Review Special topic: recent clinical approach to shoulder diseases in older adults
Radiological characteristics of shoulder diseases in older adults,
including adhesive capsulitis, rotator cuff tear, and osteoarthritis of the
glenohumeral joint: a narrative review
1Department of Orthopaedic Surgery, Shoulder & Elbow Clinic, Kyung Hee University College of Medicine, Kyung Hee University Hospital at Gangdong, Seoul, Korea
*Corresponding author: Myung-Seo Kim,
Department of Orthopaedic Surgery, Shoulder & Elbow Clinic, Kyung Hee
University College of Medicine, Kyung Hee University Hospital at Gangdong, 892
Dongnam-ro, Gangdong-gu, Seoul 05278, Korea, E-mail:
84g-t@hanmail.net
• Received: November 15, 2024 • Revised: December 24, 2024 • Accepted: January 9, 2025
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Shoulder diseases, including adhesive capsulitis, rotator cuff tear, and
osteoarthritis of the glenohumeral joint, can significantly impair daily
activities in older adult patients. This review aims to examine the radiologic
findings associated with these shoulder conditions in older patients, providing
insights for accurate diagnosis and effective treatment. Adhesive capsulitis,
commonly known as frozen shoulder, leads to pain and restricted movement,
thereby causing shoulder dysfunction. Recent advances in diagnostic technology
have greatly enhanced the sensitivity and accuracy of diagnosing this condition
through radiologic evaluations, including MRI, magnetic resonance arthrography
(MRA), and high-resolution ultrasound. Rotator cuff disease is another frequent
issue in older adults, with full-thickness tears occurring in 50%–80% of
cases. Both MRI and MRA are highly sensitive and specific in identifying rotator
cuff tears. Additionally, ultrasonography is recognized for its high sensitivity
and specificity in detecting tears of the supraspinatus tendon. Although
osteoarthritis of the glenohumeral joint is less commonly prevalent, its
advanced stages can severely affect the function of the upper extremity. Plain
radiography is typically the first imaging technique used to assess this type of
osteoarthritis. As the condition worsens, CT is utilized to measure glenoid bone
loss, glenoid version, and inclination, which are crucial for accurate surgical
planning. Each imaging modality provides distinct benefits: plain radiographs
for initial structural assessment, ultrasonography for real-time evaluation of
soft tissues, MRI/MRA for detailed visualization of capsular and tendinous
lesions, and CT for precise bony analysis.
Previous studies have indicated that shoulder pain affects approximately 20% of
individuals over the age of 65, ranking it as the third most common source of
pain following back and knee pain [1].
Common conditions associated with shoulder pain include adhesive capsulitis,
rotator cuff tears, and osteoarthritis of the glenohumeral joint [2,3].
Without proper diagnosis and treatment, these shoulder pathologies may progress,
leading to pain and functional impairment that complicates daily activities
[4–8]. Advances in diagnostic techniques now allow for the
identification of diseases causing shoulder pain with high sensitivity and
accuracy through the use of MRI, magnetic resonance arthrography (MRA), and
ultrasonography [9]. For glenohumeral
joint arthritis, surgical planning can be facilitated by radiography and CT
[10]. Therefore, it is essential for
healthcare providers to be well-versed in the radiologic characteristics of
common shoulder pathologies in older adults.
Objectives
This article reviews the radiologic findings associated with shoulder diseases in
older adults, offering insights for accurate diagnosis and effective
treatment.
Ethics statement
As this study was a literature review, it did not require approval from the
institutional review board or individual consent.
Adhesive capsulitis
Plain radiography
Plain radiography typically shows no significant findings in patients with
adhesive capsulitis [11]. Its primary
utility is to differentiate diseases such as calcific tendinitis or
osteoarthritis that may cause shoulder pain [12].
Ultrasonography
As technological advances in ultrasound have improved the accurate visualization
of shoulder joint structures, it is increasingly being used to examine patients
with adhesive capsulitis, leveraging its dynamic and non-invasive advantages
[13]. The radiological
characteristics observable in patients with adhesive capsulitis via ultrasound
include the following.
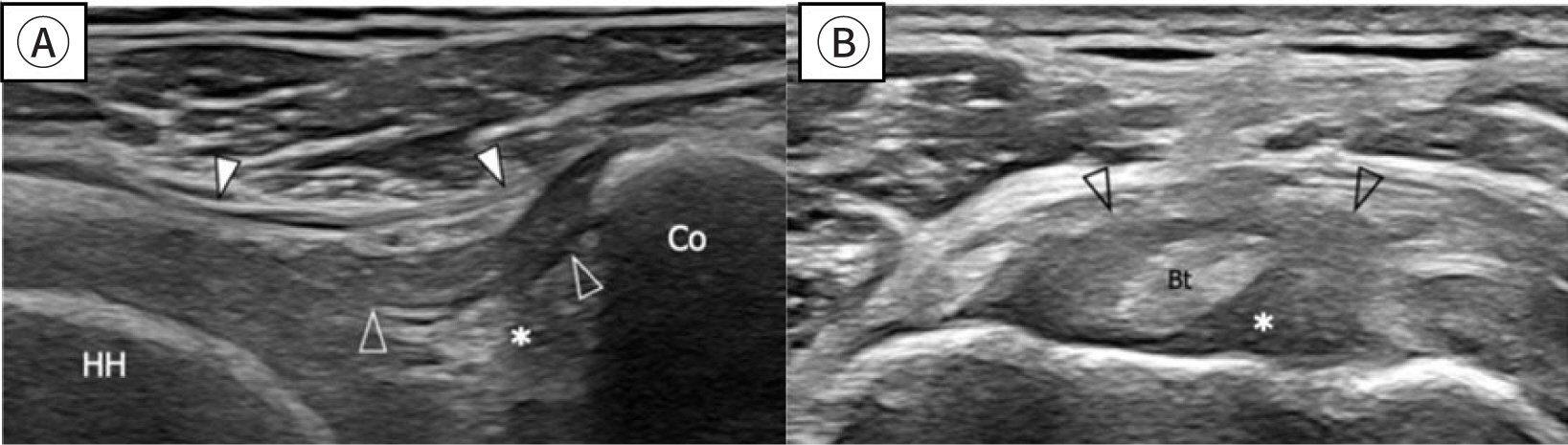
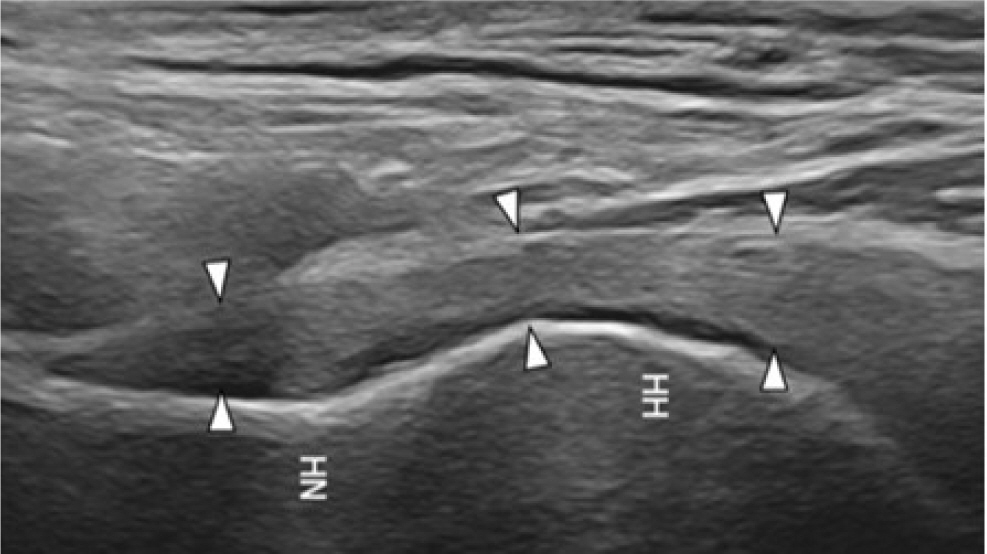
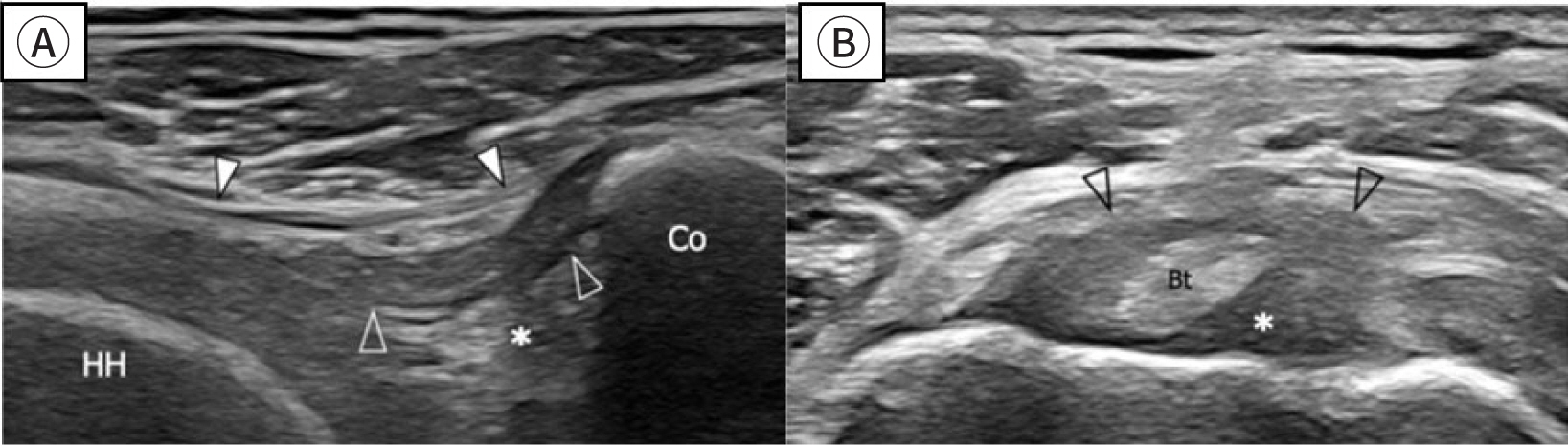
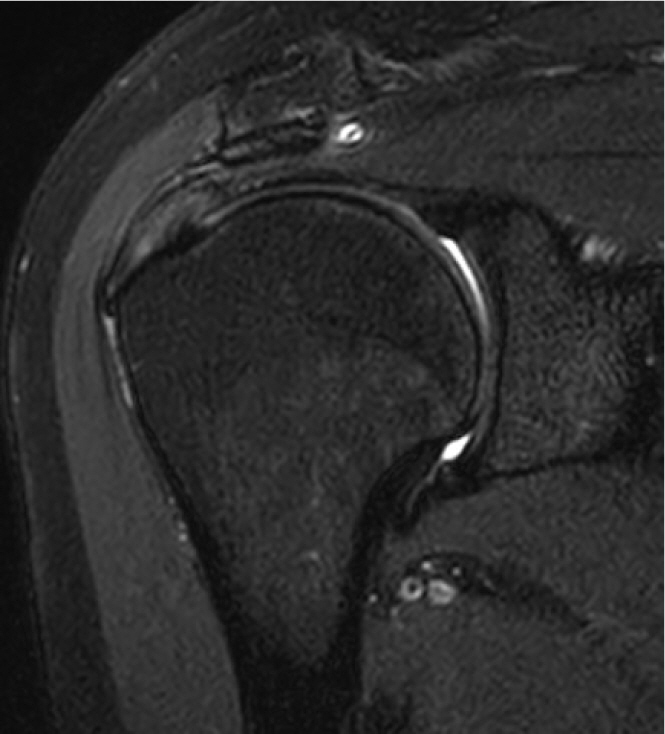
- Coracohumeral ligament, inferior glenohumeral capsule thickening, and
rotator interval abnormality (88% sensitivity and 96% specificity; Figs. 1, 2) [5,9,14,15]
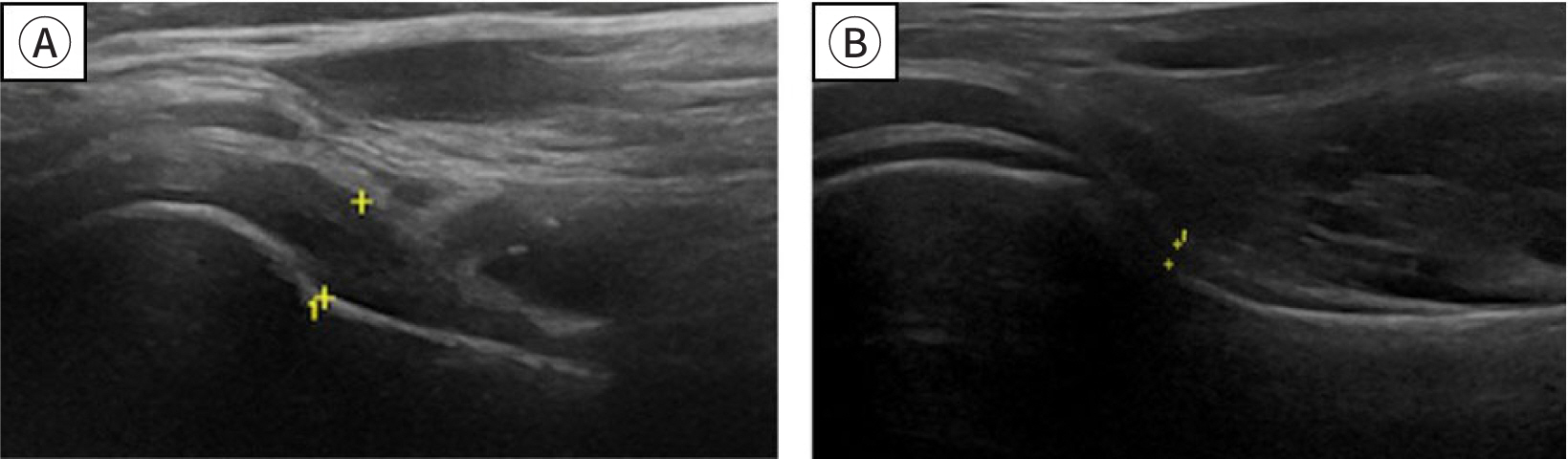
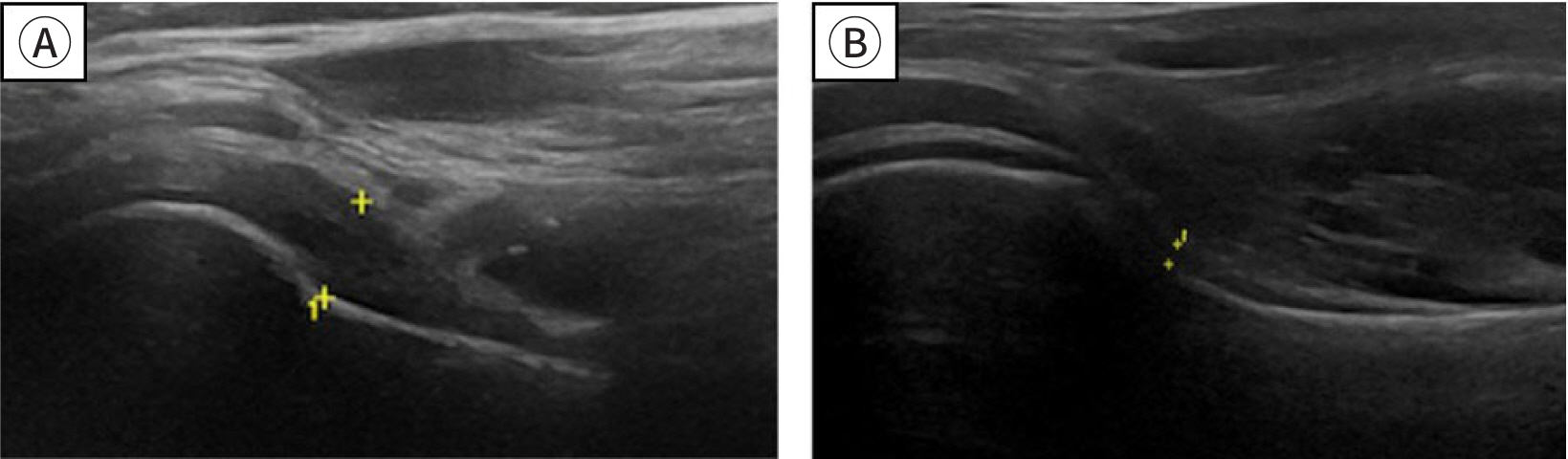
- Thickening of the axillary pouch, as illustrated in Fig. 3, is a notable finding [16,17]
- Increased vascularity in the rotator interval [18]
Fig. 1.
Ultrasonography. Thickened coracohumeral ligament, oblique transverse
image (A), short axis image (B). Adapted from Picasso et al. [5] with CC-BY.
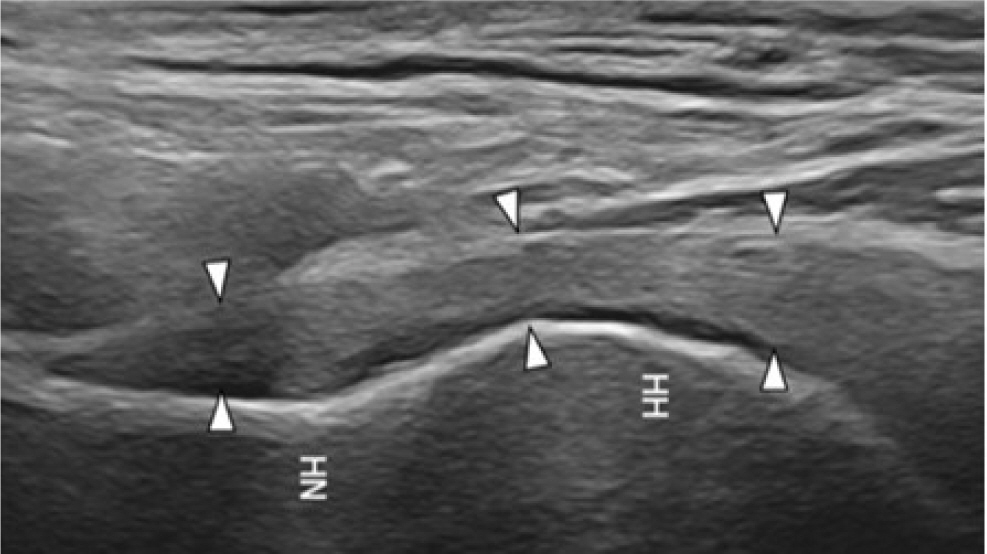
Fig. 2.
Ultrasonography. Thickened inferior glenohumeral capsule,
longitudinal image. Adapted from Picasso et al. [5] with CC-BY.
Fig. 3.
Ultrasonography, oblique axial section. Thickened axillary pouch (A),
normal axillary pouch (B). Adapted from Tue et al. [17] with CC-BY.
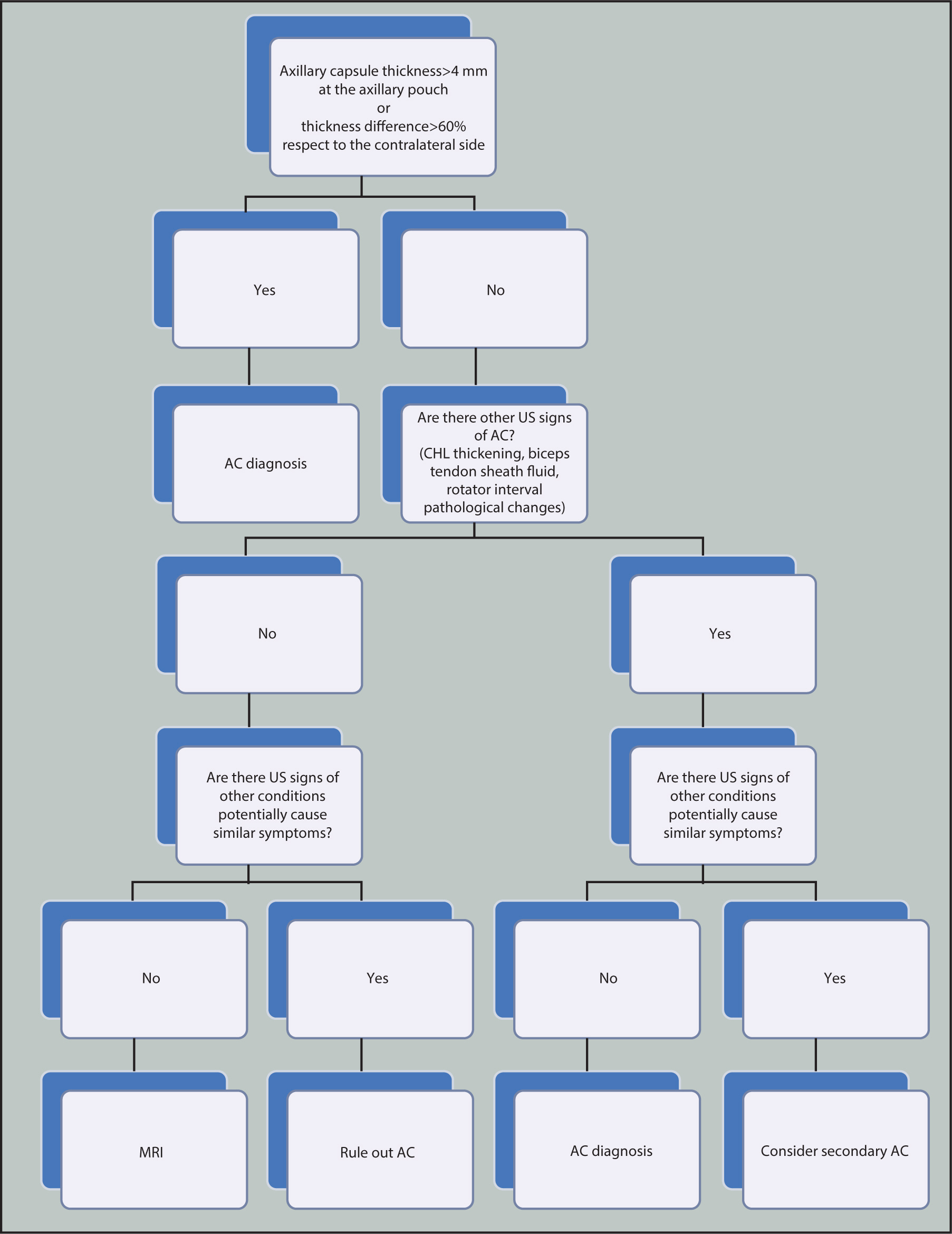
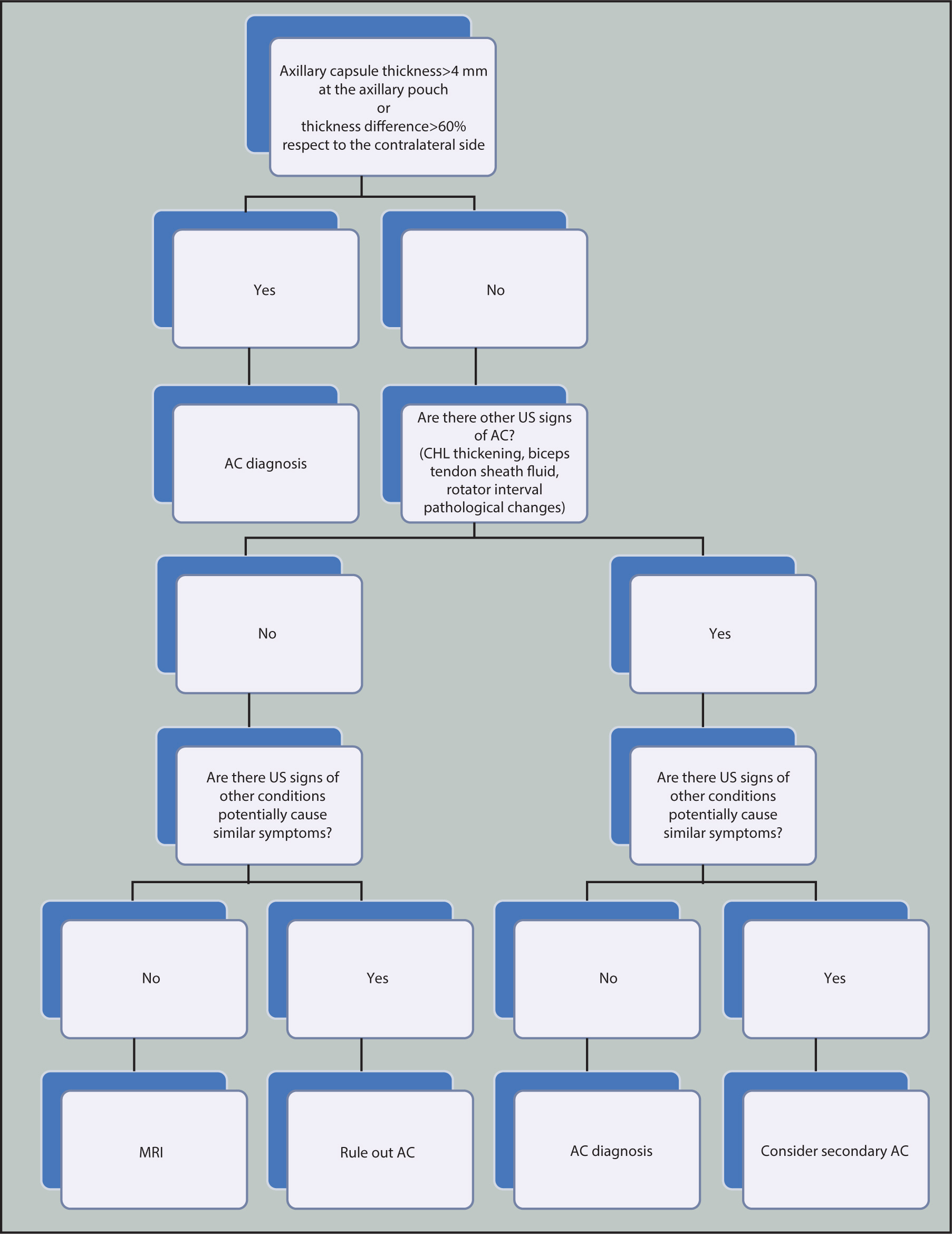
Recently, a protocol for diagnosing adhesive capsulitis using ultrasonographic
findings has been proposed. Ultrasonography is reported to be a valuable
diagnostic tool for patients with adhesive capsulitis (Fig. 4) [5].
Fig. 4.
Protocol for imaging evaluation using ultrasonography in patients
with adhesive capsulitis. Adapted from Picasso et al. [5] with CC-BY.
MRI and magnetic resonance arthrography
MRI is considered the gold standard for assessing the entire glenohumeral capsule
and pericapsular soft tissue in cases of adhesive capsulitis [5]. A recent systematic review and
meta-analysis of MRI radiological characteristics in adhesive capsulitis
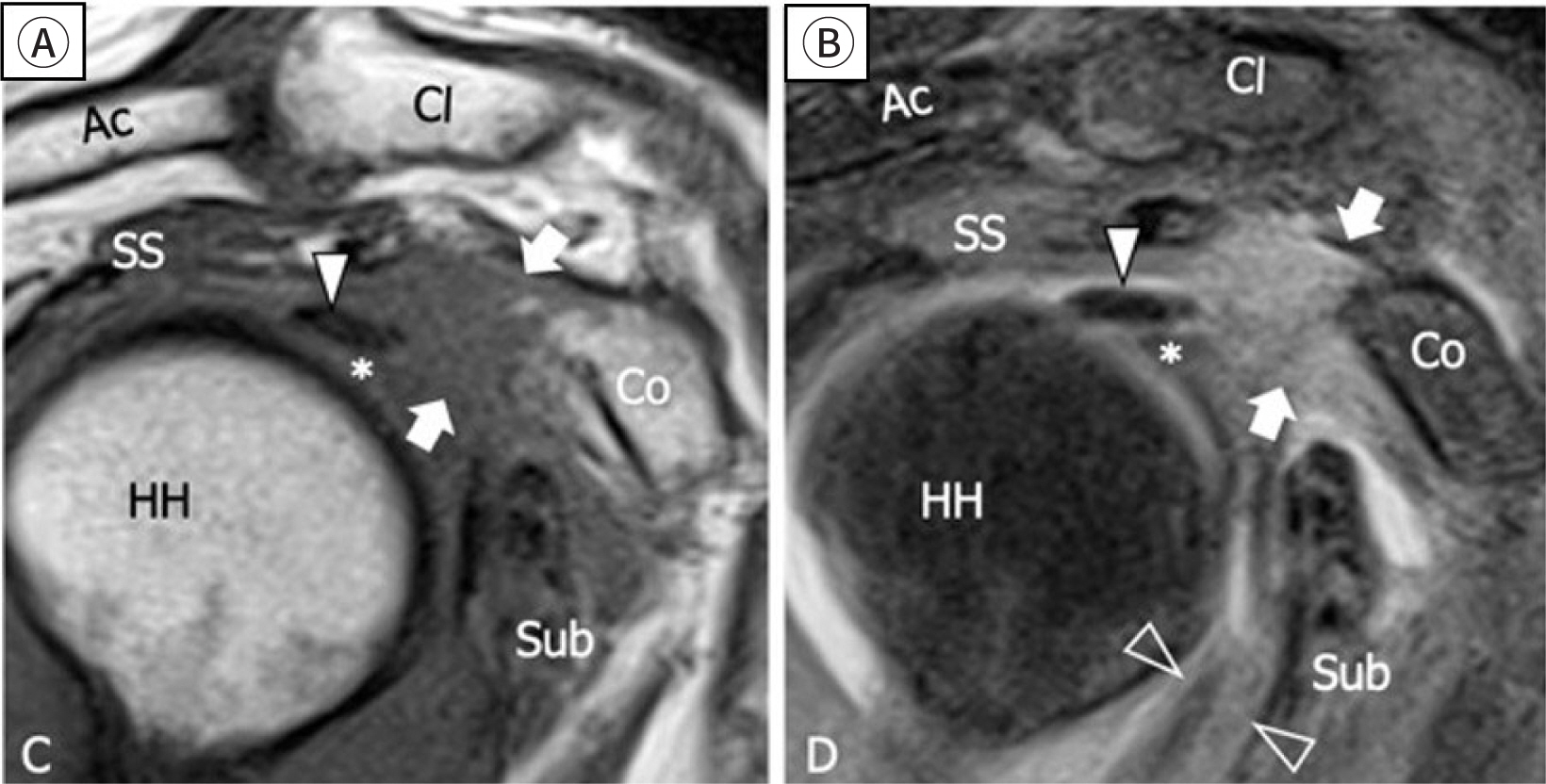
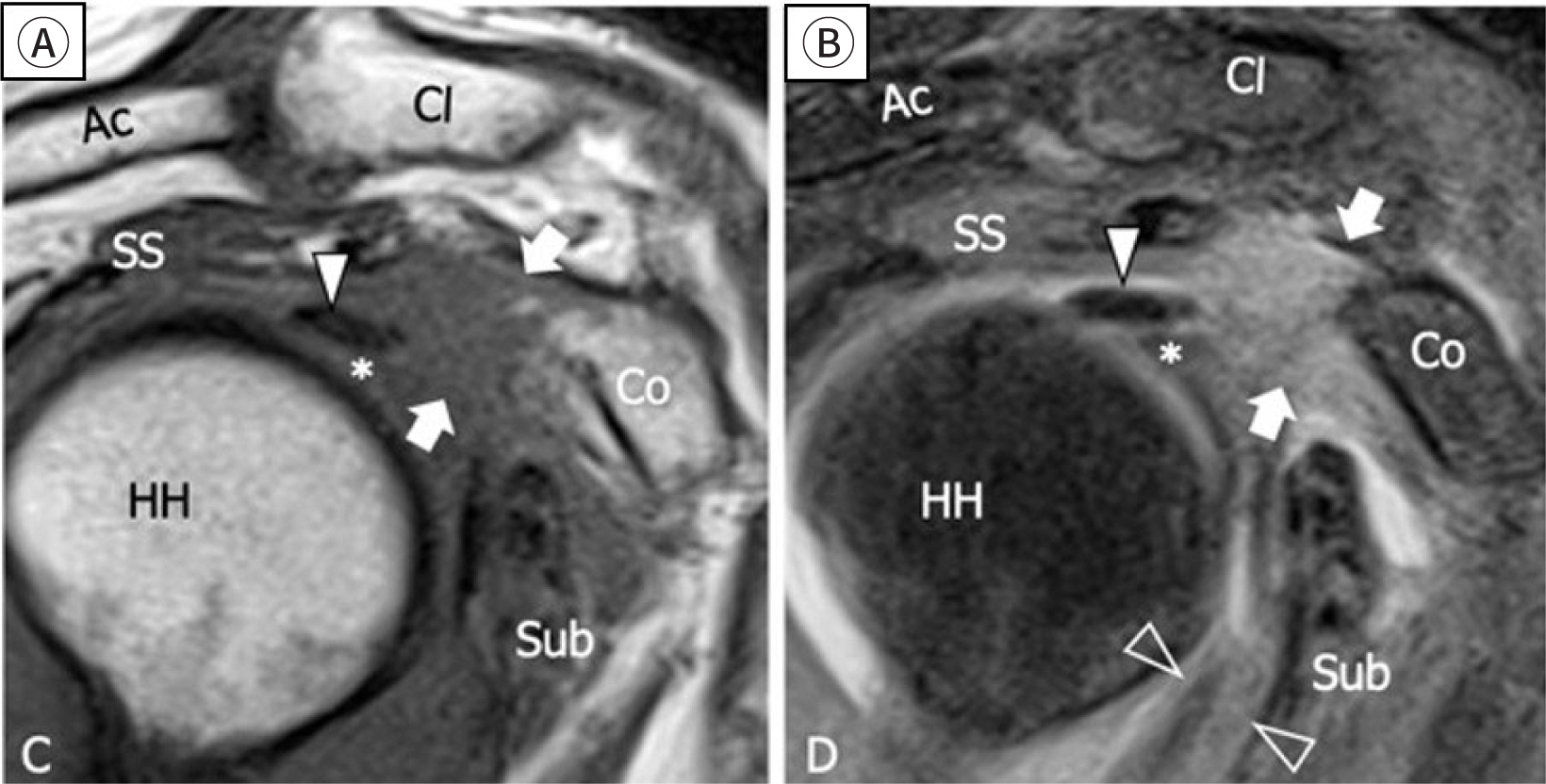
identified six significant findings (Fig.
5) [5,19].
- Coracohumeral ligament thickening and fat obliteration of the rotator
interval [5,20]
- Inferior glenohumeral ligament hyperintensity and thickening
(85.3%–88.2% sensitivity and 88.2% specificity) [21]
- Obliteration of the subcoracoid fat triangle by hypointense
synovium
- Contrast enhancement of the axillary joint capsule and the rotator
interval [22]
Fig. 5.
Sagittal T1 and T2-weighted MRI scan. Fat obliteration (arrow),
thickened and hyperintensity of the anteroinferior capsule (outlined
arrowhead; A,B). Adapted from Picasso et al. [5] with CC-BY. SS, supraspinatus; Ac, acromion; CI,
clavicle; Co, coracoid process; Sub, subscapularis; HH, humeral
head.
MRI and MRA are crucial diagnostic tools for identifying specific radiologic
characteristics of adhesive capsulitis, thereby playing a significant role in
understanding the disease's nature [11].
Rotator cuff tear
Plain radiography
Plain radiography is typically the first step in assessment due to its speed, low
cost, and broad availability [23]. While
it does not allow for direct evaluation of the rotator cuff, it can reveal
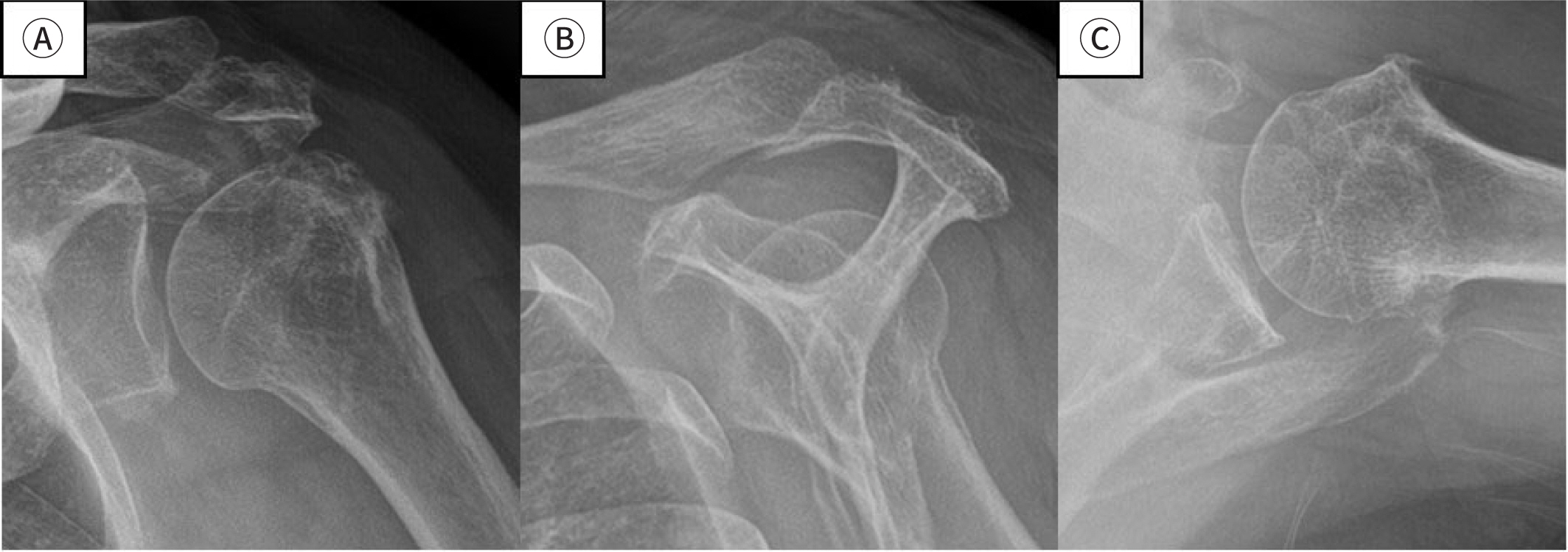
osseous abnormalities linked to impingement. Anteroposterior, outlet, and
axillary views are taken, and certain findings indicative of chronic rotator
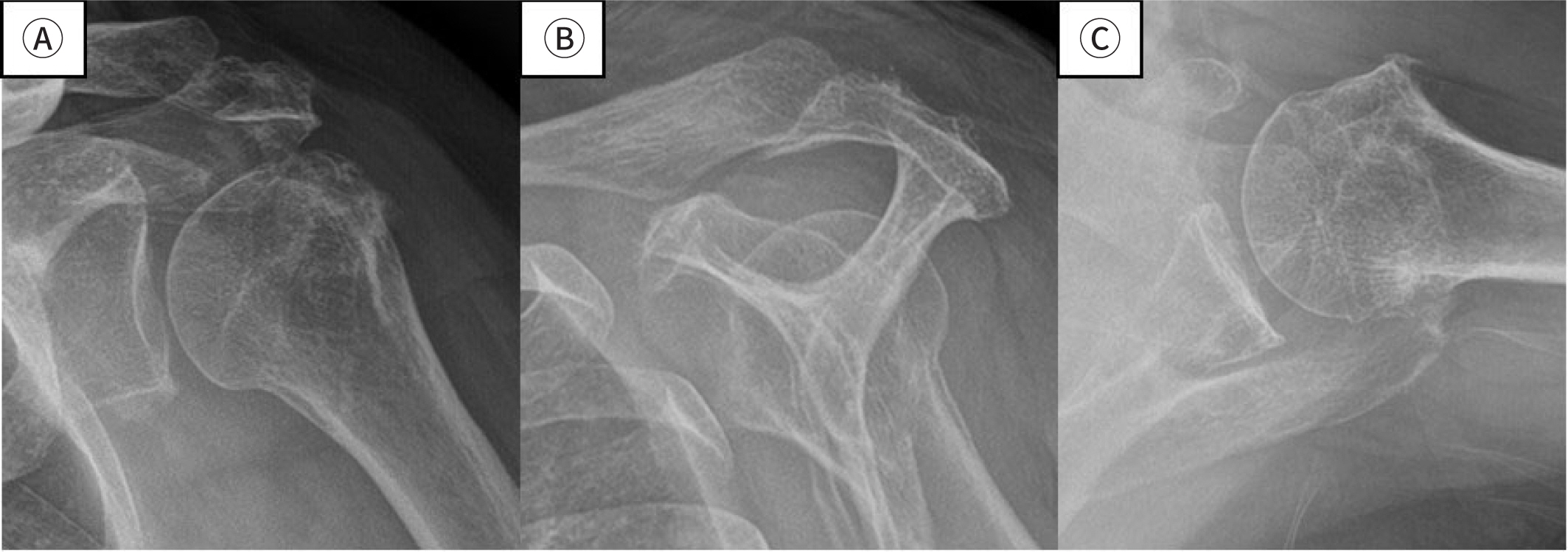
cuff tears can be observed on these radiographs (Fig. 6) [24].
- Anteroposterior view: reduction of subacromial space, subacromial
enthesophyte, and cystic change with sclerosis of the acromion and
greater tuberosity [25]
- Outlet view: coracoacromial arch and the morphology of the anterior
acromion (flat, curved, or hooked)
- Axillary view: Details of the glenoid, glenohumeral alignment,
coracohumeral interval, and os acromiale [24]
Fig. 6.
Plain image. True anteroposterior view (A), outlet view (B) and
axillary view (C). Provided by the authors.
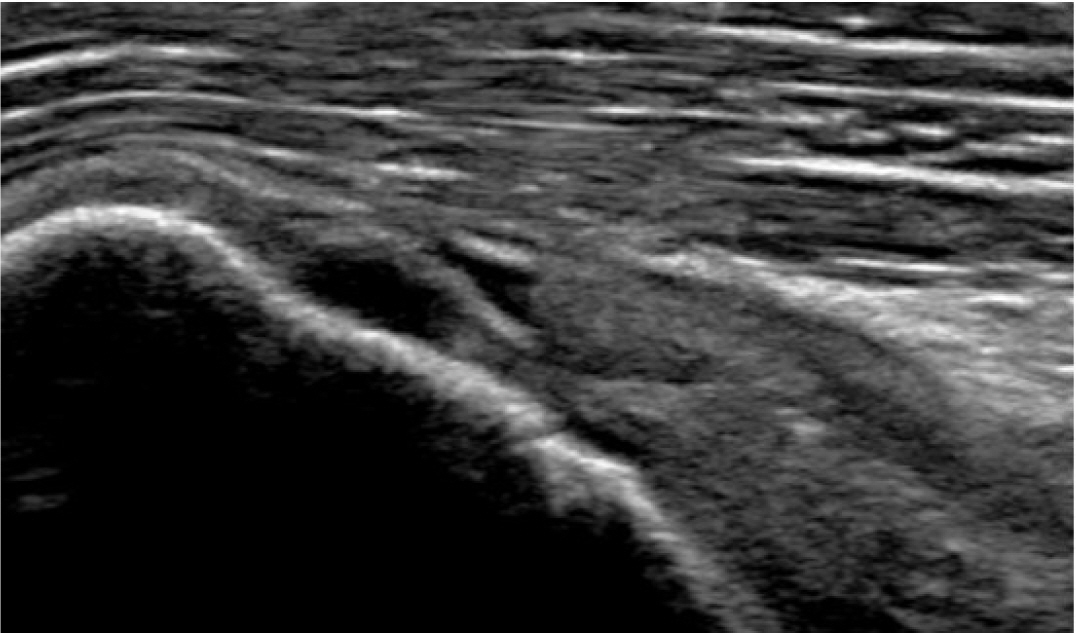
Ultrasonography
Ultrasound is a crucial diagnostic tool with sensitivity and specificity
comparable to 1.5T MRI, particularly effective in diagnosing full-thickness
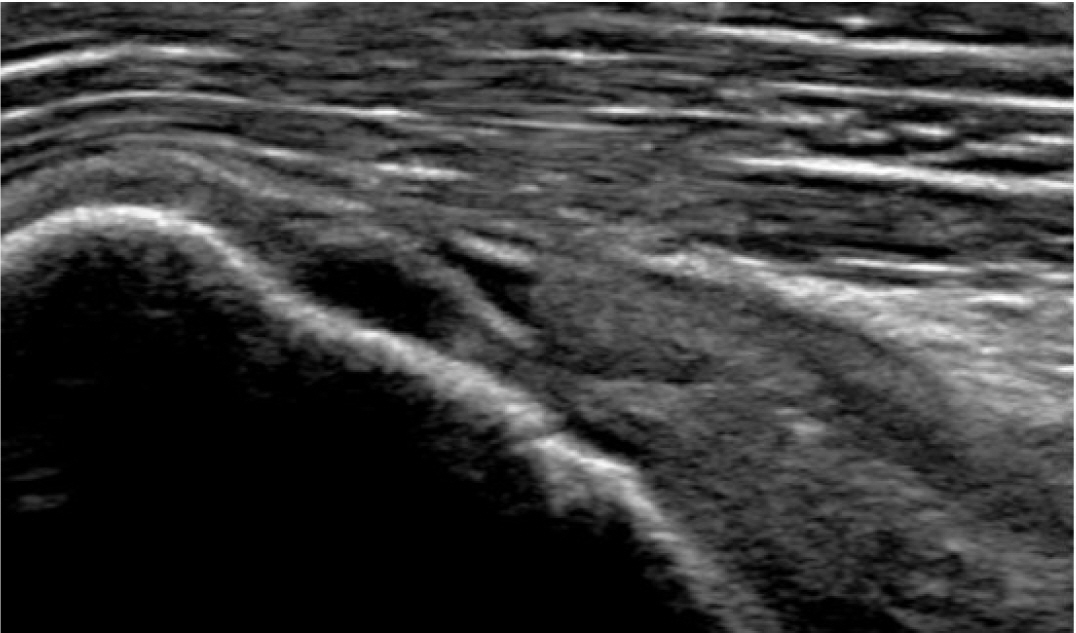
rotator cuff tears [26]. In cases of
full-thickness rotator cuff tendon tears, the defect in the cuff typically
appears hypoechoic or anechoic. This is accompanied by irregularities in the
greater tuberosity and pitting caused by the tear (Fig. 7) [24,27].
Fig. 7.
Longitudinal plane ultrasound image of supraspinatus tendon. Anechoic
gap and pitting due to tear. Provided by the authors.
MRI and magnetic resonance arthrography
MRI is effective in evaluating both bone and soft tissue, establishing it as a
precise diagnostic tool for confirming rotator cuff pathology. MRA, on the other
hand, shows almost perfect sensitivity and specificity in detecting
full-thickness rotator cuff tears, with values nearing 100% [28].
Rotator cuff tendinopathy, two hallmarks (Fig. 8) [29,30]
- Abnormal increased signal within the substance of the cuff (without
extension to the articular or bursal side)
- Swelling or increased thickness of the tendon
Fig. 8.
Oblique coronal fat-suppressed T2-weighted MRI scan. Abnormal
high signal and focal swelling of the supraspinatus tendon. Provided
by the authors.
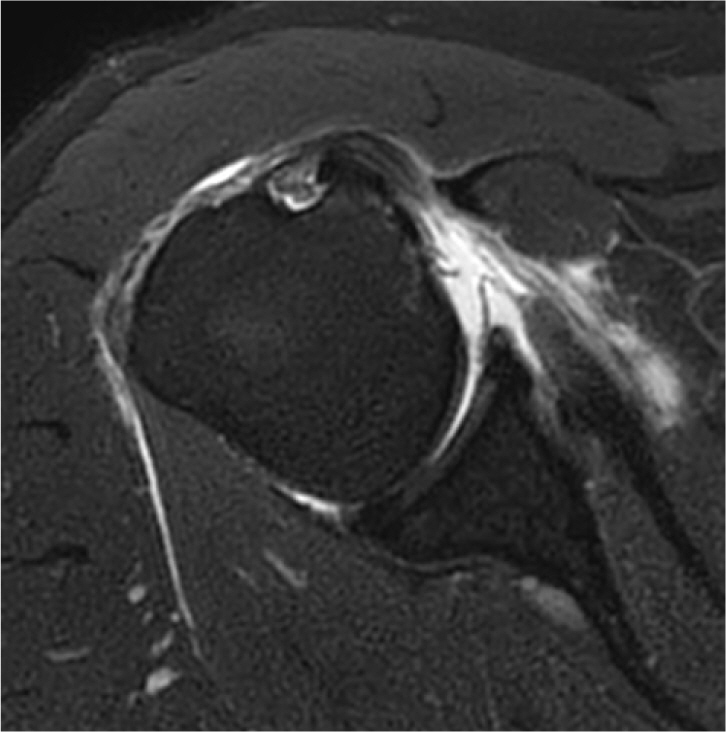
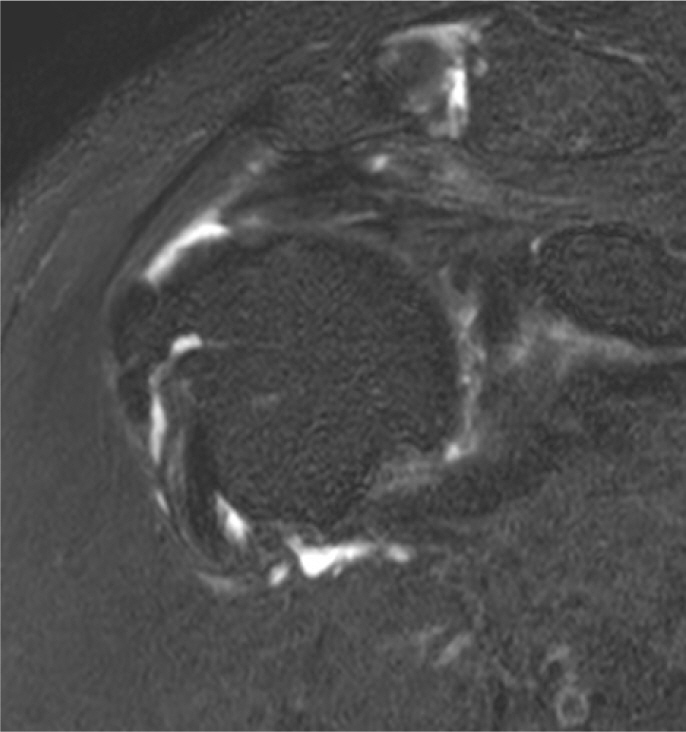
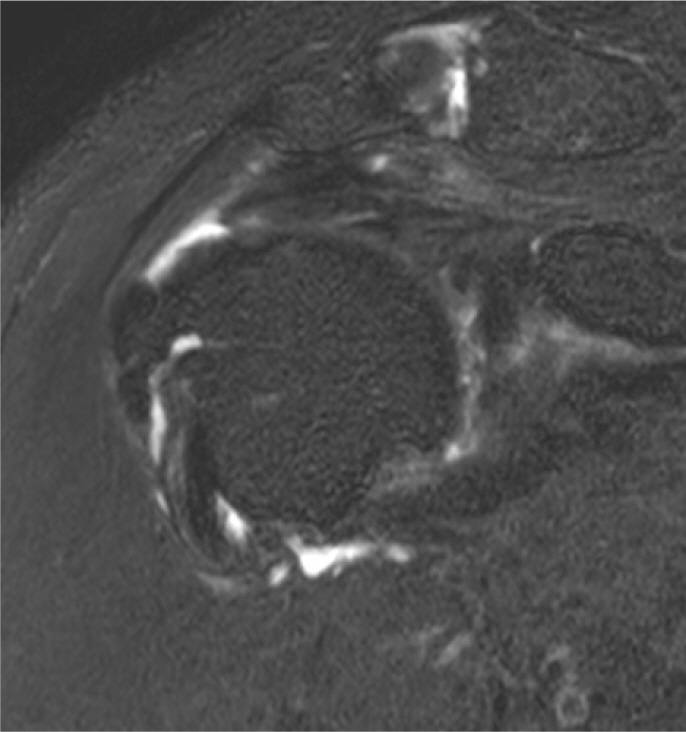
Rotator cuff tear
- Supraspinatus
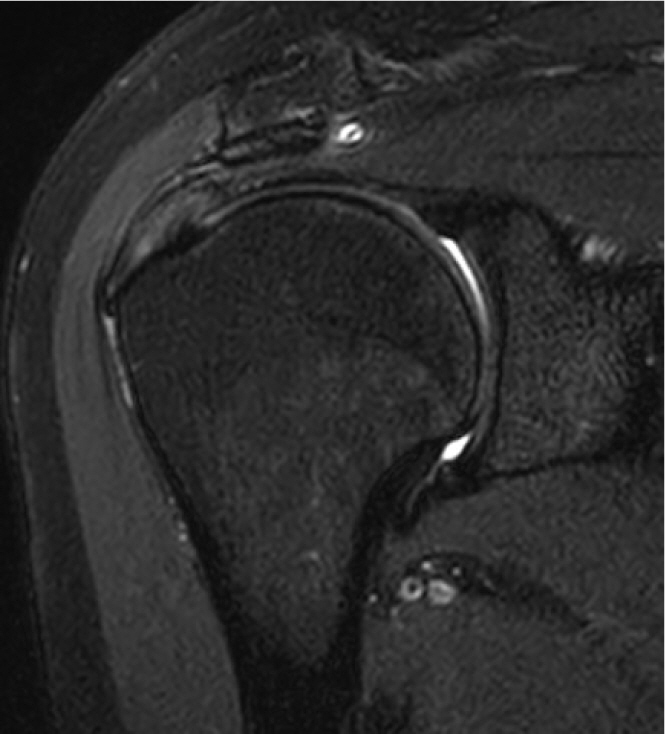
The most commonly observed radiological feature in full-thickness rotator
cuff tears is high signal fluid intensity extending from the glenohumeral
joint to the subacromial bursa (Fig. 9)
[31]. In approximately 10% of
patients, a low-signal tear is noted when the humeral head migrates
superiorly, resulting in an absence of cuff tissue between the humeral head
and the subacromial bursa [30].
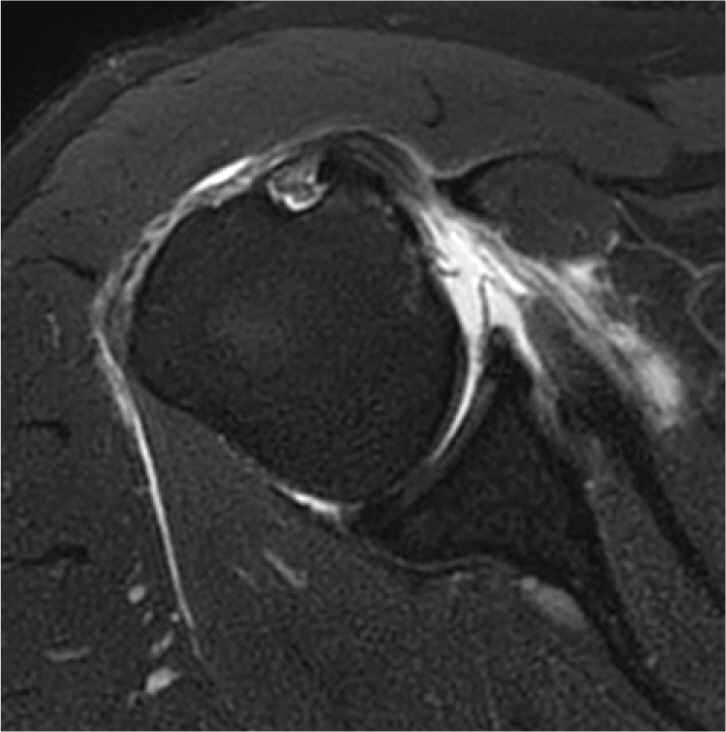
- Subscapularis
Fig. 9.
Oblique coronal fat-suppressed T2-weighted MRI scan. Fluid signal
intensity.
Subscapularis tendon tears are relatively difficult to detect using MRI.
These tears most commonly begin in the upper third of the tendon and tend to
progress caudally (Fig. 10) [32–34].
- Infraspinatus and teres minor
Fig. 10.
Oblique sagittal and axial fat-suppressed PD-weighted MRI scan.
Subscapularis full-thickness tear. Provided by the authors.
Infraspinatus tears typically occur alongside supraspinatus tendon tears,
with oblique coronal and sagittal fat-suppressed T2-weighted images being
the most effective for detection, similar to those used for the
supraspinatus tendon [35]. Isolated
tears of the infraspinatus have been reported to be rare [36].
In the case of the teres minor, tears are reported in only 0.9% of cases and
typically occur alongside tears in the supraspinatus and tears [37]. The integrity of these muscles is
best assessed using oblique sagittal fat-suppressed T2-weighted images
[38].
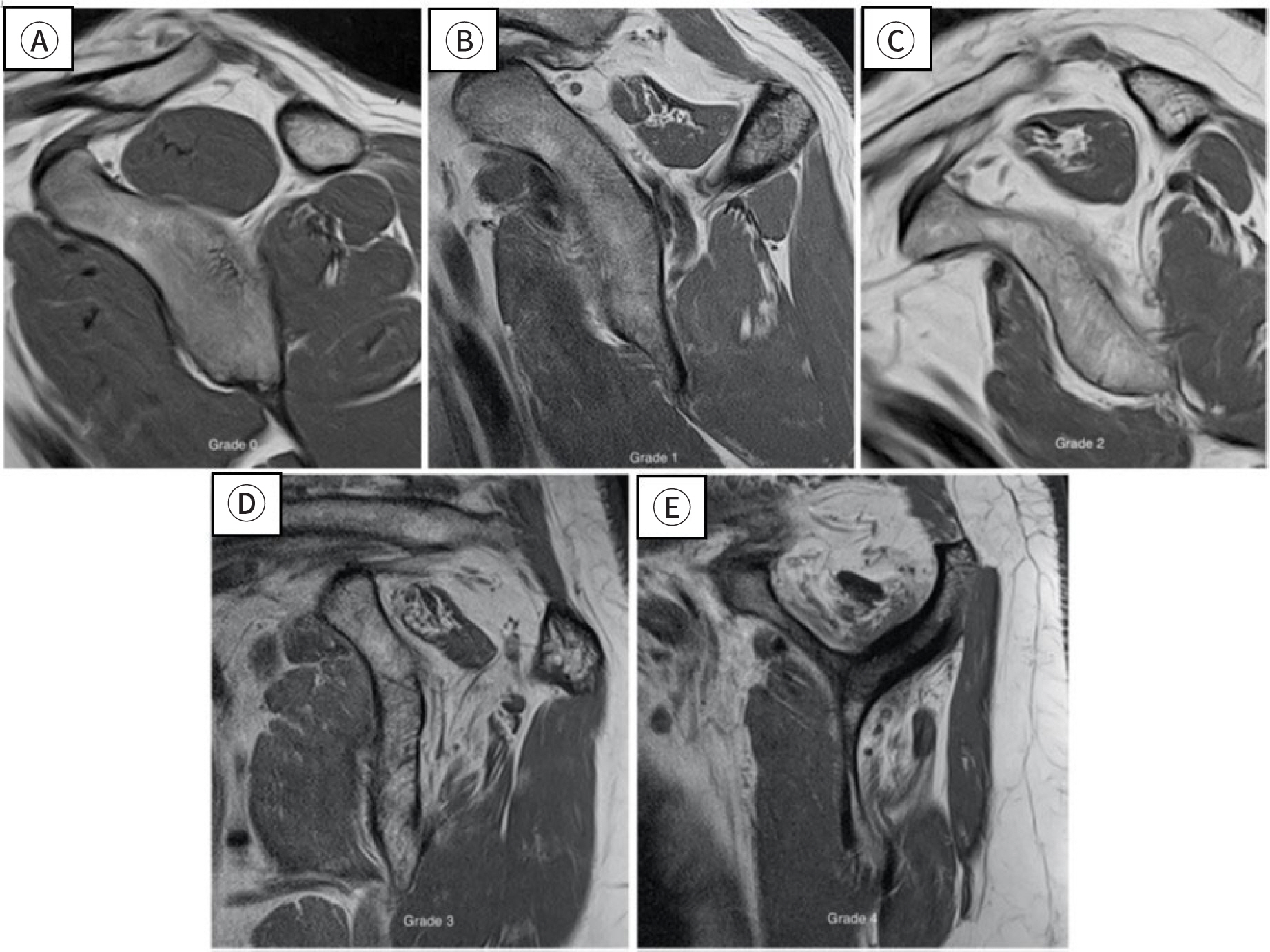
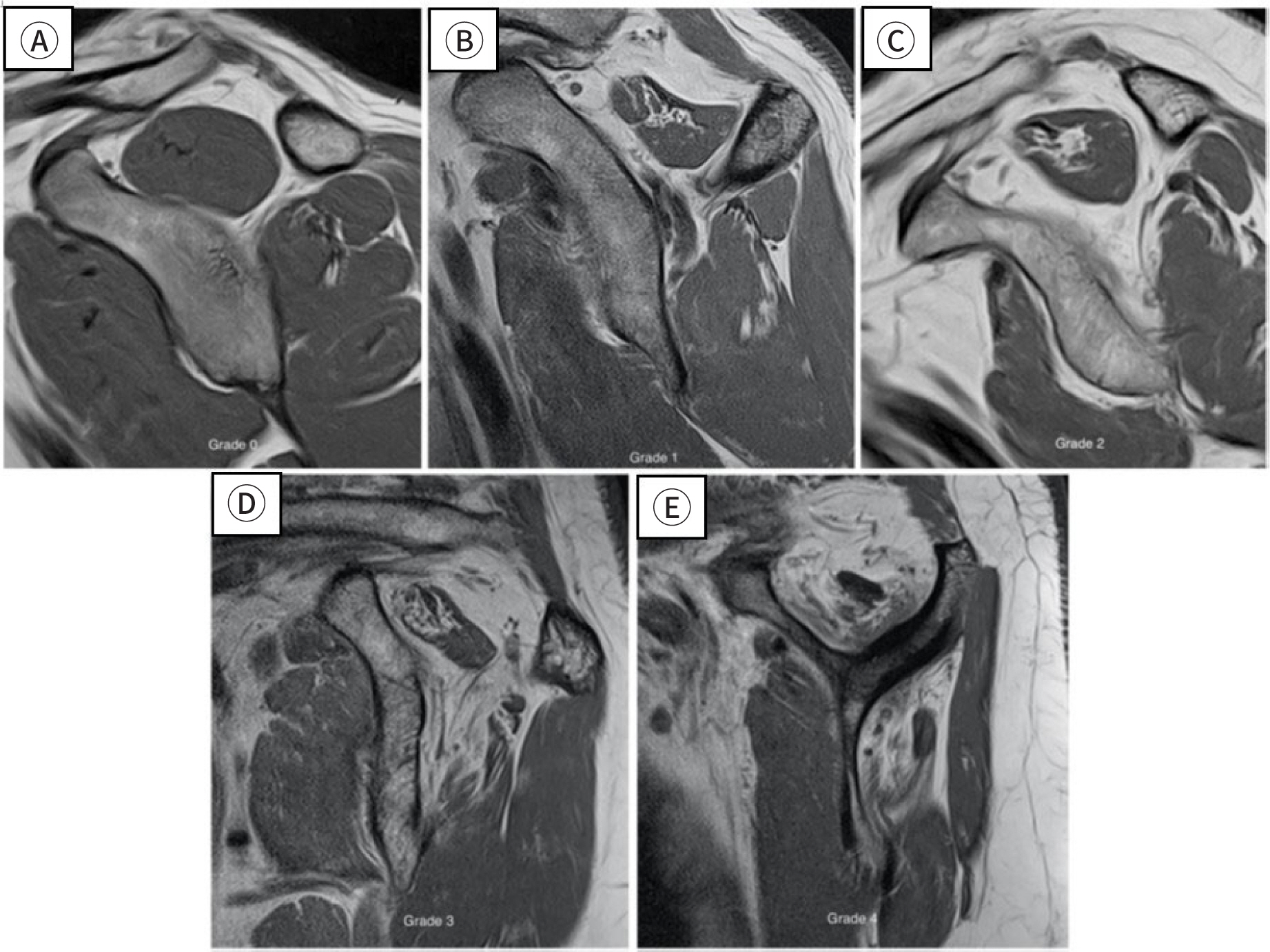
- Fatty infiltration of rotator cuff muscles
Fatty infiltration is characterized by a reduction in the elasticity of the
torn rotator cuff, resulting from lipid deposition in the muscle tissue of
chronic tears [39]. Therefore, fatty
infiltration in the rotator cuff muscles independently influences surgical
outcome [40]. The severity of this
condition can be classified based on the muscle signal observed in sagittal
oblique T1-weighted MRI scans (Table
1; Fig. 11) [41,42].
Table 1.
Goutallier classification
Grade
Muscle description
0
Normal
I
Some fatty streaks
II
Amount of muscle is greater than
fatty infiltration
III
Amount of muscle is equal to
fatty infiltration
IV
Amount of fatty infiltration is
greater than muscle
Fig. 11.
Fatty infiltration. Normal (A), grade I (B), grade II (C), grade
III (D), grade IV (E). Adapted from Yubran et al. [42] with CC-BY.
Osteoarthritis of the glenohumeral joint
Plain radiography
Plain radiography is often the initial imaging modality used, incorporating
anteroposterior (internal rotation), true anteroposterior (Grashey external
rotation), outlet, and axillary views. These views are essential for assessing
joint space narrowing, osteophytes, subchondral cysts, subchondral bone
irregularities, glenoid bone stock, and glenoid version [10].
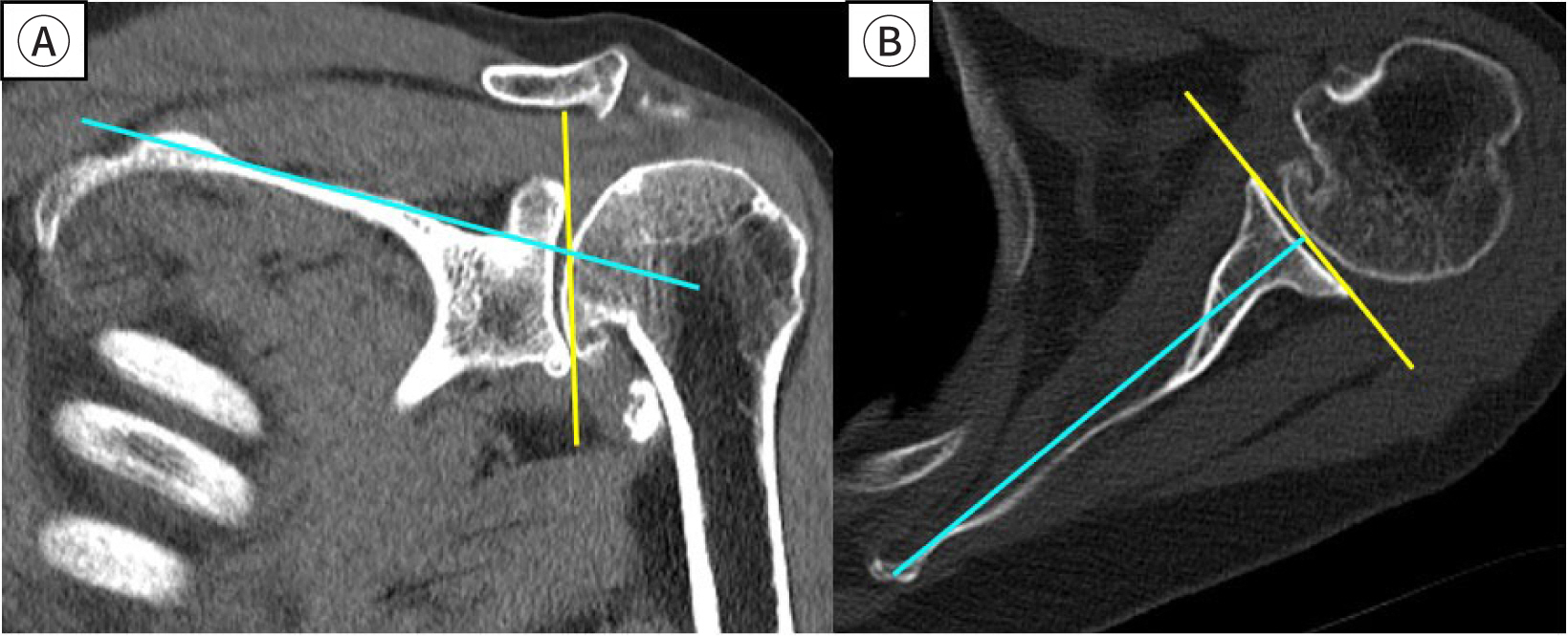
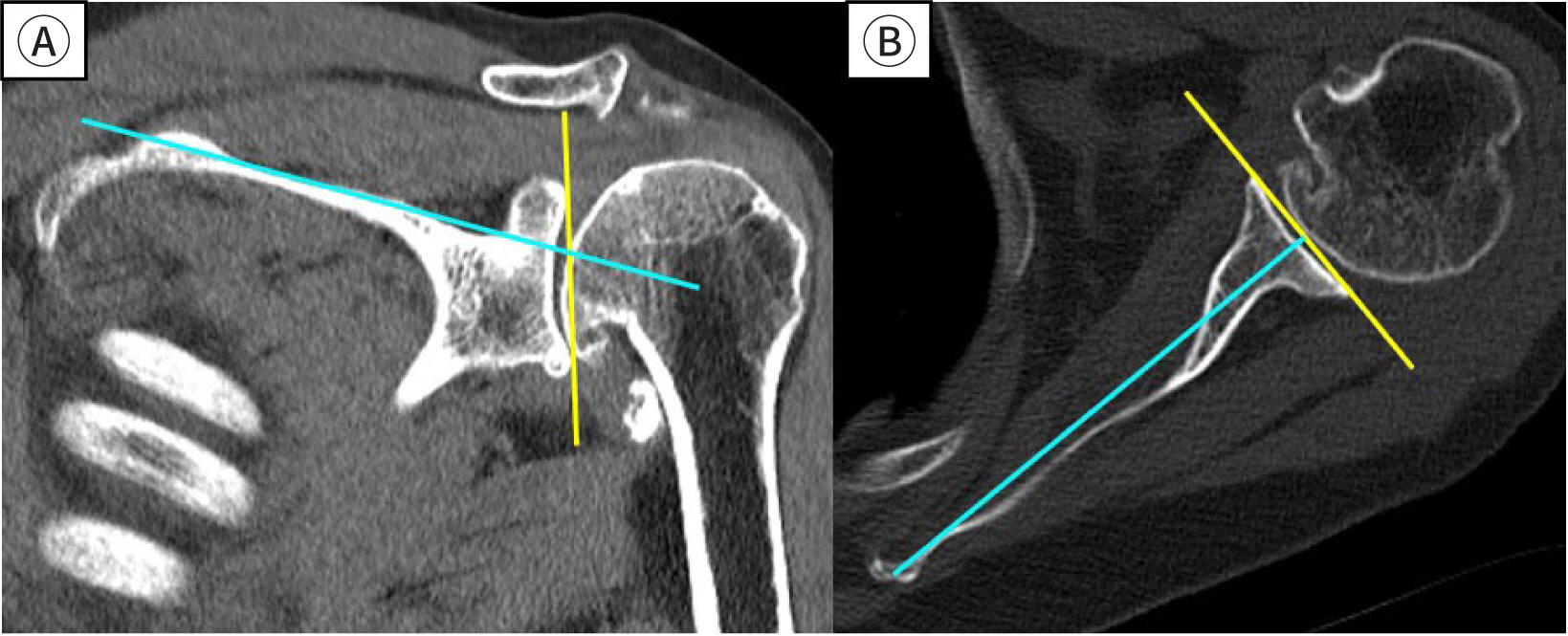
CT
Evaluating the precise bone stock of the glenoid—including bone loss,
version, and inclination—is challenging with plain radiography due to
overlapping structures. Therefore, CT is utilized for preoperative planning of
arthroplasty (Fig. 12) [43].
Fig. 12.
CT: glenoid inclination (A), glenoid version (B). Provided by the
authors.
Conclusion
To accurately diagnose and manage shoulder diseases in older adults, it is crucial to
evaluate the unique radiological features of each condition. This evaluation guides
the appropriate course of treatment, ranging from conservative approaches to
surgical interventions. Advanced diagnostic modalities, including MRI (or MRA),
known for their high sensitivity and specificity, are essential. Additionally,
ultrasonography is pivotal in identifying the radiological characteristics specific
to shoulder diseases in this patient group. Understanding the key findings in each
case of shoulder disease is vital for effective diagnosis and management.
Authors' contributions
Project administration: Kim MS
Conceptualization: Kim MS
Methodology & data curation: Kim MS, Jung TH
Funding acquisition: not applicable
Writing – original draft: Kim MS, Jung TH
Writing – review & editing: Kim MS, Jung TH
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Davis DL. Shoulder dysfunction and mobility limitation in
aging. Adv Geriatr Med Res 2023;5(3):e230008.
2. Davis DL, Sun K, Simonsick EM. Association of shoulder dysfunction with mobility limitation
among older adults in the Baltimore longitudinal study of
aging. Gerontol Geriatr Med 2023;9:23337214231179843
3. Sözlü U, Başar S, Kanatlı U. Scapular muscle endurance, shoulder pain, and functionality in
patients with rotator-cuff-related shoulder pain: a matched, case-control
study. Clin Shoulder Elb 2024;27(1):52-58.
4. Ko SH, Na SC, Kim MS. Risk factors of tear progression in symptomatic small to
medium-sized full-thickness rotator cuff tear: relationship between
occupation ratio of supraspinatus and work level. J Shoulder Elbow Surg 2023;32(3):565-572.
5. Picasso R, Pistoia F, Zaottini F, Marcenaro G, Miguel-Pérez M, Tagliafico AS, et al. Adhesive capsulitis of the shoulder: current concepts on the
diagnostic work-up and evidence-based protocol for radiological
evaluation. Diagnostics 2023;13(22):3410
7. Daher M, Lopez R, Covarrubias O, Boufadel P, Fares MY, Abboud JA. Sleep disturbances in rotator cuff pathology: insights into
mechanisms and clinical implications. Clin Shoulder Elb 2024;27(4):514-518.
8. MacConnell AE, Davis W, Burr R, Schneider A, Dugas LR, Joyce C, et al. An objective assessment of the impact of tendon retraction on
sleep efficiency in patients with full-thickness rotator cuff tears: a
prospective cohort study. Clin Shoulder Elb 2023;26(2):169-174.
9. Papalexis N, Parmeggiani A, Facchini G, Miceli M, Carbone G, Cavallo M, et al. Current concepts in the diagnosis and treatment of adhesive
capsulitis: role of diagnostic imaging and ultrasound-guided interventional
procedures. Radiol Med 2022;127(12):1390-1399.
10. Silva FD, Ramachandran S, Chhabra A. Glenohumeral osteoarthritis: what the surgeon needs from the
radiologist. Skeletal Radiol 2023;52(11):2283-2296.
11. Zappia M, Di Pietto F, Aliprandi A, Pozza S, De Petro P, Muda A, et al. Multi-modal imaging of adhesive capsulitis of the
shoulder. Insights Imaging 2016;7(3):365-371.
13. Al Khayyat SG, Falsetti P, Conticini E, Frediani B, Galletti S, Stella SM. Adhesive capsulitis and ultrasound diagnosis, an inseparable
pair: a novel review. J Ultrasound 2023;26(2):369-384.
14. Wu H, Tian H, Dong F, Liang W, Song D, Zeng J, et al. The role of grey-scale ultrasound in the diagnosis of adhesive
capsulitis of the shoulder: a systematic review and
meta-analysis. Med Ultrason 2020;22(3):305-312.
15. Tandon A, Dewan S, Bhatt S, Jain AK, Kumari R. Sonography in diagnosis of adhesive capsulitis of the shoulder: a
case–control study. J Ultrasound 2017;20(3):227-236.
16. Michelin P, Delarue Y, Duparc F, Dacher JN. Thickening of the inferior glenohumeral capsule: an ultrasound
sign for shoulder capsular contracture. Eur Radiol 2013;23(10):2802-2806.
17. Tue G, Masuzzo O, Tucci F, Cavallo M, Parmeggiani A, Vita F, et al. Can secondary adhesive capsulitis complicate calcific tendinitis
of the rotator cuff? An ultrasound imaging analysis. Clin Pract 2024;14(2):579-589.
18. Walmsley S, Osmotherly PG, Walker CJ, Rivett DA. Power Doppler ultrasonography in the early diagnosis of
primary/idiopathic adhesive capsulitis: an exploratory study. J Manip Physiol Ther 2013;36(7):428-435.
19. Suh CH, Yun SJ, Jin W, Lee SH, Park SY, Park JS, et al. Systematic review and meta-analysis of magnetic resonance imaging
features for diagnosis of adhesive capsulitis of the
shoulder. Eur Radiol 2019;29(2):566-577.
26. Zheng F, Wang H, Gong H, Fan H, Zhang K, Du L. Role of ultrasound in the detection of rotator-cuff syndrome: an
observational study. Med Sci Monit 2019;25:5856-5863.
27. Rutten MJCM, Jager GJ, Blickman JG. From the RSNA refresher courses: US of the rotator cuff:
pitfalls, limitations, and artifacts. Radiographics 2006;26(2):589-604.
31. Rafii M, Firooznia H, Sherman O, Minkoff J, Weinreb J, Golimbu C, et al. Rotator cuff lesions: signal patterns at MR
imaging. Radiology 1990;177(3):817-823.
32. Adams CR, Schoolfield JD, Burkhart SS. Accuracy of preoperative magnetic resonance imaging in predicting
a subscapularis tendon tear based on arthroscopy. Arthroscopy 2010;26(11):1427-1433.
33. Kim SC, Yoo SJ, Jo JH, Lee JH, Baek E, Lee SM, et al. The impact of supraspinatus tear on subscapularis muscle atrophy
and fatty infiltration. Clin Shoulder Elb 2024;27(4):437-446.
37. Melis B, DeFranco MJ, Lädermann A, Barthelemy R, Walch G. The teres minor muscle in rotator cuff tendon
tears. Skeletal Radiol 2011;40(10):1335-1344.
39. Mellado JM, Calmet J, Olona M, Esteve C, Camins A, Pérez del Palomar L, et al. Surgically repaired massive rotator cuff tears: MRI of tendon
integrity, muscle fatty degeneration, and muscle atrophy correlated with
intraoperative and clinical findings. AJR Am J Roentgenol 2005;184(5):1456-1463.
41. Fuchs B, Weishaupt D, Zanetti M, Hodler J, Gerber C. Fatty degeneration of the muscles of the rotator cuff: assessment
by computed tomography versus magnetic resonance imaging. J Shoulder Elbow Surg 1999;8(6):599-605.
43. Walch G, Moraga C, Young A, Castellanos-Rosas J. Results of anatomic nonconstrained prosthesis in primary
osteoarthritis with biconcave glenoid. J Shoulder Elbow Surg 2012;21(11):1526-1533.
Numerical simulation and structural optimization of automotive seat static comfort based on human-seat coupled model Haiwei Wang, Junfeng Liu, Zedong Tang, Helong Wu, Min Sun, Guang Zhang, Zheng Zhang Proceedings of the Institution of Mechanical Engineers, Part D: Journal of Automobile Engineering.2026;[Epub] CrossRef
Machine learning outperforms deep learning in adhesive capsulitis diagnosis: a clinical-radiomics model bridging PD-T2 MRI and multimodal data fusion Yang Yang, Ting Pan, Cong Zhang European Journal of Radiology.2025; 193: 112470. CrossRef
Radiological characteristics of shoulder diseases in older adults,
including adhesive capsulitis, rotator cuff tear, and osteoarthritis of the
glenohumeral joint: a narrative review
Fig. 1.
Ultrasonography. Thickened coracohumeral ligament, oblique transverse
image (A), short axis image (B). Adapted from Picasso et al. [5] with CC-BY.
Fig. 2.
Ultrasonography. Thickened inferior glenohumeral capsule,
longitudinal image. Adapted from Picasso et al. [5] with CC-BY.
Fig. 3.
Ultrasonography, oblique axial section. Thickened axillary pouch (A),
normal axillary pouch (B). Adapted from Tue et al. [17] with CC-BY.
Fig. 4.
Protocol for imaging evaluation using ultrasonography in patients
with adhesive capsulitis. Adapted from Picasso et al. [5] with CC-BY.
Fig. 5.
Sagittal T1 and T2-weighted MRI scan. Fat obliteration (arrow),
thickened and hyperintensity of the anteroinferior capsule (outlined
arrowhead; A,B). Adapted from Picasso et al. [5] with CC-BY. SS, supraspinatus; Ac, acromion; CI,
clavicle; Co, coracoid process; Sub, subscapularis; HH, humeral
head.
Fig. 6.
Plain image. True anteroposterior view (A), outlet view (B) and
axillary view (C). Provided by the authors.
Fig. 7.
Longitudinal plane ultrasound image of supraspinatus tendon. Anechoic
gap and pitting due to tear. Provided by the authors.
Fig. 8.
Oblique coronal fat-suppressed T2-weighted MRI scan. Abnormal
high signal and focal swelling of the supraspinatus tendon. Provided
by the authors.
Fig. 10.
Oblique sagittal and axial fat-suppressed PD-weighted MRI scan.
Subscapularis full-thickness tear. Provided by the authors.
Fig. 11.
Fatty infiltration. Normal (A), grade I (B), grade II (C), grade
III (D), grade IV (E). Adapted from Yubran et al. [42] with CC-BY.
Fig. 12.
CT: glenoid inclination (A), glenoid version (B). Provided by the
authors.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Fig. 7.
Fig. 8.
Fig. 9.
Fig. 10.
Fig. 11.
Fig. 12.
Radiological characteristics of shoulder diseases in older adults,
including adhesive capsulitis, rotator cuff tear, and osteoarthritis of the
glenohumeral joint: a narrative review
Goutallier classification
Grade
Muscle description
0
Normal
I
Some fatty streaks
II
Amount of muscle is greater than
fatty infiltration
III
Amount of muscle is equal to
fatty infiltration
IV
Amount of fatty infiltration is
greater than muscle