendations for these centers. The review details the operational framework
and functions of the workplace injury trauma management program, the scope of
the impacts of such injury, the groups targeted for crisis intervention, and the
psychological interventions tailored to each stage of recovery. Initiated as a
pilot project in 2018, trauma counseling centers for workers have gradually
become more common, with 23 centers in operation across Korea as of 2024.
Insights from workplace disasters and policy interventions
The tragic fire at the primary battery facility in Hwaseong in 2024, which
resulted in numerous fatalities, serves as a grim reminder of past workplace
accidents. These include the crane collapse in 2017, the fatal accident
involving a conveyor at a power plant in Taean in 2018, and the fire at a
logistics center in Icheon in 2020. These incidents have left deep scars and
reignited public discourse on the importance of workplace safety. Despite a
decreasing trend in the rate of fatal injuries in South Korea since 2014,
the country’s rates remain quite high compared to other
industrialized nations [1]. For
instance, in 2023, South Korea’s fatal injury rate was 0.39 per
10,000 employees, which is 2.3 times higher than the average rate of 1.66
per 100,000 employees reported by EU member countries in 2022 [2].
Under Korea’s Occupational Safety and Health Act, a workplace injury
is defined as “any death, injury, or disease of a person who provides
labor caused by structures, equipment, raw materials, gas, vapor, powder,
dust, etc. related to [their] duties, or by [their] work or other
duties.” A “serious accident” is a severe incident that
involves one or more fatalities or affects many victims [3]. Since the implementation of the
Serious Accidents Punishment Act in 2022, which applies to companies with 50
or more employees, increased attention has been paid to workplace safety
systems and accident prevention [4,5].
Workplace accidents result in not only the loss of life and physical and
emotional suffering for workers but also economic and social costs,
including property damage and loss of productivity. For instance, the 2017
crane collapse at Samsung Heavy Industries caused six deaths and severely
injured 25 workers, with over 1,000 people witnessing the tragedy either
directly or indirectly. Similarly, the suicide of a stablehand in July 2017
highlighted the mental health risks that workers face, marking a pivotal
moment for heightened awareness of mental health in the workplace [6].
Psychological impact of serious workplace accidents
The psychological trauma experienced by workers exposed to serious workplace
accidents varies depending on the severity and proximity of their exposure.
Individuals who directly witness such events are more likely to face severe
psychological effects than those who do not witness them firsthand [7]. The psychological consequences of
experiencing catastrophic workplace accidents can be categorized as
follows:
1) Psychological disorders stemming from trauma
Traumatic experiences, such as workplace disasters, can trigger a range
of mental health issues, including dissociative symptoms like
depersonalization and derealization [8,9]. If these issues
are not addressed, they may lead to post-traumatic stress disorder
(PTSD), depression, panic disorders, substance abuse, and anxiety
disorders [10–12]. Survivors may experience
insomnia, intrusive memories, nightmares, impaired concentration, and
hypersensitivity to noise. They may also grapple with feelings of guilt,
hopelessness, and emotional detachment from others [13].
2) Intrusive responses and emotional dysregulation
Trauma survivors often report re-experiencing distressing events, feeling
as if they are being repeatedly exposed to the same incident. Intrusive
symptoms, a hallmark of PTSD, are frequently associated with excessive
alcohol consumption used as a coping mechanism. Research indicates that
individuals with severe early symptoms of PTSD are at increased risk of
problematic drinking and persistent PTSD [14–17].
Workers who have been exposed to workplace accidents frequently report a
lower quality of life, along with higher rates of suicidal thoughts and
depressive symptoms, compared to those who have not experienced such
incidents [18,19]. Factors contributing to this
reduced quality of life include poor sleep, decreased motivation,
depression, and anxiety, with anxiety identified as particularly key
[20].
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,
published by the American Psychiatric Association, recognizes that
experiencing or witnessing traumatic events can result in involuntary,
intrusive memories and prolonged psychological distress [21]. Similarly, the National
Institute for Occupational Safety and Health has identified a range of
symptoms associated with traumatic incident stress. These include chest
pain, difficulty breathing, memory problems, nightmares, anxiety, guilt,
fear, and uncontrollable anger, and are frequently observed following
exposure to catastrophic workplace events [22].
3) Cognitive and social impacts
Trauma resulting from workplace accidents can also impact cognitive
functions and social adaptability. Studies investigating the
neurological effects of trauma have shown that individuals with smaller
hippocampal volumes or larger cavum septum pellucidum 1 month after
trauma exposure tend to exhibit more severe symptoms at both 1 and 14
months post-trauma. These findings highlight the importance of long-term
monitoring, psychological stabilization, and early intervention within
the first year following exposure [23,24].
The severity of disabilities following trauma, alongside mental health
challenges and reduced adaptability, significantly impacts the ability
of workers to return to their jobs and maintain productivity [25,26].
Returning to work: balancing recovery and livelihood
Returning to work is often a primary concern for individuals affected by
industrial accidents. However, the prospect of encountering recurring
traumatic triggers in the workplace presents considerable challenges.
Despite the profound psychological impact of workplace injuries, recovery is
achievable.
Social support plays a critical role in protecting mental health. Research
has demonstrated that social support reduces the likelihood of developing
PTSD, mitigates the effects of substance abuse, and helps preserve mental
well-being, even during crises such as the coronavirus disease 2019 pandemic
[27].
Establishing a robust psychological support system can assist workers in
navigating their trauma and developing resilience, empowering them to move
forward with their lives despite the challenges.
Policy and prevention: addressing trauma at the workplace
Recognizing the urgent need to address trauma resulting from workplace
injuries, Korea has enacted policies aimed at preventing and mitigating PTSD
among workers who have been exposed to serious workplace accidents. In 2018,
the Korea Occupational Safety and Health Agency (KOSHA) initiated a pilot
program for an Occupational Trauma Center, designed to protect the mental
health of workers and facilitate their recovery.
Objectives
This article provides an overview of the establishment, current operations, and
future directions of the Occupational Trauma Center regarding its expanding role
in supporting affected workers and promoting mental health recovery at the
community level.
Ethics statement
As this study is a literature review, it did not require institutional review board
approval or individual consent.
Purpose and status of Occupational Trauma Centers
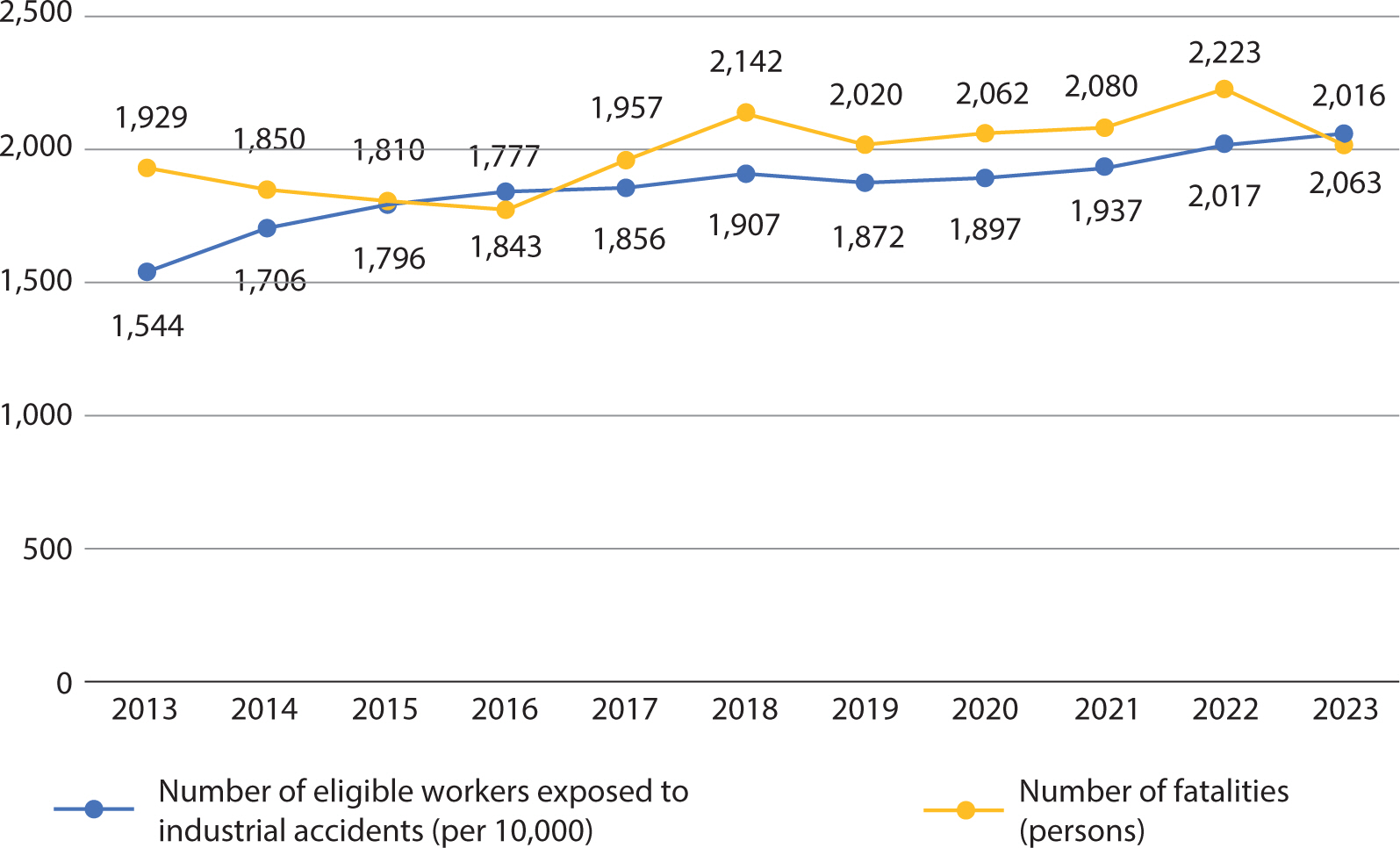
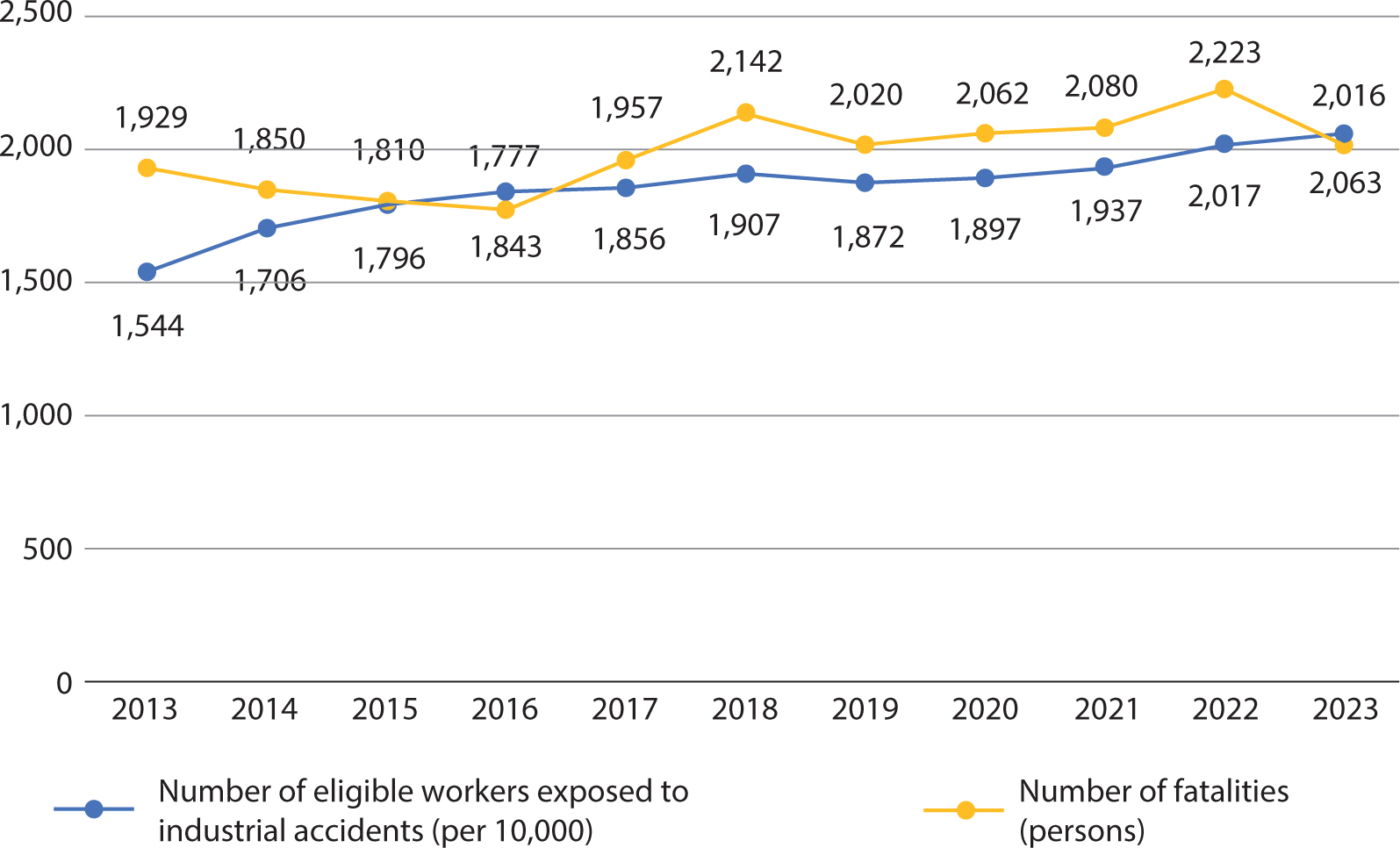
According to data from the Ministry of Employment and Labor, the number of workers
covered by industrial accident compensation insurance has steadily increased
annually, rising from 15.44 million in 2013 to 19.07 million in 2018 before reaching
20.63 million in 2023 (Fig. 1). In the context
of work-related injuries, the approval rate for PTSD claims has increased from two
cases in 2011 to 83 in 2021, representing a 40-fold surge (Table 1). This trend reflects a growing societal recognition of
post-traumatic stress as an occupational disease.
Fig. 1.
Number and rate of fatalities due to industrial accidents. Data from
Ministry of Employment and Labor [1].
Table 1.
Mental health disorders associated with occupational injuries
(2011–2022)
Category
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
Applications
102
127
137
137
165
183
213
268
331
581
720
678
Approvals
26
47
53
47
63
85
126
201
231
396
515
445
Approval rate (%)
25.5
37
38.7
34.3
38.2
46.4
59.2
75
69.8
68.2
71.5
65.6
Depression
14
15
14
17
17
14
52
72
66
113
113
80
Adjustment disorder
2
11
5
11
13
21
32
53
78
162
248
227
Acute stress disorder
4
7
14
3
9
5
8
15
15
23
10
26
Post-traumatic stress disorder
2
7
9
9
14
25
21
36
39
55
83
63
Anxiety disorder
2
1
2
3
2
4
1
5
13
19
21
23
Others
2
6
9
4
8
16
12
20
20
24
40
26
Data from Korea Workers’ Compensation & Welfare Service
[28].
Job trauma refers to the psychological and physical responses—including fear,
anxiety, and anger—that emerge after direct or indirect exposure to a
significant industrial accident or comparable event in the workplace [29]. In 2014, the Worker Health Center in East
Gyeonggi initiated programs aimed at stabilizing acute stress and preventing
post-traumatic stress among manufacturing workers affected by workplace accidents,
whether directly or indirectly. These initiatives highlighted the importance of
psychological interventions in the aftermath of such incidents, prompting the Center
to seek appropriate countermeasures.
In 2017, a crane accident in the heavy industry sector resulted in numerous
casualties and public outcry. At the time, no specialized system had been
implemented to address trauma among workers impacted by such an event. This
large-scale disaster underscored the critical need for occupational trauma
management to alleviate post-traumatic stress and support workers’ return to
their jobs following industrial accidents. In response, a pilot Occupational Trauma
Center was established in Daegu in 2018, with a focus on addressing industrial
accidents throughout the nation for a 2-year period [30]. By 2020, the initiative had expanded to include eight centers
across the country. As of 2024, Korea has a total of 23 such centers operating under
the jurisdiction of KOSHA, which also oversees on-site accident investigations to
ensure effective coordination with affiliated organizations.
Occupational Trauma Centers are located within Worker Health Centers across the
country. Each trauma center is staffed with two counseling psychologists and
equipped with private consultation rooms to promote psychological safety. Table 2 details the annual operational status
of these centers [31].
Table 2.
Operational status of Occupational Trauma Centers in Korea by
year
Year
Number of centers opened
Centers
2018–2019
1
Pilot center with national jurisdiction
(Daegu Occupational Trauma Center)
2020
8
Eastern Gyeonggi, Western Gyeonggi,
Gyeongnam, Gwangju, Bucheon, Daegu, Daejeon, Incheon
Data from Korea Occupational Safety and Health Agency [31].
Occupational Trauma Management Program and operational framework
The Occupational Trauma Management Program is a psychological support initiative
designed to alleviate the emotional impact on workers who have experienced serious
workplace accidents, work-related injuries, or incidents such as a
colleague’s intentional self-harm, workplace violence (including bullying),
and verbal or physical abuse from customers. This program is designed to support
workers in their return to their jobs. In the case of serious workplace accidents,
where the extent of damage and worker exposure may be extensive, timely coordination
of post-incident psychological support is crucial. Following an accident, a rapid
assessment is conducted to evaluate each affected individual’s level of
exposure, the extent of the impact, relationships with injured parties, available
support systems and resources, and the company’s response to the accident.
This ensures that high-risk groups can be prioritized for psychological support.
When a serious workplace accident occurs, referrals can be made through the following
channels:
First, in the event of a serious workplace accident, the local branch (or sub-branch)
of the Ministry of Employment and Labor responsible for investigating the scene may
inform the affected workplace and recommend the implementation of the Occupational
Trauma Management Program. The incident can be referred to the Occupational Trauma
Center if the workplace has 50 or more employees; if two or more fatalities have
occurred, resulting in widespread exposure; or if the accident has generated
substantial public concern. Additionally, if investigators interviewing witnesses of
a significant industrial accident determine that occupational trauma management is
necessary, they have the authority to notify the local KOSHA office (Fig. 2).
Fig. 2.
Operational framework of the occupational trauma management program. Data
from Korea Occupational Safety and Health Agency [28].
Second, when investigating a serious workplace accident, the Central Accident
Investigation Team of KOSHA may recommend and promote the implementation of the
Occupational Trauma Management Program.
Third, the Occupational Trauma Management Program may be activated following a
serious workplace accident or incident if either the workplace or individual workers
recognize the need for occupational trauma management and request psychological
support.
Furthermore, in the event of large-scale accidents—such as the 2020 fire at
the Logistics Center in Icheon or the 2024 fire at a primary battery plant in
Hwaseong—that result in a significant number of casualties and widespread
exposure among workers, response efforts may extend beyond jurisdictional boundaries
through coordinated requests among government ministries [32].
Additionally, it is crucial to regularly monitor KOSHA’s reports on fatal
accidents, regardless of whether a request for occupational trauma management has
been made. Access to up-to-date information about accidents and the number of
victims within the relevant jurisdiction can facilitate rapid intervention.
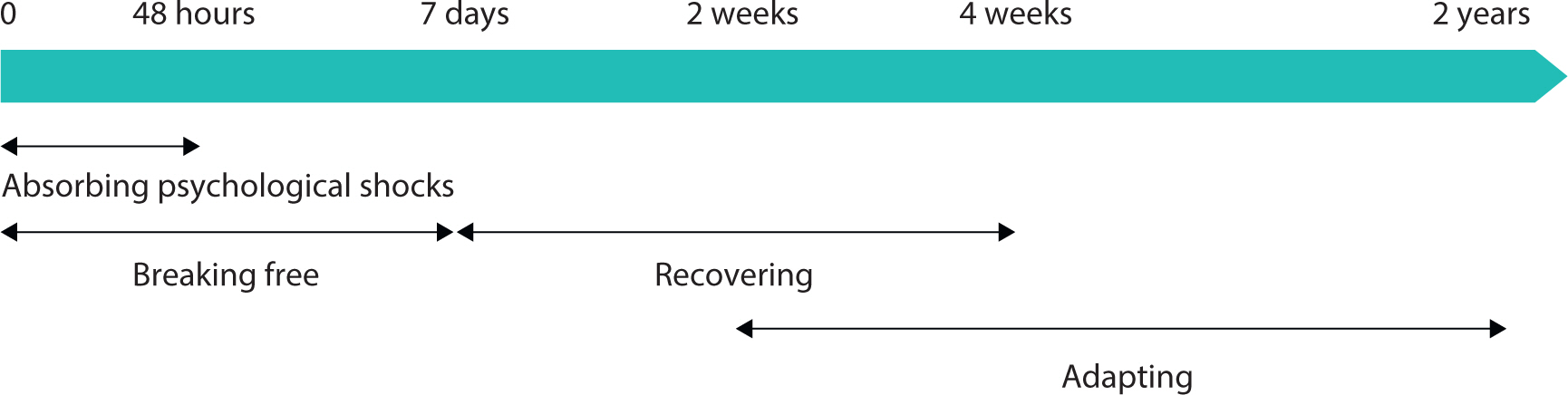
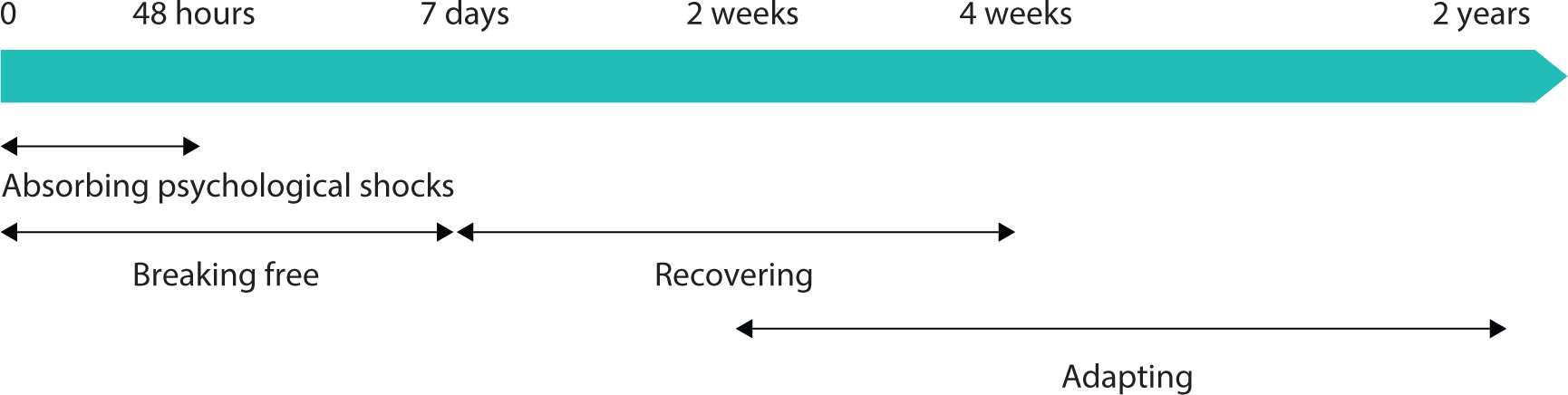
Psychological responses by post-accident phase
Psychological states—including physical, emotional, cognitive, and behavioral
aspects—evolve following an accident. Within 48 hours after the event,
individuals typically enter a period of shock, while within 7 days of the incident,
they begin to distance themselves from the immediate psychological impact. Recovery
rates vary from person to person. The period from 1 week to 1 month after the
accident is generally regarded as the recovery phase. This is followed by a period
of adaptation, which facilitates reintegration into daily life (Fig. 3). The following overview summarizes each phase in the
Occupational Trauma Management Program’s psychological response following an
accident.
Fig. 3.
Changes in psychological responses by phase after exposure to or
witnessing of an accident. Data from Korea Occupational Safety and Health
Agency [29].
Emergency response phase (within 7 days of the incident)
During this stage, intrusive symptoms are highly active. Survivors may experience
guilt, a sense of loss, anger, grief, irritability, dissociation, flashbacks,
nightmares, and insomnia, with these symptoms collectively peaking in severity
for up to a week. Symptoms observed between 3 days and 1 month after exposure
meet the criteria for acute stress reaction, with PTSD being diagnosed after 1
month. The primary goal is to stabilize the individual psychologically; however,
debriefing about the event can trigger re-experiencing, so caution is advised
[33,34]. If an individual exhibits extreme psychological and physical
reactions in the early stages, it is crucial to establish a safe environment
where they can access counseling services to achieve psychological
stabilization. Survivors should not be compelled to share personal thoughts or
emotions about the incident [35]. If
symptoms are not severe, clinicians should encourage the maintenance or swift
resumption of daily activities and recommend medication if necessary.
Additionally, they should endeavor to prevent isolation and to pay close
attention to any difficulties the worker reports.
As an example, the Eastern Gyeonggi Occupational Trauma Center has an emergency
response team—consisting of an occupational and environmental medicine
specialist, a counseling professional, and a musculoskeletal disorder prevention
specialist—in place for rapid crisis intervention. Depending on the needs
of the workplace and workers, nursing or occupational hygiene professionals may
also be added to the team (Table 3).
Table 3.
Crisis intervention programs offered by the Eastern Gyeonggi
Occupational Trauma Center
Focus area
Support personnel
Activities
Psychological education
Counseling specialist
- Education on physical, cognitive,
emotional, and behavioral trauma responses - Information
on recovery processes - Referral to trauma counseling
services
Physical stabilization training
Musculoskeletal disorder Prevention
specialist
- Muscle relaxation through physical
exercises - Promotion of body awareness and preventing
dissociation
Medical and psychological
assessment
Occupational and environmental
medicine Specialist
- Medical diagnosis of pre-existing
and physical conditions - Assessment of psychological
state
Counseling specialist
- Initial psychological evaluation for
stress and emotional responses
Psychological stabilization
Counseling specialist
- Counseling to prevent hyperarousal
and dissociation - Expansion of emotional safety and
promotion of psychological comfort - Individual or group
counseling
Administrative support
Office manager
- External cooperation and
scheduling - Support during mobile counseling
Work environment improvement
Occupational environment
specialist
- Consultation to ensure safety in the
accident area
Data from Eastern Gyeonggi Occupational Trauma Center.
The primary targets for emergency intervention are detailed in Table 4. In cases of physical injury,
psychological intervention can occur after appropriate medical treatment has
been administered. Individuals who initially discover or respond to accidents,
such as safety managers and health managers, may also be at high risk for PTSD
and are therefore prioritized for support [36].
Table 4.
Victims and priority groups for crisis intervention
Victim type
Description
Primary victims
Survivors experiencing physical
injuries or psychological trauma
Secondary victims
Witnesses or responders to fatalities
or injuries, accident response managers, team members of
victims, roommates, or others feeling responsible for the
incident
Program eligibility
Includes directly affected
individuals, first responders, safety managers, health officers,
colleagues with close personal ties to victims, and coworkers or
roommates
Data from Korea Occupational Safety and Health Agency [37].
Early response phase (8 days to 1 month after the incident)
During the early response phase, symptoms of post-traumatic stress may intensify,
including insomnia, major depression, alcohol dependence, and anxiety. The
primary objective of management is to prevent the development of PTSD, sleep
disorders, major depression, anxiety disorders, alcohol dependence, and suicidal
behavior. At this stage, clinicians typically administer screening assessments,
such as tests for post-traumatic stress reactions, physical responses, emotional
issues like depression or anxiety, and suicidal ideation. Formal counseling is
often initiated at this point. Any ongoing acute stress reactions must also be
monitored. Individuals with mild symptoms are encouraged to practice self-care
and resume their daily activities. However, if recovery is not observed after 1
month, or if severe insomnia, panic disorder, or an exacerbation of pre-existing
mental health conditions occur within this first month, the use of psychiatric
medication may be considered.
Mid-term response phase (1 to 3 months after the incident)
Starting at the 1-month mark, the objective is to reduce symptoms of PTSD and
prevent lasting effects. During this period, an individual may be formally
diagnosed with PTSD. While many people begin to show improvement or recovery,
those who do not should receive ongoing follow-up. Most individuals are capable
of resuming their daily activities, with the option of receiving further
counseling if necessary.
Long-term response phase (3+ months after the incident)
The long-term response is the stage of follow-up designed to alleviate any
residual effects of post-traumatic stress. At this point, most individuals can
fully resume normal activities, and the restoration of regular routines is
encouraged. However, in workplaces where multiple accidents have occurred,
gradual recovery may require flexible adjustments to the number of counseling
sessions.
From a managerial perspective, once an accident occurs, operations at the
workplace should be temporarily halted to prevent secondary incidents. Exposed
workers must be monitored for potential sleep, dietary, health, or psychological
issues, and transparent information should be provided to prevent
misunderstandings or mistrust regarding the incident. Workers who require it
should be granted time off or leave to support their psychological well-being.
Those affected should be separated from the accident site and public areas, and
if the demands of their job are high, they should be temporarily reassigned to
lighter duties to avoid overwork. If any individual experiences chest pain,
difficulty breathing, severe pain, extreme anxiety, or insomnia, management
should ensure they have access to appropriate medical care [37].
Crisis intervention methods and case examples
Before any crisis intervention takes place, it is essential to establish the
objectives and process of psychological intervention and adapt them to the specific
workplace environment. A private counseling area that fosters a sense of safety
should be designated, and efforts should be made to offer psychological services to
all exposed workers, ensuring clear advance communication to avoid
misunderstandings. Research has shown that employing multiple intervention methods
is more effective than relying on a single approach [38].
The Occupational Trauma Management Program involves a variety of crisis intervention
strategies. These include group-based psychological education aimed at immediate
stabilization, individual and group counseling, and follow-up services.
Psychological education
This training provides trauma education based on Psychological First Aid (PFA),
with core principles including the neurophysiological foundations of physical,
emotional, cognitive, and behavioral responses, as well as the processes of
arousal control, normalization, and validation. The safety of survivors should
be promoted and emphasized [39]. PFA is
widely endorsed by experts as a key early intervention for individuals affected
by disasters and is considered the standard for mental health and psychosocial
support in catastrophic or extreme conditions [40]. One advantage of psychological education is its capacity to
address many individuals simultaneously. Its objectives are to promote personal
awareness of acute reactions (such as anxiety or fear), increase psychological
stability, and prepare individuals for potential future psychological shifts.
When feasible, this education is offered during the emergency and early response
phases, although the timing can be adjusted as necessary (Table 5). Additionally, psychological education can help
support physical safety when integrated with activities like group stretching or
muscle relaxation exercises.
Table 5.
Processes and activities associated with psychological support for
witnesses to workplace fatalities at a manufacturing company
Processes
Activity
Collaboration request
- The local branch of the Ministry of
Employment and Labor or KOSHA sent a request to the Occupational
Trauma Center for collaboration on the case. - The
Occupational Trauma Center coordinated with the health and
safety manager of the company to select workers who required
psychological support.
Rapid intervention
- The Occupational Trauma Center
formed an emergency response team. - The emergency
response team administered a psychological and physical
stabilization program. - Psychological evaluations for
trauma, depression, and anxiety were conducted along with
individual counseling.
Worker recovery support
- Two to nine sessions of individual
psychological counseling were provided. - Follow-up
evaluations were completed at 1 month, 6 months, and 3 years
after the accident.
KOSHA, Korea Occupational Safety and Health Agency.
Data from Eastern Gyeonggi Trauma Counseling Center.
Individual counseling
Sessions are conducted on a one-on-one basis and typically last between 40 and 60
minutes. The details can be adjusted depending on the individual’s level
of exposure and the degree of trauma. If medical treatment or medication is
required, psychiatric referrals can be made. Initial sessions are generally
focused on stabilization; once individuals can self-regulate, they proceed to
processing memories and mourning, and ultimately to reintegration and resuming
their daily activities [41]. The degree
of early stabilization may be indicative of prognosis.
Group counseling
Approximately 10 workers experiencing similar levels of shock may participate in
a group. If an individual’s symptoms are severe, one-on-one counseling is
preferable. Group members can verbalize or use other media to express their
grief and shock, collectively engage in mourning processes, and contribute to
psychological healing. At the initiation of group counseling, rules should be
established to prevent secondary trauma, such as avoiding blame or
accusations.
Follow-up
Follow-up services begin when individuals have largely returned to normal
functioning and are approaching discharge from the program. These services aim
to prevent relapses and verify successful adaptation.
The following brief example from a crisis intervention for witnesses of a fatal
accident at a workplace in the eastern Gyeonggi region illustrates how
psychological support can facilitate post-accident intervention.
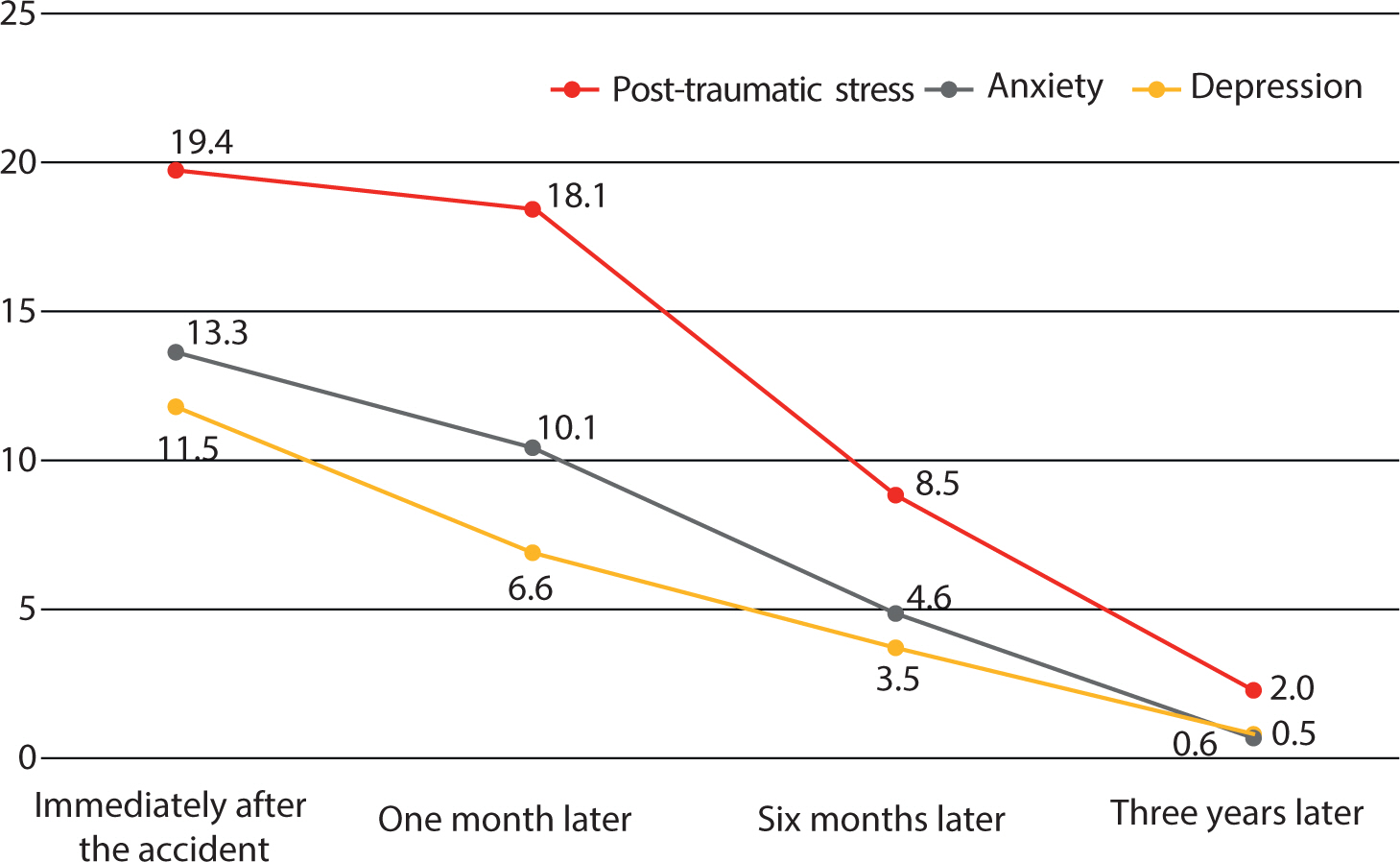
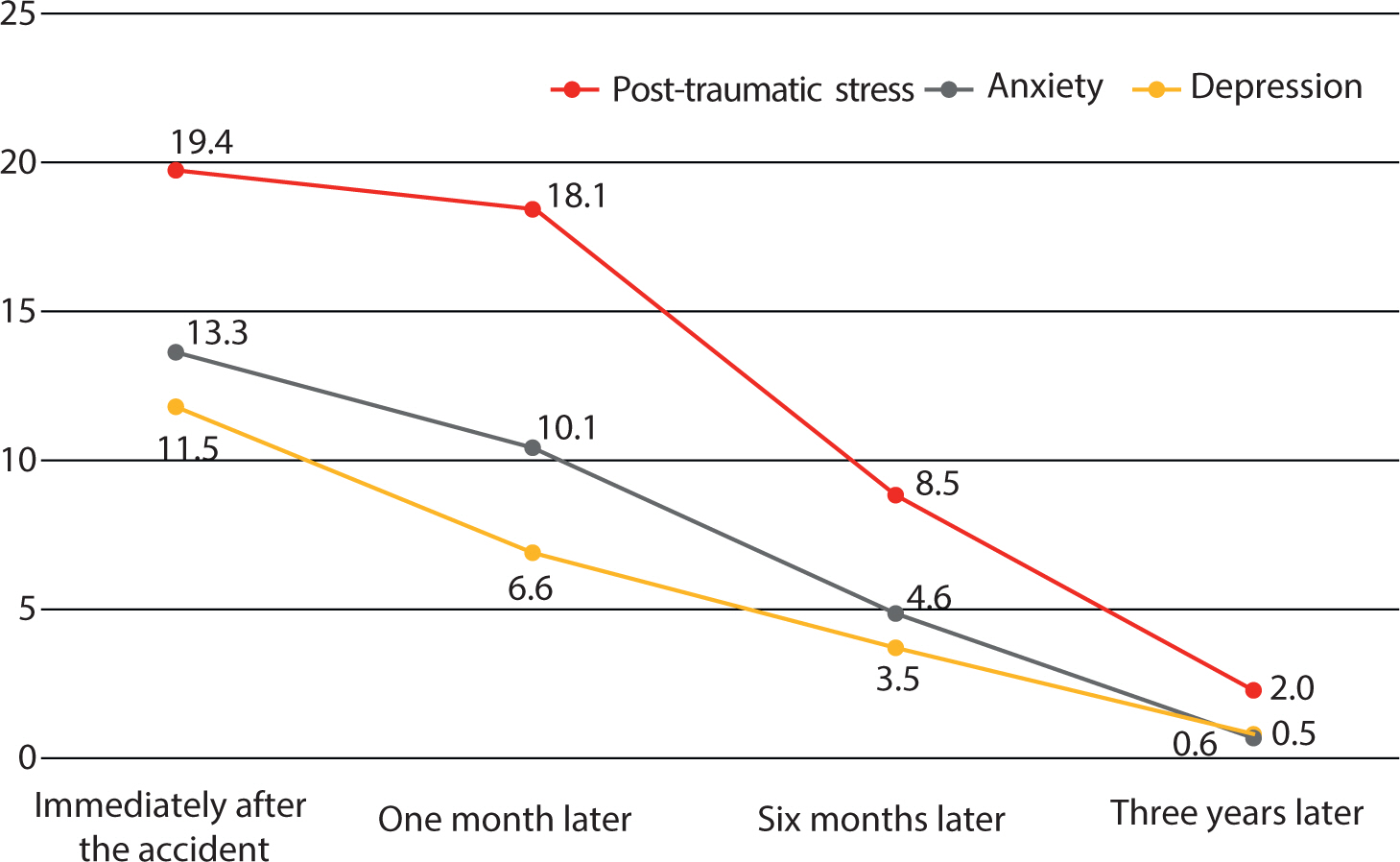
When the Occupational Trauma Management Program intervention was applied,
individual recovery times varied. Nonetheless, psychological assessments
conducted at 1 month, 6 months, and 3 years after the accident revealed
reductions in post-traumatic stress, depression, and anxiety to more stable
levels compared to initial measurements. These outcomes are illustrated in Fig. 4.
Fig. 4.
Changes in post-traumatic stress and emotional state among workers
receiving psychological support. Data from Kim et al. [24].
Role of the Occupational Trauma Center
Occupational Trauma Centers were established to prevent post-traumatic stress among
workers exposed to sudden workplace accidents and to support their return to normal
life and work. The Occupational Trauma Management Program plays a key role in
safeguarding the mental health of workers impacted by workplace injuries. As of
2024, a total of 23 Occupational Trauma Centers have been established within Worker
Health Centers across Korea, aligning with the jurisdictions of local branches of
the Ministry of Employment and Labor.
The key prerequisites for Occupational Trauma Centers to foster psychological safety
and ensure prompt stabilization for workers are as follows:
1) Timely intervention after workplace accidents: Early interventions,
including PFA and community-based trauma care, are vital for improving
outcomes for survivors [42]. When
investigating industrial accidents, local offices of the Ministry of
Employment and Labor should actively recommend the implementation of the
Occupational Trauma Management Program.
2) Regional accessibility: Korea now has 23 Occupational Trauma Centers
operating within Worker Health Centers, making psychological interventions
for industrial accidents in nearby jurisdictions more accessible than ever.
The availability of on-site services helps to alleviate the time and
financial burdens faced by businesses.
3) Follow-up for exposed workers: Monitoring is necessary to prevent
secondary trauma, track worker recovery, and evaluate the ongoing efficacy
of treatment.
Conclusion
In the context of workplace injury, it is imperative to raise awareness about the
need for collaboration among relevant agencies, workplaces, and individuals to
safeguard the mental health of victims and to ensure that the hidden suffering
associated with high rates of work-related fatalities is addressed. Employers must
recognize that preventing post-traumatic stress is key to helping workers resume
their duties and minimizing lost labor time.
Going forward, Occupational Trauma Centers must emphasize public accessibility,
professional expertise, and diverse empirical research to validate the effectiveness
of the program, as follows.
Public accessibility
Nationwide legislation is required to protect workers’ mental health
following workplace accidents. Such legislation would increase awareness of
mental health in the workplace, facilitate prompt access to psychological
services for affected individuals, and promote the consistent implementation of
Occupational Trauma Management Programs. Although improving accident
investigation systems to prevent recurrence is crucial, now is also the time for
active referral to and promotion of Occupational Trauma Centers to avoid
secondary psychological harm resulting from accidents.
Professional expertise
A training system for occupational trauma experts must be established.
Specialized counseling personnel—trained to address industrial disasters,
as these differ from other forms of disaster or personal trauma)—are
needed. It is essential to develop a structured educational system that
considers variations by timeframe, recovery phase, and risk level, and that
supports the acquisition of empirically verified techniques. Such a system is
crucial for the continuous improvement of professional standards in the field of
industrial accident trauma counseling.
Empirical research
To evaluate the Occupational Trauma Management Program, a variety of empirical
studies are necessary. More experts are encouraged to generate evidence-based
findings regarding the effectiveness of psychological interventions after
industrial accidents.
Large-scale workplace accidents continue to occur, and climate change has led to
an increase in significant catastrophes. Consequently, there is a growing need
for collaborative responses across multiple agencies. Extending beyond public
institutions, more robust networks of occupational health managers must be
fostered within workplaces. Such networks would ensure that community-based
systems can operate effectively to safeguard the mental health of workers
affected by workplace accidents.
Authors' contributions
Project administration: Kim CS, Kong JO, Koo JW
Conceptualization: Kim CS, Kong JO
Methodology & data curation: Kim CS, Kong JO
Funding acquisition: not applicable
Writing – Original draft: Kim CS
Writing – review & editing: Kim CS, Kong JO, Koo JW
Conflict of interest
No potential conflict of interest relevant to this article was reported.
3. Korea Law Information Center. Occupational safety and health act [Internet]. Sejong (KR): Ministry of Government Legislation; c2022 [cited 2023 Jan 14]. Available from https://www.law.go.kr/
4. Ministry of Government Legislation. National Law Information Center [Internet]. Sejong (KR): Ministry of Government Legislation; c2024 [cited 2024 Nov 10]. Available from http://www.moleg.go.kr
5. Kim M, Park S. The effect of corporate characteristics on occupational injuries:
comparison of SMEs and large enterprises. Ind Res 2023;47(2):139-169.
6. Ministry of Employment and Labor. Pilot operation of the occupational trauma counseling center in
Daegu. Sejong: Ministry of Employment and Labor; 2018.
7. Lim JM, Jang MS, Kim KW. A study on psychological trauma, safety climate, safety
accidents, and safety behavior among workers with industrial
experience. Korean J Health Psychol 2020;25(6):1077-1095.
8. Black DW, Grant JE. DSM-5 guidebook. 1st ed. Seoul: Hakjisa; 2018.
9. Boyer SM, Caplan JE, Edwards LK. Trauma-related dissociation and the dissociative disorders:
neglected symptoms with severe public health consequences. Dela J Public Health 2022;31(2):78-84.
10. Jang JM, Choi NH, Kang HS, Park SH. Levels of event impact, anxiety, and depression among workers
with industrial accidents. J Korean Acad Community Health Nurs 2009;20(2):234-242.
11. Woo JM, Kang TY, Lee JE. Increasing risk of mental health problems among subway drivers
experiencing accidents on the track. Korean J Occup Environ Med 2005;17(1):36-43.
12. Wiseman TA, Curtis K, Lam M, Foster K. Incidence of depression, anxiety and stress following traumatic
injury: a longitudinal study. Scand J Trauma Resusc Emerg Med 2015;23:29
13. Lee DY, Na J, Sim M. Psychological reactions and physical trauma by types of
disasters: view from man-made disaster. J Korean Neuropsychiatr Assoc 2015;54(3):261-268.
14. Kim CS, Kim JW, Lee SY, Cho SE, Cho YM, Koo JW, et al. A case study on posttraumatic stress responses among workers who
witnessed industrial accidents in a manufacturing workplace. In: Proceedings of the Korean Society of Occupational and Environmental
Medicine Conference; 2014 Nov 6-8; Gyeongju. Seoul (KR): The Korean Society of Occupational & Environmental
Medicine; 2014 p. p. 321-322.
15. Kim I, Lee D. The effects of intrusive and intentional rumination on
psychological distress and problem drinking in adults: mediating effects of
PTSD symptoms and emotion regulation difficulties. J Rehabil Psychol 2024;30(4):117-142.
16. Yoon MS, Lee HJ. Moderating role of social support on the relationship between
posttraumatic stress disorder (PTSD) and drinking behavior among
employees. Mental Health Soc Work 2014;42(4):115-142.
17. Kim JB, Lim JH. Effects of trauma level, initial symptom severity and problematic
alcohol on PTSD symptoms in victims of disaster: focusing on exposure to
natural disasters causing death and injury. Ment Health Soc Work 2023;51(2):29-52.
18. Kim SI, Yeon GY, Ha EH, Woo HW, Kim YC. Quality of life, suicide ideation, and depressive symptoms in
industrial injury patients. J Korean Neuropsychiatr Assoc 2001;40(3):416-424.
19. Sluys K, Häggmark T, Iselius L. Outcome and quality of life 5 years after major
trauma. J Trauma Acute Care Surg 2005;59(1):223-232.
20. Heo SJ. Effects of pain, sleep quality, rehabilitation motivation, depression,
and anxiety on quality of life in occupational accident patients. [M.S. thesis]. Gongju: Kongju National University; 2021.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington: American Psychiatric Association; 2013
22. National Institute for Occupational Safety and Health
(NIOSH). National Institute for Occupational Safety and Health
[Internet] Washington (DC), NIOSH. c2024;[cited 2024 Nov 10]. Available from https://www.cdc.gov/niosh/index.html
23. Ben-Zion Z, Artzi M, Niry D, Keynan NJ, Zeevi Y, Admon R, et al. Neuroanatomical risk factors for posttraumatic stress disorder in
recent trauma survivors. Biol Psychiatry Cogn Neurosci Neuroimaging 2020;5(3):311-319.
24. Kim CS, Kong JO, Jeong HJ, Koo JW. A case of trauma management for co-workers after a workplace
fatality. In: Proceedings of the Korean Society of Occupational and Environmental
Medicine Conference; 2022 Nov 11; Jeju. Seoul (KR): The Korean Society of Occupational & Environmental
Medicine; 2022.
25. Baek SU, Lee WT, Kim MS, Lim MH, Yoon JH, Won JU. Self-esteem trajectories after occupational injuries and diseases
and their relation to changes in subjective health: result from the panel
study of workers’ compensation insurance (PSWCI). J Korean Med Sci 2023;38(37):e284.
26. Hong CM. Work performance among workers without disabilities after
industrial accidents: a longitudinal study. Open Pub Health J 2024;17:e18749445296395.
27. Shin J, Park K, Lee Y, Choi S, Jang Y, You M. The protective effect of perceived social support on
psychological health during the COVID-19 pandemic: the case of Gyeonggi
province in South Korea. Korean Soc Health Educ Promot 2023;40(2):1-14.
28. Ministry of the Interior and Safety. Korea workers’ compensation & welfare service work-related
injury disease mental disorders [Internet] Sejong (KR), Ministry of the Interior and Safety. c2022;[cited 2024 Nov 10]. Available from https://www.data.go.kr/data/15113358/fileData.do#tab-layer-file
29. Korea Occupational Safety and Health Agency. Occupational trauma management program operating manual. Ulsan: Korea Occupational Safety and Health Agency; 2020.
30. Lee MS, Kim EY. Current status and challenges of industrial accident trauma
support in Korea: a case study of the occupational trauma center in region
D. Korean J Counsel Psychotherapy 2023;35(4):1517-1541.
31. Korea Occupational Safety & Health Agency. Notice [Internet]. Ulsan (KR): Korea Occupational Safety & Health
Agency; c2025 [cited 2024 Nov 10]. Available from https://kosha.or.kr/kosha/report/notice.do
33. Mayou RA, Ehlers A, Hobbs M. Psychological debriefing for road traffic accident victims:
three-year follow-up of a randomised controlled trial. Br J Psychiatry 2000;176(6):589-593.
34. van Emmerik AAP, Kamphuis JH, Hulsbosch AM, Emmelkamp PMG. Single session debriefing after psychological trauma: a
meta-analysis. Lancet 2002;360(9335):766-771.
37. Korea Occupational Safety and Health Agency. Occupational trauma management program operating manual. Ulsan: Korea Occupational Safety and Health Agency; 2021.
38. Roberts NP, Kitchiner NJ, Kenardy J, Robertson L, Lewis C, Bisson JI. Multiple session early psychological interventions for the
prevention of post‐traumatic stress disorder. Cochrane Database Syst Rev 2019;8(3):CD006869
The age of trauma: the prevalence and psychological impact of potentially traumatic exposures in South Korea Gaeun Son, Jihee Jang, Euntaek Hong, Subin Park, Yun-Kyeung Choi, Kee-Hong Choi Frontiers in Psychiatry.2025;[Epub] CrossRef
Trauma counseling centers for psychological support to manage trauma
from workplace injuries in Korea: a narrative review
Fig. 1.
Number and rate of fatalities due to industrial accidents. Data from
Ministry of Employment and Labor [1].
Fig. 2.
Operational framework of the occupational trauma management program. Data
from Korea Occupational Safety and Health Agency [28].
Fig. 3.
Changes in psychological responses by phase after exposure to or
witnessing of an accident. Data from Korea Occupational Safety and Health
Agency [29].
Fig. 4.
Changes in post-traumatic stress and emotional state among workers
receiving psychological support. Data from Kim et al. [24].
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Trauma counseling centers for psychological support to manage trauma
from workplace injuries in Korea: a narrative review
Mental health disorders associated with occupational injuries
(2011–2022)
Category
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
Applications
102
127
137
137
165
183
213
268
331
581
720
678
Approvals
26
47
53
47
63
85
126
201
231
396
515
445
Approval rate (%)
25.5
37
38.7
34.3
38.2
46.4
59.2
75
69.8
68.2
71.5
65.6
Depression
14
15
14
17
17
14
52
72
66
113
113
80
Adjustment disorder
2
11
5
11
13
21
32
53
78
162
248
227
Acute stress disorder
4
7
14
3
9
5
8
15
15
23
10
26
Post-traumatic stress disorder
2
7
9
9
14
25
21
36
39
55
83
63
Anxiety disorder
2
1
2
3
2
4
1
5
13
19
21
23
Others
2
6
9
4
8
16
12
20
20
24
40
26
Data from Korea Workers’ Compensation & Welfare Service
[28].
Operational status of Occupational Trauma Centers in Korea by
year
Year
Number of centers opened
Centers
2018–2019
1
Pilot center with national jurisdiction
(Daegu Occupational Trauma Center)
2020
8
Eastern Gyeonggi, Western Gyeonggi,
Gyeongnam, Gwangju, Bucheon, Daegu, Daejeon, Incheon
Data from Korea Occupational Safety and Health Agency [31].
Crisis intervention programs offered by the Eastern Gyeonggi
Occupational Trauma Center
Focus area
Support personnel
Activities
Psychological education
Counseling specialist
- Education on physical, cognitive,
emotional, and behavioral trauma responses - Information
on recovery processes - Referral to trauma counseling
services
Physical stabilization training
Musculoskeletal disorder Prevention
specialist
- Muscle relaxation through physical
exercises - Promotion of body awareness and preventing
dissociation
Medical and psychological
assessment
Occupational and environmental
medicine Specialist
- Medical diagnosis of pre-existing
and physical conditions - Assessment of psychological
state
Counseling specialist
- Initial psychological evaluation for
stress and emotional responses
Psychological stabilization
Counseling specialist
- Counseling to prevent hyperarousal
and dissociation - Expansion of emotional safety and
promotion of psychological comfort - Individual or group
counseling
Administrative support
Office manager
- External cooperation and
scheduling - Support during mobile counseling
Work environment improvement
Occupational environment
specialist
- Consultation to ensure safety in the
accident area
Data from Eastern Gyeonggi Occupational Trauma Center.
Victims and priority groups for crisis intervention
Victim type
Description
Primary victims
Survivors experiencing physical
injuries or psychological trauma
Secondary victims
Witnesses or responders to fatalities
or injuries, accident response managers, team members of
victims, roommates, or others feeling responsible for the
incident
Program eligibility
Includes directly affected
individuals, first responders, safety managers, health officers,
colleagues with close personal ties to victims, and coworkers or
roommates
Data from Korea Occupational Safety and Health Agency [37].
Processes and activities associated with psychological support for
witnesses to workplace fatalities at a manufacturing company
Processes
Activity
Collaboration request
- The local branch of the Ministry of
Employment and Labor or KOSHA sent a request to the Occupational
Trauma Center for collaboration on the case. - The
Occupational Trauma Center coordinated with the health and
safety manager of the company to select workers who required
psychological support.
Rapid intervention
- The Occupational Trauma Center
formed an emergency response team. - The emergency
response team administered a psychological and physical
stabilization program. - Psychological evaluations for
trauma, depression, and anxiety were conducted along with
individual counseling.
Worker recovery support
- Two to nine sessions of individual
psychological counseling were provided. - Follow-up
evaluations were completed at 1 month, 6 months, and 3 years
after the accident.
KOSHA, Korea Occupational Safety and Health Agency.
Data from Eastern Gyeonggi Trauma Counseling Center.
Table 1.
Mental health disorders associated with occupational injuries
(2011–2022)
Data from Korea Workers’ Compensation & Welfare Service
[28].
Table 2.
Operational status of Occupational Trauma Centers in Korea by
year
Data from Korea Occupational Safety and Health Agency [31].
Table 3.
Crisis intervention programs offered by the Eastern Gyeonggi
Occupational Trauma Center
Data from Eastern Gyeonggi Occupational Trauma Center.
Table 4.
Victims and priority groups for crisis intervention
Data from Korea Occupational Safety and Health Agency [37].
Table 5.
Processes and activities associated with psychological support for
witnesses to workplace fatalities at a manufacturing company
KOSHA, Korea Occupational Safety and Health Agency.
Data from Eastern Gyeonggi Trauma Counseling Center.