Review Special topic: role of institutes related to the occupational and environmental diseases in Korea
Challenges from 14 years of experience at Workers' Health
Centers in basic occupational health services for micro and small enterprises in
Korea: a narrative review
1Workers' Health Center in East Gyeonggi, Seongnam, Korea
2Department of Environmental Medicine, Ewha Womans University College of Medicine, Seoul, Korea
3With Health Welfare Social Cooperative, Daegu, Korea
*Corresponding author: Kyunghee
Jung-Choi, Department of Environmental Medicine, Ewha Womans University College
of Medicine, 25, Magokdong-ro 2-gil, Gangseo-gu, Seoul 07804, Korea, E-mail:
jungchoi@ewha.ac.kr
• Received: November 26, 2024 • Revised: January 8, 2025 • Accepted: January 8, 2025
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Health and safety issues in micro and small enterprises (MSEs) are recognized as
a global challenge. This study aimed to examine Workers' Health Centers
(WHCs) as a representative public organization providing occupational health
services to MSEs in Korea. WHCs were established in 2011 after a trial period
aimed at addressing occupational diseases in MSEs with limited resources. As of
2024, there are 24 WHCs, 22 branch offices, and 23 trauma counseling centers for
workers. These health centers are managed by the Korea Occupational Safety and
Health Agency, with their actual operation delegated to private organizations.
Each WHC employs an average of 13 staff members and is organized into four
specialized teams: cardiovascular disease prevention, workplace environment
improvement, musculoskeletal disease prevention, and occupational stress
management. These centers also offer common basic programs along with
region-specific specialized initiatives. In 2023, the total cumulative number of
users reached 203,877, with employees from MSEs comprising approximately 88.5%
of the total. WHCs can thus be seen as playing a pivotal role as case managers
of health requirements in the workplace by fostering strong relationships with
MSEs and linking them to other relevant programs through a
problem-solving-oriented approach. Given the limited resources of these
enterprises, proactive policies and the equitable application of safety and
health regulations are essential. A balanced strategy that combines regulatory
enforcement with practical assistance is critical to ensure the success of WHCs
in improving health and safety conditions in MSEs.
Health and safety issues in micro and small enterprises (MSEs), which account for
70 percent of total employment worldwide [1], are recognized as a significant global challenge [2–4]. According to Organization for Economic Co-operation and
Development (OECD) criteria, microenterprises are businesses with fewer than 10
employees, while small enterprises have between 10 and 49 employees. Thus, MSEs
are workplaces with fewer than 50 employees. To sustain themselves, MSEs
typically adopt a low-road strategy, relying on low wages and price
competitiveness. They occupy a less powerful position in the global value chain
compared to medium and large businesses and often bear the risks and costs
transferred from their larger counterparts. With increasing pressures on working
conditions, such as unstable contracts, low wages, and unpaid overtime [5], the workforce becomes increasingly
vulnerable to occupational safety and health (OSH) risks. Additionally, as
organizational interdependence becomes more complex and employment relationships
fracture, the gap between employment contracts, employment regulations, and
management controls widens. Therefore, MSEs lack the resources necessary for OSH
prevention and appropriate management, leaving their employees exposed to
significant risks to their well-being, along with poor working conditions and
low-quality work.
In OECD countries, the rates of fatal occupational injuries in 2020 ranged from
less than one to over five per 100,000 workers [6]. In the same year, Korea reported a rate of 4.65 fatal
occupational injuries per 100,000 workers. Although this rate is decreasing, it
remains significantly high. Similar to MSEs in other countries [7], those in Korea experience a higher
incidence of occupational injuries and diseases compared to medium and large
enterprises [8]. A 2022 report on
industrial accidents revealed that the overall company accident rate was 0.65,
while workplaces with fewer than five employees had a rate of 1.12 [9]. In contrast, enterprises with 50 or more
employees all reported rates below the average. In MSEs, musculoskeletal
disorders (MSDs), such as back pain, constitute almost 55% of occupational
diseases, making them the most prevalent [9–11]. These are
followed by hearing loss, pneumoconiosis, and cardiovascular disease (CVD).
Additionally, new types of occupational diseases are emerging, including MSD,
CVD, and psychological issues, which differ from the traditional chemical or
metal poisoning still present in Korea, as shown by the industrial accident
compensation insurance data [9]. However,
it is important to note that the industrial accident compensation insurance data
does not cover all individuals affected by industrial accidents, especially
those with occupational diseases. Coverage is limited to those who have applied
for and been granted compensation.
Efforts to prevent occupational diseases in MSEs in Korea have led to the
development of three main support programs focused on occupational health: the
Clean Workplace Project, financial support for work environment assessments or
special medical examinations, and private contractor programs for health and
Workers’ Health Centers (WHCs) [12,13]. These initiatives
collectively target nearly 2 million MSEs, accounting for 98% of the total, and
approximately 11 million workers [14].
The Clean Workplace Project offers up to $23,000 in financial assistance to
manufacturing companies with fewer than 50 employees to enhance their OSH
facilities. Additionally, financial support is provided for work environment
assessments and special medical examinations specifically for MSEs. Private
contractor programs for health and WHCs deliver direct occupational health
services. The private contractor program for health, which operates solely in
the workplace, focuses on managing chronic diseases and workplace hygiene
through the services of a nurse or occupational hygienist [8]. In contrast, WHCs are situated in industrial complexes
and staffed by a range of specialists including experts in occupational and
environmental medicine, nurses, exercise specialists, occupational hygienists,
and psychological counselors [15]. These
centers offer services both onsite and at the workplace.
Objectives
Although the Korean WHC has been operational for over a decade, there is a
notable scarcity of literature that systematically organizes the current status
and discussions surrounding these institutions. In light of this gap, this study
explores the WHC as a key public organization providing occupational health
services to MSEs in Korea.
Ethics statement
It is a literature database-based review; therefore, neither approval by the
institutional review board nor obtainment of informed consent was required.
Methods
To explore the status and discussions regarding WHCs in Korea, we first used domestic
and international search tools to locate WHC-focused papers and reports authored by
Korean researchers. For Korean-language papers, we searched using the keywords
근로자건강센터 (“workers’ health center”) and 직업트라우마센터 (“trauma
counseling center for workers”) in Google Scholar, the DataBase Periodical
Information Academic (DBPIA), the Research Information Sharing Service (RISS), the
Korean Studies Information Service System (KISS), and the National Assembly Library.
To identify English-language papers, we used the search terms
“workers’ health center and Korea” and “trauma
counseling center for workers and Korea” in Google Scholar and PubMed. We
also reviewed references cited in the initially identified documents, as well as
official WHC operations reports published by the Korea Occupational Safety and
Health Agency (KOSHA). The content of the selected papers and reports was analyzed
and categorized into data on the background, development, and performance of WHCs.
Papers and reports unrelated to WHCs were excluded from the analysis.
Results
Background of Workers’ Health Centers
The Participatory Government, which was established in February 2003, formed the
Presidential Advisory Committee on Aging and Future Society in March 2004. This
committee was tasked with developing a national strategy to address the
challenges of a low birth rate and an aging population [16]. In September 2004, the committee released the
Healthcare System Reform Plans for Ensuring Public Health in an Aging and Future
Society [17]. Included in this report was
a proposal to create an industrial health management system through
collaboration with the Ministry of Health and Welfare and the Ministry of Labor.
To support this initiative, these ministries launched a joint project aimed at
establishing an industrial health center, which would offer industrial health
services funded by the National Health Promotion Fund [18].
In September 2006, the establishment review committee selected the Banwol-Sihwa
area, a national industrial complex with a high concentration of MSEs, as the
site for the new industrial health center. The Banwol-Sihwa Regional Center for
Occupational Health opened in March 2007 [19]. From 2007 to 2009, the center was operated by KOSHA and its
staff. In 2010, while KOSHA continued to oversee the center's management
and provide administrative support, service provision was handled by medical
staff, nurses, and industrial hygienists employed by a privately entrusted
organization. By 2011, funding for the Banwol-Sihwa Regional Center for
Occupational Health was not included in the National Health Promotion
Fund's budget, leading to its closure after four years of operation
[18].
The Ministry of Employment and Labor facilitated the establishment of a WHC to
provide primary care to MSEs, funded by the Industrial Accident Compensation
Insurance and Prevention Fund. The entire process, from business planning to
operation, was delegated to private operating agencies. The inaugural WHC, the
Gyeonggi Western WHC, was set up in the Banwol-Sihwa Industrial Complex area,
leveraging the existing infrastructure of the Banwol-Sihwa Regional Center for
Occupational Health [20]. Subsequently,
the Incheon WHC and Gwangju WHC were introduced in 2011 through a public
offering [18,21].
Development of Workers’ Health Centers
Purpose, legal basis, and funding sources of Workers’ Health
Centers
The purpose of the WHCs has evolved slightly in line with the operational
directives of KOSHA. Initially, when WHCs were introduced in 2012, their
primary function was to enhance the prevention of occupational diseases and
to support the health maintenance and promotion of workers by offering basic
public occupational health services. These services included counseling on
preventing occupational diseases, specifically targeting workers in MSEs,
which are known for their relatively weak health management systems [22]. By 2016, KOSHA had redefined the
purpose of WHCs, positioning them to fulfill the responsibilities of a
health officer in MSEs that are not mandated to appoint one [21]. A health officer is tasked with
supporting the business owner or the person responsible for safety and
health management, especially concerning technical issues, as stipulated by
the Occupational Safety and Health Act. This shift marked a transition from
a broad and progressive goal of providing basic occupational health services
to a more focused objective aligned with the specific duties of a health
officer within the Korean occupational health framework. Following the 2018
report on WHC operations, the centers' foundational purpose was no
longer explicitly described [23,24]. The focus shifted from defining
their “purpose” to specifying their “role,”
which now includes acting as health officers for MSEs and serving as health
guardians for vulnerable enterprises.
The legal basis for the WHCs was established in 2013 when the Occupational
Safety and Health Act was revised to include a provision allowing the
Minister of Employment and Labor to establish and operate "facilities
for maintaining and promoting workers' health" [25]. This revision was further detailed
in Notification No. 2013-6 from the Ministry of Employment and Labor, which
defined WHCs and outlined the services they offer [26]. In 2019, amendments to the Occupational Safety and
Health Act broadened the range of facility users from
"workers" to "persons providing labor" [27]. Subsequently, in 2020, specific
guidelines for the establishment and operation of WHCs were integrated into
Notification No. 2020-19 issued by the Ministry of Employment and Labor
[28].
WHCs are funded through the Industrial Accident Compensation Insurance and
Prevention Fund, with budgets that vary based on the size of each center. In
2023, the operating budget for each center ranged from 564 to 968 million
won (approximately $400,000–$670,000, using 2024 exchange rates)
[24]. When examining the growth
of WHCs in terms of personnel and budget, the number of employees increased
by 1.9 times, from 172 in 2016 to 332 in 2023. However, the budget for WHCs
only grew by 1.7 times, from KRW 10.33 billion to KRW 17.774 billion over
the same period [21,24].
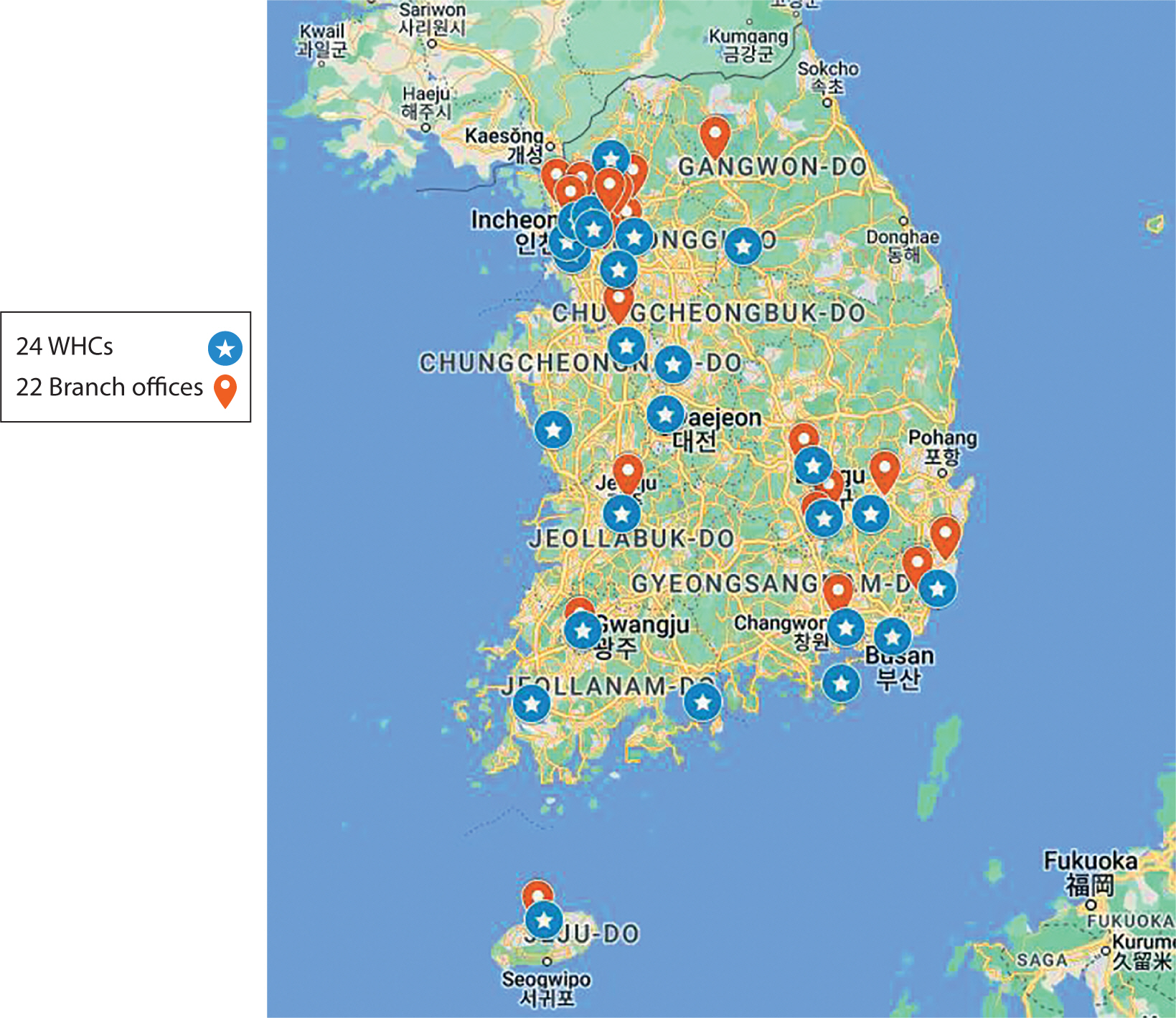
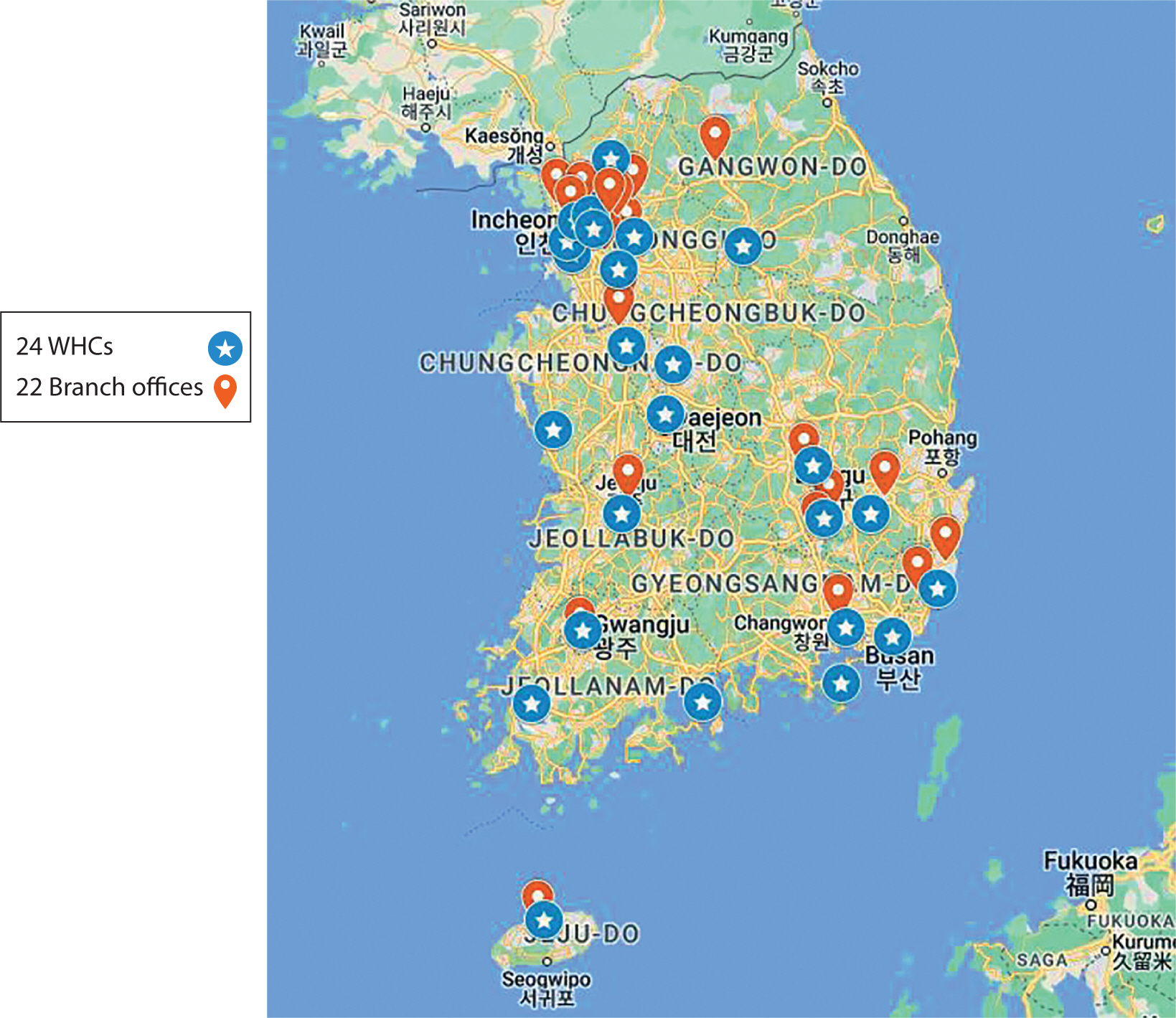
Nationwide distribution and facilities
As of 2024, there are 24 WHCs, 22 branch offices, and 23 trauma counseling
centers for workers (Table 1, Fig. 1). The expansion of WHCs began in
the early 2010s, with three centers established in 2011, two in 2012, and
five annually from 2013 to 2015. Since then, the growth rate has decreased,
with one WHC established in 2016, two in 2020, and one in 2024. Starting in
2016, five new branch offices were established to serve workers in
industrial complexes located beyond the reach of existing WHCs [21]. The years 2017 and 2023 saw the
addition of 16 and one branch office, respectively. To address trauma among
workers who have experienced significant industrial accidents, a pilot
trauma counseling center for workers was launched in 2018 and 2019. This
initiative led to the official establishment of eight institutions in 2020
[29]. The network expanded with
five additional centers in 2021, one in 2023, and nine in 2024, totaling 23
operational trauma counseling centers for workers.
Table 1.
Workers’ health centers, branch offices, and trauma
counseling centers for workers by region and operating agencies in
Korea
Region
Workers’ Health Center
(WHC)
Branch office (BO)
Trauma counseling center for
workers
Operating agency
Seoul
Seoul WHC
Seoul Jung-gu BO
○
Ewha University-Industry
Collaboration Foundation
Seoul Western WHC
Seoul Seongdong BO
○
Seoul National University Research
and Development Business Foundation
Busan
Busan WHC
Yangsan BO
○
Busan University Research and
Business Development Foundation
Daegu
Daegu WHC
Seodaegu BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Daegu Dalseong BO
Incheon
Incheon WHC
Incheon Bupyeong BO
○
Yonsei University
University-Industry Foundation
Gwangju
Gwangju WHC
Gwangju Gwangsan BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Daejeon
Daejeon WHC
-
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Ulsan
Ulsan WHC
Ulsan Buk-gu BO
○
Dong-a
University Industry-Academy Cooperation
Foundation
Gyeonggi-do
Gyeonggi Western WHC
Gunpo BO
○
Korea University Research and
Business Foundation
Gyeonggi Eastern WHC
Seongnam BO
○
The Catholic University of Korea,
Industry-Academic Cooperation Foundation.
Bucheon WHC
Gimpo Yangchon BO
○
The Catholic University of Korea,
Industry-Academic Cooperation Foundation
Gimpo Gochon BO
Gyeonggi Southern WHC
Pyeongtaek BO
○
Korea Workers’ Compensation
& Welfare Service Ansan Hospital
Gyeonggi Northern WHC
Namyangju BO
○
Gachon University
Industry-Academic Cooperation Foundation
Gangwon special self-governing
province
Gangwon WHC
Chuncheon BO
○
Yonsei University Wonju Severance
Christian Hospital
Chungcheongbuk-do
Chungbuk WHC
-
○
Korea Industrial Health
Association
Chungcheongnam-do
Chungnam WHC
Asan BO
○
Dankook University
Industry-Academia Cooperation Foundation
Chungnam Western WHC
-
-
Mirae Hygiene Environment
Institute Co., Ltd.
Jeonbuk special self-governing
province
Jeonbuk WHC
Wanju BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Jeollanam-do
Jeonnam Eastern WHC
-
○
Won-jin Foundation for
occupational diseases Green Hospital
Jeonnam Western WHC
-
-
Mokpo National University
Industry-Academic Cooperation Foundation
Gyeongsangbuk-do
Gyeongbuk Northern WHC
Gumi BO
○
Gumi Ganddong Hospital
Gyeongsan WHC
Yeongcheon BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Gyeongsangnam-do
Gyeongnam WHC
Changwon BO
○
Teo Occupational and Environmental
Medicine Center
-
Geoje BO
○
Daewoo Medical Foundation
Jeju special self-governing
province
Jeju WHC
Jeju Yeon-dong BO
○
Cheju Halla General Hospital
Fig. 1.
Distribution of Workers' Health Centers (WHCs) in
Korea.
WHC facilities cover an area of 400 to 500 square meters, while branch
offices range from 80 to 100 square meters [24]. Each center includes a front desk, separate counseling
rooms for MSD and CVD prevention, an education room, an exercise room, a
psychological counseling room, and a doctor’s counseling room. Since
WHCs are not medical facilities, they are not equipped to perform diagnostic
procedures such as blood draws or X-ray examinations. However, they do have
basic testing devices for consultations, exercise equipment, and protective
gear for use in the workplace. Since 2018, the WHCs have been maintaining
user consultation records through a web-based computer system. This system
functions as an integrated platform for both WHCs and branch offices, with
data centrally managed by KOSHA [30].
Management and operational staff
The managing agency, KOSHA, oversees the operational status of WHCs and
manages the Central Operation Committee. The actual operation of WHCs is
delegated to private organizations, with annual contract renewals between
KOSHA and these consignment agencies, ensuring a guaranteed operation period
of three years [31]. KOSHA contracts
with private agencies that fulfill specific qualification requirements.
These agencies are categorized into four types: university-industry
collaboration foundations, health-related associations, general hospitals,
and hospitals of the Korea Workers’ Compensation and Welfare Service
[31].
As of December 2023, the total number of employees at WHCs and their branch
offices was 302. This count does not include the staff at trauma counseling
centers for workers or the Geoje WHC, which operates under a unique staffing
structure. This brings the average staffing level to approximately 13
employees per center [24]. Each
center is structured into four specialized teams: the CVD Prevention Team,
which includes nurses; the Workplace Environment Improvement Team, made up
of industrial hygienists; the MSD Prevention Team, staffed by physical
therapists or exercise specialists; and the Occupational Stress Management
Team, which comprises counseling psychologists. Additionally, each center
employs physicians who provide comprehensive counseling. Centers that have a
branch office are staffed with one nurse and one additional specialist. In
contrast, each trauma counseling center for workers is staffed by two
psychology counselors.
Among the operational personnel of WHCs, irregular workers constitute nearly
70%. Their contracts are renewed annually, leading to significant job
insecurity [31,32]. In 2021, the turnover rate at WHCs was 15.8%,
approximately three times higher than the overall industry average of 4.8%
[31]. A 2021 survey revealed that
WHC employees are dissatisfied with job security and wage fairness, yet they
express considerable satisfaction with their work and job achievements. The
most challenging aspects of their work include unilateral work directives
from KOSHA, additional tasks stemming from government policies, rude
customer behavior, and unfair treatment by contracting agencies, listed in
order of difficulty [31].
Key programs and activities
The programs of a WHC are categorized into basic and regional specialization
initiatives. Basic programs, implemented by all centers nationwide,
encompass post-examination health counseling following general and special
health examinations, work environment consulting, health counseling for CVD
or MSD prevention, job stress management, education on occupational disease
prevention, and monitoring of occupational disease occurrence. Regional
specialization initiatives, on the other hand, are tailored to the specific
needs of the region in which each center operates. For instance, the Seoul
WHC offers an occupational disease prevention program tailored for workers
in the printing industry, a health management program for mobile workers
such as designated drivers and delivery personnel, and a health management
program for care workers [24]. All
programs are available both at the center and in the workplace, and can be
provided either individually or in groups.
WHCs prioritize networking with a variety of community stakeholders. They
share information and experiences, and coordinate activities with regional
employment and labor offices of the Ministry of Employment and Labor,
regional offices of KOSHA, labor unions, regional organizations,
occupational health institutes, and university hospitals, among others.
Public relations play a crucial role in promoting and recognizing WHCs. They
publicize their activities through websites, social networking sites,
leaflets, articles, videos, and TV or radio broadcasts.
Performance of Workers’ Health Centers
Key performance indicators
All WHCs are evaluated annually based on performance indicators that
encompass quantitative, qualitative, operational, user satisfaction, and
bonus categories, as of 2023 [24].
The quantitative evaluation relies on metrics such as improvements in health
levels, stabilization rates of occupational trauma, and post-examination
health counseling for essential and special employment workers. The
qualitative assessment evaluates the appropriateness of regional
specialization programs, conducted by a panel of approximately five internal
and external experts from KOSHA. The operational evaluation includes on-site
inspections by KOSHA officials, who review compliance with operational
plans, staffing and operations, the appropriateness of program
implementation and budget execution, and personal data protection. The
satisfaction survey is conducted by an external company hired by KOSHA,
which performs a sample survey of users. Bonus points are awarded for the
identification of potential occupational diseases or for winning awards at
the Workers’ Health Center Excellence Case Competition [24].
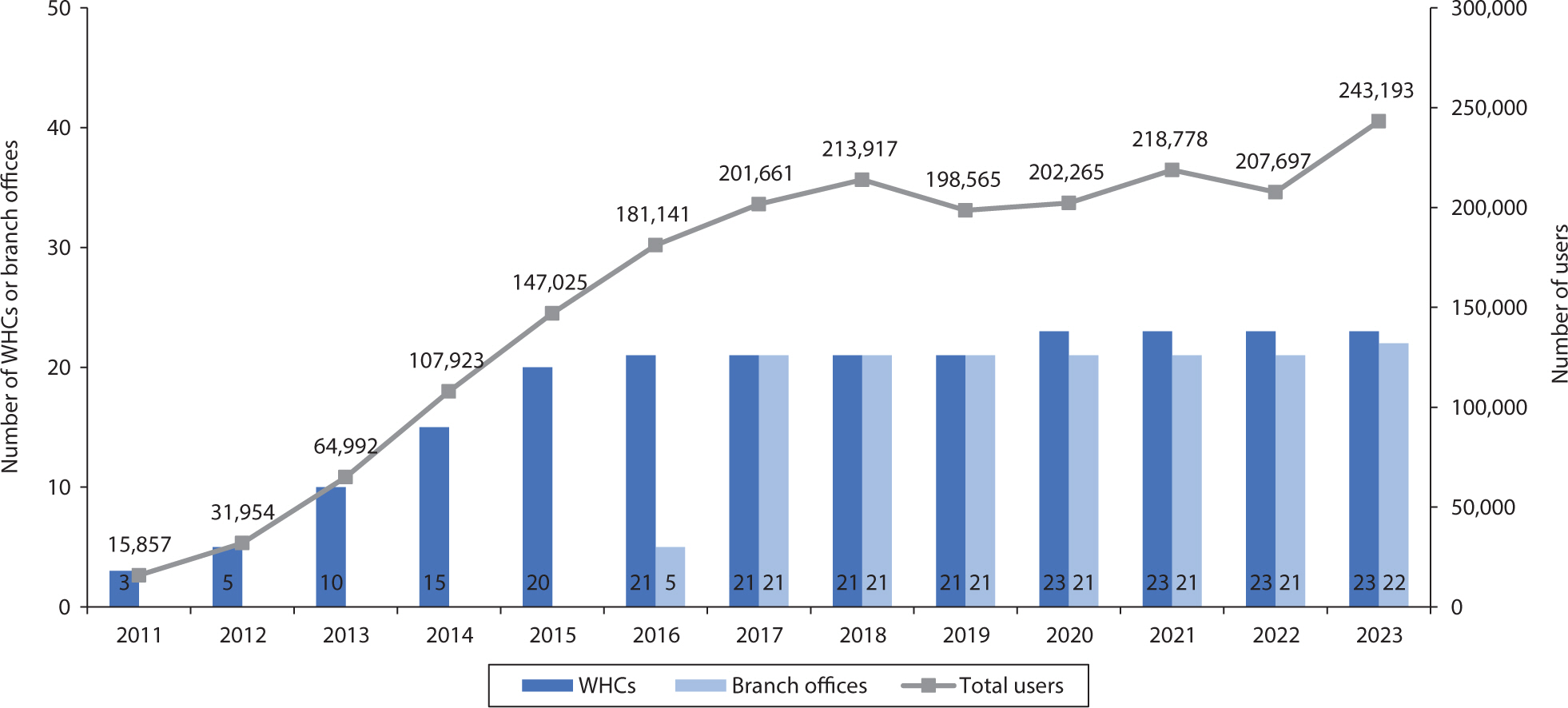
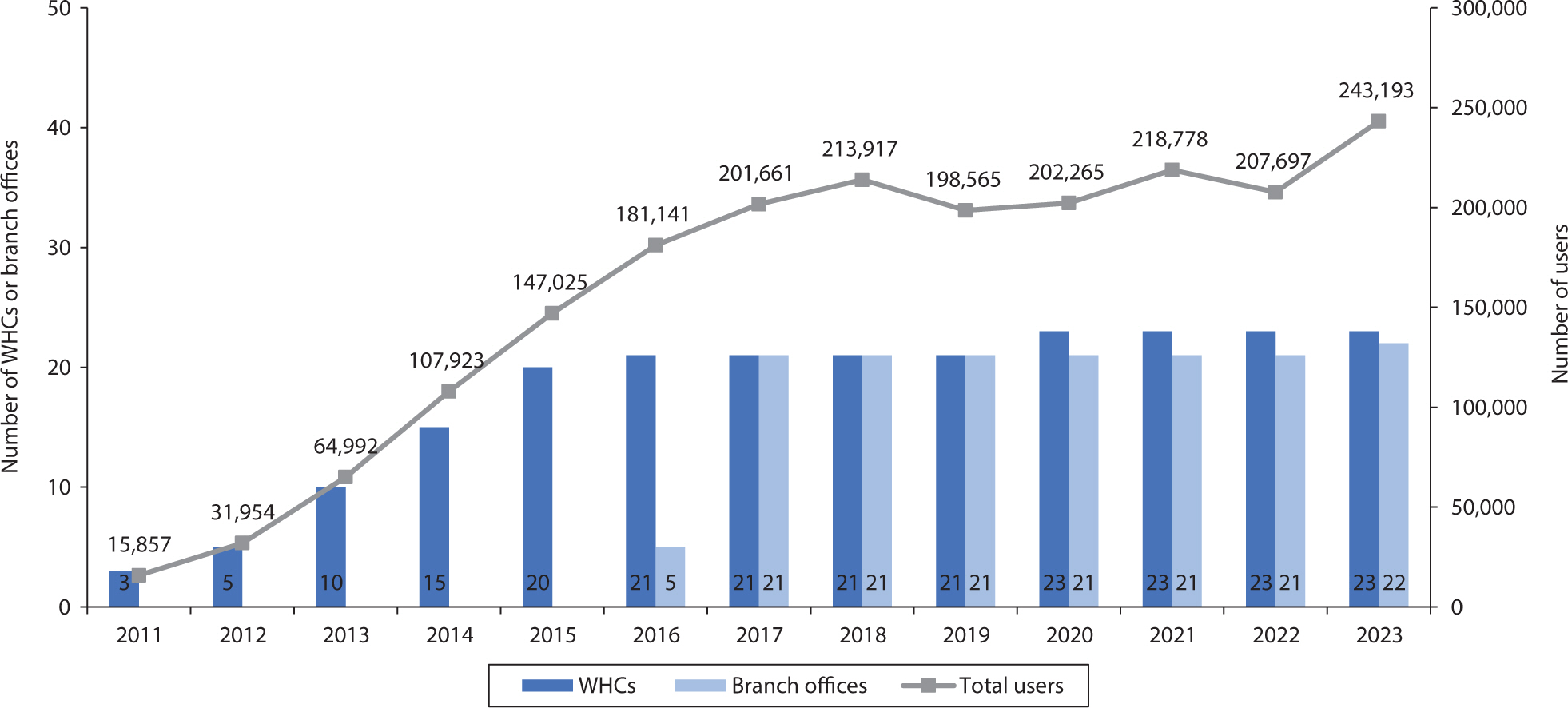
Performance of Workers’ Health Centers
The number of WHC users has increased alongside the rise in the number of
WHCs established (Fig. 2) [24,33,34]. In 2023, the
average cumulative number of users per center reached 8,864, equating to
about 35 users per day at each center. Employees of MSEs represent
approximately 88.5% of the total usage of these centers. As of 2019, 42.9%
of all users visited the centers for counseling, while 57.1% received this
service at their workplace [35]. User
satisfaction with WHCs is exceptionally high. Annually, from the end of
October to the end of November, a contracted company conducts a
telephone-based structured interview survey. For this survey, 80 users per
WHC and 35 users per branch office are randomly selected to participate. The
survey assesses various aspects such as convenience, equipment utilization,
staff attitudes, service expertise, appropriateness of consultation time,
and intention to reuse the services. In 2023, the overall satisfaction score
for WHCs and branch offices was an impressive 95.4 out of 100 [24].
Fig. 2.
The number of Workers' Health Centers (WHCs), branch
offices, and users by year.
The WHCs have played a key role in addressing social concerns related to
occupational diseases. In 2016, they carried out a health survey targeting
retired workers who had been exposed to methyl alcohol [21]. This initiative was in response to
several cases of methyl alcohol poisoning among subcontracted MSEs producing
smartphone components [36].
Furthermore, when instances of occupational diseases such as toxic liver
disease, lead, or arsenic poisoning were reported, health impact assessments
were performed for retired workers from the implicated factories [30]. In cases where radon-contaminated
consumer goods were detected, assessments were extended to both current and
retired workers from the affected workplaces [23]. Additionally, these centers provided support for
health counseling and the processing of claims for industrial accident
compensation insurance.
Discussion
Over the past 14 years, Korea's WHCs have developed slowly but steadily. These
centers focus on providing services to MSEs, where occupational health is often at
risk. Several factors contribute to the poor occupational health and safety observed
in MSEs. These include a "general and multifaceted lack of resources"
[2,37,38]. First, there is a lack of
understanding of legal obligations, especially those related to OSH. Additionally,
there is limited interest in OSH, minimal time devoted to it, and a general
indifference toward learning about improvement measures. Second, MSEs restrict
workers' access to the autonomous representation of their interests through
work councils and trade unions. Third, MSEs have less access to external health and
safety services compared to larger enterprises. Fourth, both workers and employers
in MSEs typically have limited experience. Lastly, inspections and controls are
infrequent. These conditions may be worsened by other vulnerabilities such as job
insecurity, the economic vulnerability of the enterprise, the ongoing threat of
unemployment, limited profitability, and the prevalence of illegal work and workers
associated with MSEs. All these issues are also relevant in the Korean context
[15].
To ensure that the WHCs in Korea effectively fulfill their role in promoting safety
and health in MSEs, several challenges must be addressed. Firstly, increasing WHC
acceptance among MSEs requires an understanding of their unique characteristics and
the development of diversified programs tailored to these attributes. MSE owners,
often entrepreneurs and craftsmen, have a strong sense of self-identity [2]. They see themselves as responsible
individuals who care for their workers and seek recognition for their commitment.
Consequently, identifying workplace risks might be perceived as an indirect
criticism, implying negligence or a failure to fulfill their responsibilities. This
perception can lead to resistance against external health management. Recognizing
these characteristics provides an opportunity to build trust with MSE owners.
Engaging in open, meaningful conversations can help address their concerns and
foster greater acceptance of workplace safety and health management programs [38]. A strategy that emphasizes trust and
dialogue—an action-driven, problem-solving-oriented, low-cost
approach—combined with aligning health and safety with other management
goals, has proven to be the most successful intervention method [38]. WHCs have been providing occupational
health services to communities for over 10 years, laying a foundation for
establishing credibility with MSEs and creating a structure that facilitates
collaboration across various professional fields. WHCs can play a crucial role in
case management, building strong relationships with these enterprises, and linking
them to other relevant programs, such as the Clean Workplace Project or financial
support programs for work environment assessments and special medical examinations.
It is also essential to diversify initiatives, not only by increasing the number of
WHC users but also by expanding into programs that prioritize addressing problems
specific to MSEs.
Legal regulations should be strengthened to enhance compliance among MSEs. In Korea,
these companies are partially exempt from certain regulations. To manage
occupational diseases effectively, employers must establish an occupational health
management system within their enterprises. The legal requirements for this vary
based on the company's size and the industry in which it operates. For
enterprises with more than 50 employees, health officers are appointed to provide or
oversee health management services. Workplaces with fewer than 300 employees have
the option to outsource their workplace health management services to external
organizations. While MSEs are required to assess their work environments and conduct
health checkups, they are not obligated to acquire workplace health management
services. This is in stark contrast to Finland, where it is mandatory for all
employers to provide comprehensive occupational health services, including
preventive services, to their employees [32].
Administrative oversight often overlooks MSEs, making it challenging to effectively
monitor compliance with systems such as work environment assessments and
workers’ health checks. This lack of supervision reduces the motivation of
MSEs to implement health management measures. WHC staff often encounter refusals
when attempting to arrange visits to workplaces, which they report as a significant
obstacle in fulfilling their responsibilities [32]. Active government efforts to strengthen regulations and improve OSH
infrastructure [39] are essential to
encourage MSEs to utilize occupational health services.
Additionally, measures should be taken to increase accessibility for MSEs and their
workers. In Korea, as in other countries, a significant portion of the workforce is
employed by small and medium-sized enterprises; nearly 2 million companies, or 98%
of all businesses, have fewer than 50 employees. Among these, approximately 62% of
employees work in MSEs, accounting for about 11 million workers [14]. The country is served by 24 WHCs, each
managing around 120,000 workplaces and 500,000 workers. Additionally, there is a
growing number of workers in non-traditional employment relationships, such as gig
workers. WHCs need to expand their services to better support these vulnerable
groups. The primary role of WHCs aligns with providing basic occupational health
services, delivered by community professionals [40]. These services are a fundamental right for all workers, and OSH
should be upheld without discrimination based on region, employment type, workplace
size, or other socioeconomic factors. However, the current number of WHCs,
established to address the needs of small enterprises and disadvantaged workers, is
woefully inadequate. A strategic plan for expanding WHCs should be developed with a
long-term perspective in mind [32,41,42].
Furthermore, with the rising number of migrant workers, it is crucial to develop
strategies to overcome language and cultural barriers to enhance the accessibility
of basic occupational health services.
Finally, an essential task is to develop a long-term strategy for the advancement of
WHCs, supported by the creation of an organization dedicated to this purpose. While
outsourced projects have been implemented to enhance WHCs, these efforts have
primarily focused on short-term improvements, leaving the directions for mid- to
long-term development unaddressed [31,32,41,42]. To ensure the effective
delivery of basic occupational health services, intermediate or secondary-level
support structures are necessary, in addition to national-level efforts [39]. KOSHA’s WHC department struggles to
fulfill its role as a control tower due to limited personnel and resources [31,32].
This underscores the urgent need for a WHC support organization equipped with the
expertise and capacity to serve as a central coordinating body. This organization
should be responsible for formulating long-term plans for WHCs, including their
expansion and the prioritization of service subjects. It should also tackle the
communication structure and governance to enhance coordination within WHCs and
between WHCs, KOSHA, the Ministry of Employment and Labor, and other relevant
agencies. The organization should focus on standardizing practices, developing new
approaches that incorporate emerging technologies, and providing comprehensive
training for WHC staff, emphasizing the center’s vision, goals, and basic
occupational health services. Enhancing the capacity of WHC staff to deliver both
occupational safety and health services, tailored to the specific needs and
circumstances of MSEs, would be beneficial. Additionally, the organization should
monitor program effectiveness, disseminate best practices from various centers, and
manage data generated by WHCs to inform future improvements. Establishing a robust
plan to ensure job security for WHC employees is also a critical priority.
WHCs were established in Korea to prevent occupational diseases in MSEs that have
minimal resources. These centers are the only public health centers dedicated to
providing basic occupational health services to vulnerable workers in the country
without seeking profit. To fulfill the mission of a WHC, the development of programs
should consider the unique characteristics of MSEs. OSH regulations should be
uniformly applied to these companies, and proactive policies should be targeted at
these entities due to their resource limitations. WHCs may be essential as case
managers, fostering strong relationships with MSEs and linking them to other
relevant programs. By emphasizing workplace-centered connections, WHCs contribute to
improving work environments, either independently or with support from KOSHA or
private institutions. A problem-solving-oriented approach is crucial; a balanced
strategy that integrates regulation with practical support is key to ensuring
success.
Authors' contributions
Project administration: not applicable
Conceptualization: Kong JO, Choi Y, Yang S, Jung-Choi K
Methodology & data curation: Jung-Choi K
Funding acquisition: not applicable
Writing – original draft: Jung-Choi K
Writing – review & editing: Kong JO, Choi Y, Yang S, Jung-Choi
K
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Kok JD, Berrios M. Small matters: global evidence on the contribution to employment by the
self-employed, micro-enterprises and SMEs. Geneva: International Labour Organization (ILO); 2019.
2. Walters D, Wadsworth E, Hasle P, Refslund B, Ramioul M. Safety and health in micro and small enterprises in the EU: final report
from the 3-year SESAME project. Luxembourg: Publications Office of the European Union; 2018.
3. Walters D. Health and safety in small enterprises: European strategies for managing
improvement. Brussels: Presses Interuniversitaires Européennes; 2001.
4. Serrano MR, Xhafa E. Industrial relations in micro and small enterprises: patterns, trends
and prospects. Geneva: International Labour Organization (ILO); 2024
5. Kim I, Min J. Working hours and the regulations in Korea. Ann Occup Environ Med 2023;35:e18.
7. European Agency for Safety and Health at
Work. Contexts and arrangements for occupational safety and health in micro
and small enterprises in the EU: SESAME projects. Luxembourg: Publications Office of the European Union; 2016.
8. Park H, Ha E, Kim J, Jung H, Paek D. Occupational health services for small-scale enterprises in
Korea. Ind Health 2002;40(1):1-6.
9. Ministry of Employment and Labor. 2022 Industrial accident status. Sejong: Ministry of Employment and Labor; 2023.
10. Yang M, Myong JP, Lee J, Park MY, Kang MY. Association between irregular working hours and work-related
musculoskeletal pain: results from the 6th Korean Working Conditions
Survey. Ann Occup Environ Med 2023;35:e21.
11. Park J, Park J, Han B, Kim Y. Vulnerability of employees in businesses with fewer than five
workers (micro-enterprises) to occupational safety and health
problems. Am J Ind Med 2017;60(12):1056-1065.
16. Presidential Advisory Council on Policy
Planning. Response to low birthrate and aging society. Seoul: Presidential Advisory Council on Policy
Planning; 2008.
17. National Archives of Korea. Major policy records guidebook: welfare section (National Archives of
Korea). Daejeon: National Archives of Korea; 2015.
18. Kim JS, Kim DS, Gil HJ, Park YS, Sin HH, Park JT. The significance and prospects of the Workers’ Health
Center. J Korean Med Assoc 2014;57(2):159-166.
19. Lee SU, Kim DS, Gang SG. Regional Occupational Health Promotion Center in Korea for the
purpose of promoting health of small-scale industry workers-assessment of
the first year's results. Ind Health 2008;(8):54-55.
20. Nam KC, Park JS, Koh JW, Kim JS, Park JT, Kim HJ, et al. An assessment of the needs and the affecting factors for small
scale enterprise Worker’s Health Centers. Korean J Occup Environ Med 2011;23(4):407-419.
21. Korea Occupational Safety and Health Agency. 2016 Workers' Health Center establishment and operation
comprehensive results. Ulsan: Korea Occupational Safety and Health Agency; 2017.
22. Korea Occupational Safety and Health Agency. 2012 Workers' Health Center work performance guide. Ulsan: Korea Occupational Safety and Health Agency; 2012.
23. Korea Occupational Safety and Health Agency. 2018 Comprehensive results of Workers' Health Center and branch
operations. Ulsan: Korea Occupational Safety and Health Agency; 2019.
24. Korea Occupational Safety and Health Agency. 2023 Comprehensive results of Workers' Health Center and branch
perations. Ulsan: Korea Occupational Safety and Health Agency; 2024.
25. Korea Legislation Research Institute. Occupational Safety And Health Act. Sejong: Korea Legislation Research Institute; 2013.
26. Ministry of Employment and Labor. Notification No. 2013-6 of the Ministry of Employment and Labor. Sejong: Ministry of Employment and Labor; 2013.
27. Korea Legislation Research Institute. Occupational Safety And Health Act. Sejong: Korea Legislation Research Institute; 2019.
28. Ministry of Employment and Labor. Notification No. 2020-19 of the Ministry of Employment and
Labor. Sejong: Ministry of Employment and Labor; 2020.
29. Korea Occupational Safety and Health Agency. 2022 Comprehensive results of Workers' Health Center
operations. Ulsan: Korea Occupational Safety and Health Agency; 2023.
30. Korea Occupational Safety and Health Agency. 2017 Workers' Health Center establishment and operation
comprehensive results. Ulsan: Korea Occupational Safety and Health Agency; 2018.
31. Chung HJ, Kim SH, Rheu HC, Park JH, Lee JH, Yoo BH, et al. A study on developing improvement plans for the commissioned operation
of Workers' Health Centers. Ulsan: Korea Occupational Safety and Health Agency; 2022.
32. Han BS, Kim SK, Choi EH, Kim HR, Jung TS, Lee JS, et al. A study on developing mid- to long-term development plans for
Workers' Health Centers. Ulsan: Korea Occupational Safety and Health Agency; 2018.
33. Korea Occupational Safety and Health Agency. 2020 Comprehensive results of Workers' Health Center and branch
operations. Ulsan: Korea Occupational Safety and Health Agency; 2021.
34. Korea Occupational Safety and Health Agency. 2021 Comprehensive results of Workers' Health Center and branch
operations. Ulsan: Korea Occupational Safety and Health Agency; 2022.
35. Korea Occupational Safety and Health Agency. 2019 Comprehensive results of Workers' Health Center and branch
operations. Ulsan: Korea Occupational Safety and Health Agency; 2020.
36. Ryu J, Lim KH, Ryu DR, Lee HW, Yun JY, Kim SW, et al. Two cases of methyl alcohol intoxication by sub-chronic
inhalation and dermal exposure during aluminum CNC cutting in a small-sized
subcontracted factory. Ann Occup Environ Med 2016;28:65
37. Choi SM, Kim CW, Park HO, Park YT. Association between unpredictable work schedule and work-family
conflict in Korea. Ann Occup Environ Med 2023;35:e46.
38. Laird I, Olsen K, Harris LA, Legg S, Perry MJ. Utilising the characteristics of small enterprises to assist in
managing hazardous substances in the workplace. Int J Workplace Health Manag 2011;4(2):140-163.
39. Rantanen J. Basic occupational health services. 3rd ed. Geneva: International Labour Organization (ILO); 2007.
40. Rantanen J. Basic occupational health services: their structure, content and
objectives. Scand J Work Environ Health Suppl 2005;(1):5-15.
41. Joo YS, Noh SC, Lim J, Lim HJ, Jung YK, Bang YW, et al. A study on establishing operational models and developing performance
indicators for the expanded installation of Workers' Health
Centers. Ulsan: Korea Occupational Safety and Health Agency; 2013.
42. Yang SH, Kang DM, Kang MY, Kim W, Kim JI, Rheu HC, et al. A study on improvement plans for the roles and functions of
Workers' Health Centers. Ulsan: Korea Occupational Safety and Health Agency; 2016.
Figure & Data
References
Citations
Citations to this article as recorded by
Topic modeling of workplace bullying discourse following legal regulation in South Korea Hyunjoo Oh, Yeajoo Kim, Hipyo Ahn, Dong-gwi Lee Frontiers in Public Health.2026;[Epub] CrossRef
Biological Monitoring as a Preventive Occupational Healthcare Tool: Urinary Biomarkers of Benzene and Toluene Exposure Among Small-Scale Printing Workers in South Korea Jungho Hwang, Yangwoo Kim, Inah Kim, Seoyeon Kim, Juyeoung Hwang, Hyein Park, Ki-Youn Kim Healthcare.2026; 14(13): 1856. CrossRef
Challenges from 14 years of experience at Workers' Health
Centers in basic occupational health services for micro and small enterprises in
Korea: a narrative review
Fig. 1.
Distribution of Workers' Health Centers (WHCs) in
Korea.
Fig. 2.
The number of Workers' Health Centers (WHCs), branch
offices, and users by year.
Fig. 1.
Fig. 2.
Challenges from 14 years of experience at Workers' Health
Centers in basic occupational health services for micro and small enterprises in
Korea: a narrative review
Workers’ health centers, branch offices, and trauma
counseling centers for workers by region and operating agencies in
Korea
Region
Workers’ Health Center
(WHC)
Branch office (BO)
Trauma counseling center for
workers
Operating agency
Seoul
Seoul WHC
Seoul Jung-gu BO
○
Ewha University-Industry
Collaboration Foundation
Seoul Western WHC
Seoul Seongdong BO
○
Seoul National University Research
and Development Business Foundation
Busan
Busan WHC
Yangsan BO
○
Busan University Research and
Business Development Foundation
Daegu
Daegu WHC
Seodaegu BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Daegu Dalseong BO
Incheon
Incheon WHC
Incheon Bupyeong BO
○
Yonsei University
University-Industry Foundation
Gwangju
Gwangju WHC
Gwangju Gwangsan BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Daejeon
Daejeon WHC
-
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Ulsan
Ulsan WHC
Ulsan Buk-gu BO
○
Dong-a
University Industry-Academy Cooperation
Foundation
Gyeonggi-do
Gyeonggi Western WHC
Gunpo BO
○
Korea University Research and
Business Foundation
Gyeonggi Eastern WHC
Seongnam BO
○
The Catholic University of Korea,
Industry-Academic Cooperation Foundation.
Bucheon WHC
Gimpo Yangchon BO
○
The Catholic University of Korea,
Industry-Academic Cooperation Foundation
Gimpo Gochon BO
Gyeonggi Southern WHC
Pyeongtaek BO
○
Korea Workers’ Compensation
& Welfare Service Ansan Hospital
Gyeonggi Northern WHC
Namyangju BO
○
Gachon University
Industry-Academic Cooperation Foundation
Gangwon special self-governing
province
Gangwon WHC
Chuncheon BO
○
Yonsei University Wonju Severance
Christian Hospital
Chungcheongbuk-do
Chungbuk WHC
-
○
Korea Industrial Health
Association
Chungcheongnam-do
Chungnam WHC
Asan BO
○
Dankook University
Industry-Academia Cooperation Foundation
Chungnam Western WHC
-
-
Mirae Hygiene Environment
Institute Co., Ltd.
Jeonbuk special self-governing
province
Jeonbuk WHC
Wanju BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Jeollanam-do
Jeonnam Eastern WHC
-
○
Won-jin Foundation for
occupational diseases Green Hospital
Jeonnam Western WHC
-
-
Mokpo National University
Industry-Academic Cooperation Foundation
Gyeongsangbuk-do
Gyeongbuk Northern WHC
Gumi BO
○
Gumi Ganddong Hospital
Gyeongsan WHC
Yeongcheon BO
○
Korean Association of Occupational
Health Nurses, Incorporated Association
Gyeongsangnam-do
Gyeongnam WHC
Changwon BO
○
Teo Occupational and Environmental
Medicine Center
-
Geoje BO
○
Daewoo Medical Foundation
Jeju special self-governing
province
Jeju WHC
Jeju Yeon-dong BO
○
Cheju Halla General Hospital
Table 1.
Workers’ health centers, branch offices, and trauma
counseling centers for workers by region and operating agencies in
Korea