1Department of Orthopaedic Surgery, Chungbuk National University Hospital, Cheongju, Korea
*Corresponding author: Ho-Seung Jeong,
Department of Orthopaedic Surgery, Chungbuk National University Hospital, 776,
1sunhwan-ro, Seowon-gu, Cheongju 28644, Korea, E-mail:
turbox2@hanmail.net
• Received: November 15, 2024 • Revised: December 26, 2024 • Accepted: January 1, 2025
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
The purpose of this review is to provide a comprehensive guide for managing older
adult patients with shoulder diseases, specifically rotator cuff tears and
osteoarthritis, and to explore effective nonsurgical treatment options. Chronic
rotator cuff tears are typically degenerative, whereas acute tears result from
trauma. A key feature of these tears is tendon degeneration accompanied by type
III collagen predominance, predisposing tears to progression. Osteoarthritis in
the glenohumeral joint arises from wear-and-tear changes that compromise
cartilage integrity, leading to pain and restricted motion. Accurate clinical
assessment and imaging, including plain radiographs, ultrasonography, and MRI,
facilitate diagnosis and guide treatment. The physic-al examination emphasizes
range of motion, rotator cuff strength, and scapular stability. Management
strategies prioritize pain relief, function preservation, and improving
mobility. Nonsurgical modalities, including exercise, manual therapy, and
activity modification, constitute first-line treatments, especially for older
adults. Pharmacological approaches involve NSAIDs, corticosteroid injections,
and neuropathic pain medications. Steroid injections have short-term benefits,
but repeated treatments may compromise tissue integrity. Platelet-rich plasma is
a regenerative option that may improve tendon healing, but mixed findings
highlight the need for further investigation. A structured physical therapy
program focusing on range of motion and strengthening is essential, with
alternative interventions used judiciously. Patients should be counseled
regarding the potential progression of tears and the possible need for future
surgical intervention if nonsurgical methods are unsuccessful. Multimodal
approaches, including joint mobilization and personalized exercise regimens,
hold potential for optimizing functional outcomes and supporting independence in
older adults.
Shoulder pain is a prevalent issue among older adults, affecting approximately
25% to 30% of this population and leading to significant symptoms and disability
[1]. This condition imposes a
considerable burden on both function and quality of life, yet it is frequently
overlooked and, as a result, undertreated [1]. Emphasizing treatment is crucial, particularly for older adults
with persistent shoulder pain, as maintaining independence is a key concern. The
loss of function in the dominant upper limb can severely impact daily activities
such as grooming, cooking, and driving. Moreover, shoulder pain or muscle
weakness around the shoulder can complicate the use of assistive devices like
walkers [2,3]. Thus, it is vital to implement effective treatment strategies to
minimize pain and preserve or restore function as much as possible. However, in
older adults, shoulder pain and the disabilities it causes are often dismissed
as inevitable aspects of aging or are seen as issues that must be endured,
leading to inadequate treatment [3].
Neither older age nor the presence of comorbidities should deter the pursuit of
active treatment and rehabilitation.
Objectives
This article provides a guide for approaching older adult patients with shoulder
diseases, specifically focusing on rotator cuff tears (RCTs) and osteoarthritis,
and explores effective nonsurgical treatment options.
Ethics statement
As this study is a literature review, it did not require institutional review board
approval or individual consent.
Rotator cuff injury
Anatomy
The rotator cuff comprises four muscle-tendon structures: the supraspinatus,
infraspinatus, subscapularis, and teres minor. The supraspinatus and
infraspinatus originate from their respective fossae on the posterior surface of
the scapula and insert into the greater tuberosity of the proximal humerus. The
supraspinatus, forming the superior aspect of the cuff, is primarily responsible
for initiating abduction at the glenohumeral joint (GHJ). In contrast, the
infraspinatus, along with the teres minor, facilitates external rotation of the
GHJ [4,5]. The subscapularis, the largest of the cuff muscles, is tasked
with internal rotation of the GHJ [4]. It
originates from the anterior surface of the scapula and inserts into the lesser
tuberosity of the humerus. The teres minor, arising from the middle third of the
lateral border of the scapula, also inserts into the greater tuberosity, aiding
in external rotation [5].
Etiology
RCTs can be categorized as acute or chronic, and as partial or full thickness.
Acute RCTs typically occur in younger patients due to traumatic events such as
falls or dislocations. In contrast, chronic RCTs develop in older adults and
result from age-related degenerative processes. This article focuses on chronic
RCTs.
The pathogenesis of RCTs in older adults is complex and multifactorial, involving
degenerative processes associated with aging, impingement, and trauma. During
tendon degeneration, there is a significant shift in collagen composition,
notably an increase in type III collagen. This type of collagen forms thin,
reticular fibers that are more susceptible to lesions, especially when compared
to the sturdier type I collagen [6,7]. The degree of tendon degeneration can
vary widely depending on the location of degradation and the condition of the
tendon, with the supraspinatus tendon typically showing more pronounced
degeneration. Tendon degeneration is a physiological process that occurs with
aging and is closely linked to the individual's age [7,8].
Additionally, increasing age is associated with higher rates of retears [9].
Typically, RCTs begin as partial-thickness tears and gradually expand due to both
intrinsic and extrinsic factors, eventually resulting in a complete tear. The
fibers that are initially torn are unable to contribute to load distribution,
causing the remaining fibers to further propagate the tear. This process is
particularly pronounced in older adults, as the tendon quality is already
compromised [10]. As the force required
to move the arm increases, it exacerbates the tear, thereby compromising joint
biomechanics. A full-thickness tear can cause significant chronic pathological
changes, including muscle atrophy, fatty infiltration, and scapular contracture,
which may lead to GHJ osteoarthritis [11].
Physical examination
The patient should initially be dressed in a gown that exposes the entire back
and shoulder girdle for evaluation. All physical examination maneuvers must be
compared with the opposite extremity. The physician should conduct a
comprehensive shoulder examination, starting with a general inspection of the
patient in a resting position to check for any signs of muscle wasting.
Palpation should cover the entire shoulder girdle to identify any tender areas.
Rotator cuff injuries frequently manifest as tenderness at Codman’s
point, which is identified by rotating the proximal end of the humerus beneath
the examiner’s finger at the anterior corner of the acromion [12].
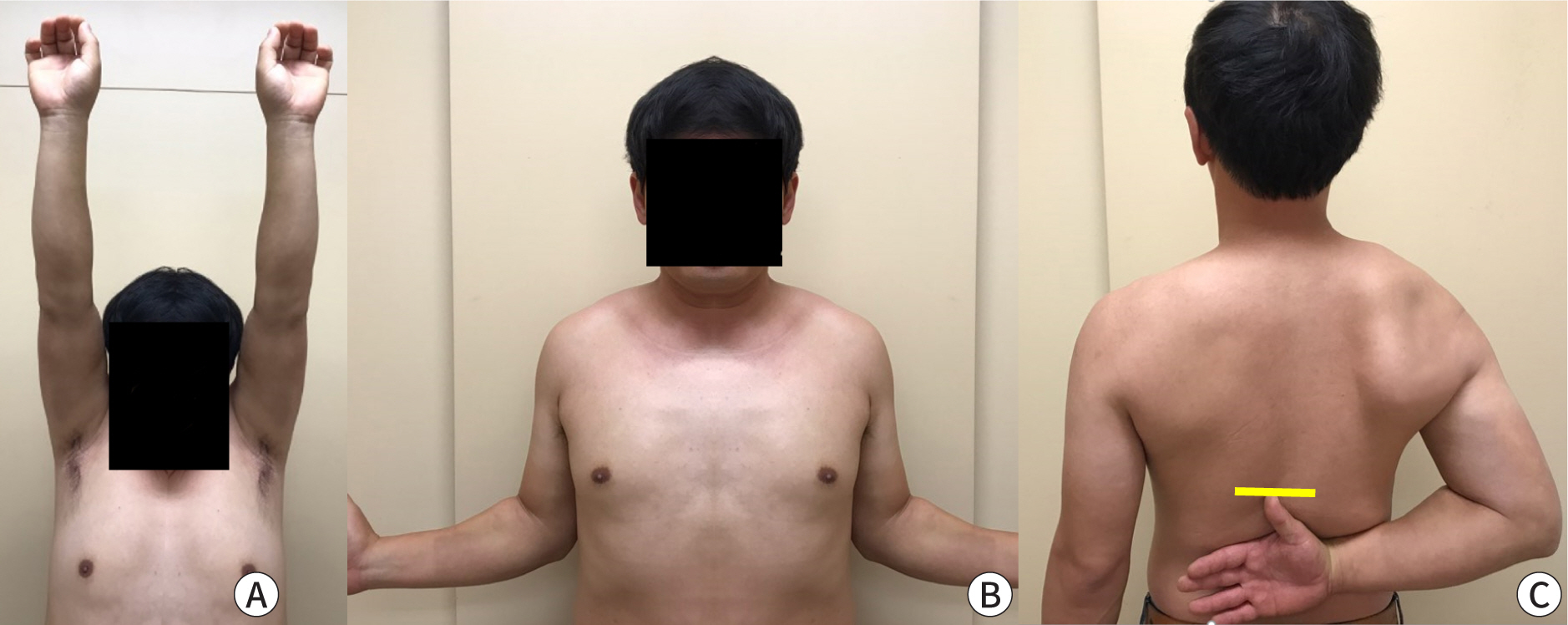
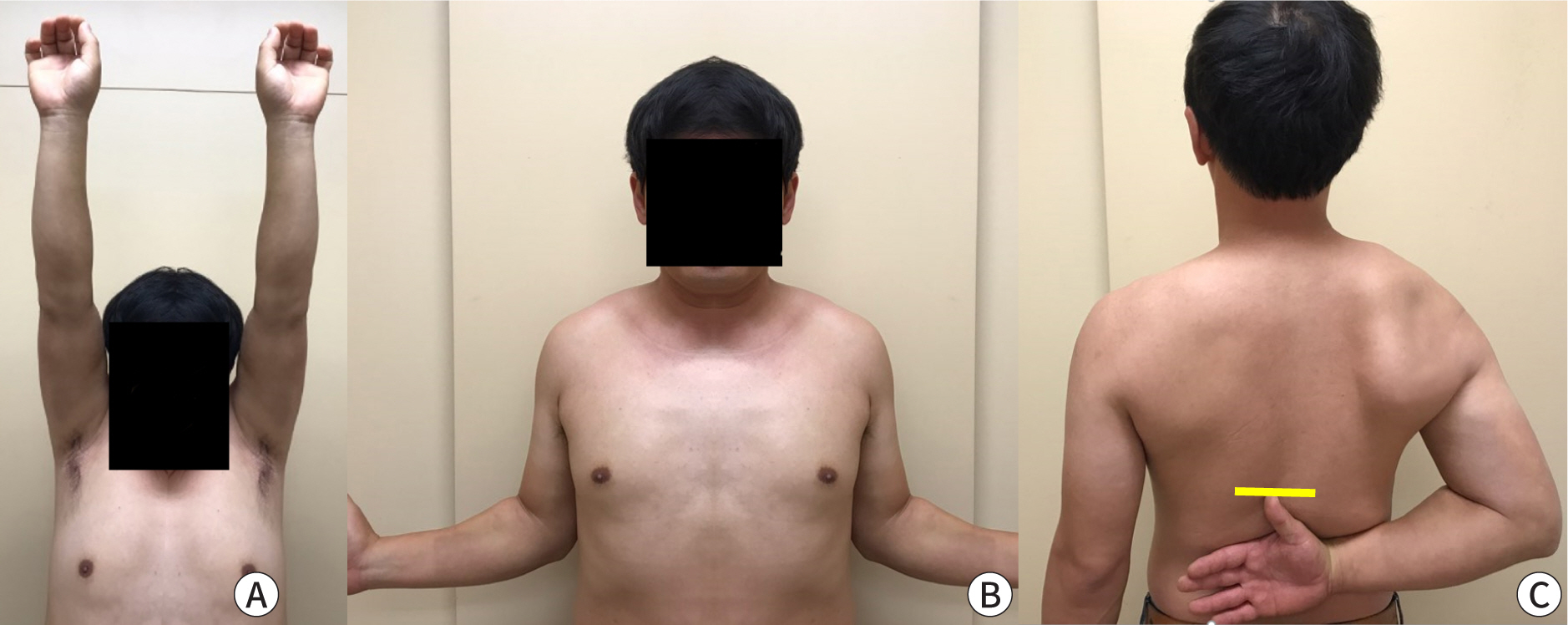
Both active and passive shoulder range of motion should be assessed. Forward
elevation is evaluated by observing the patient from the side; it is measured as
the angle between the axis of the scapula and a line extending from the shoulder
to the elbow. External rotation is assessed with the elbow close to the side,
rotating the forearm laterally. Internal rotation is measured by having the
patient reach up their back, noting the highest spinal segments reached (Fig. 1). Both external and internal rotations
can also be measured with the arm abducted to 90 degrees. Abduction is tested in
the scapular plane, and it is possible to isolate glenohumeral motion from
scapulothoracic motion by stabilizing the scapula. In patients suspected of
having a supraspinatus tear, forward shoulder elevation may be weak. In cases of
larger posterior superior tears involving both the infraspinatus and
supraspinatus muscles, external rotation and forward elevation are typically
weak. In the case of anterior or subscapularis tears, internal rotation may be
compromised.
Fig. 1.
The active range of motion is assessed by forward elevation (A),
external rotation with the elbow at the side of the body (B), and the
internal rotation angle is usually assessed by the height of the
vertebral body (yellow line) from behind (C). Provided by the authors
after consent of the examinee.
Radiological imaging
Initial evaluation of a patient with shoulder pain and dysfunction should always
include a complete set of plain radiographs of the shoulder. These are essential
for assessing potential causes of pain and for evaluating conditions such as
osteoarthritis, superior migration of the humeral head, avascular necrosis,
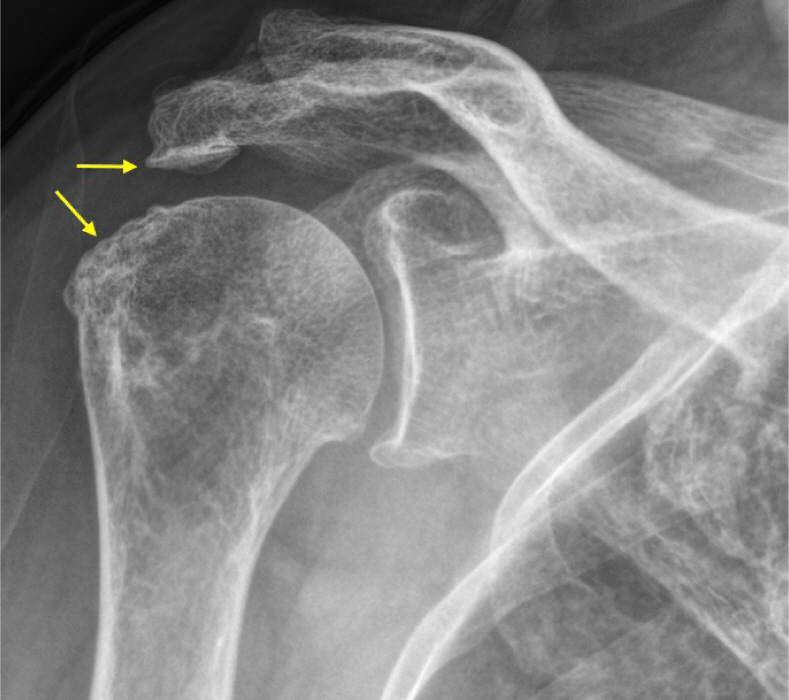
osteoporosis, or tumors (Fig. 2). A
supraspinatus outlet view may be particularly useful for visualizing bony
structures involved in scapulohumeral motions, such as bony spurs or ligamentous
calcifications that could impinge on the underlying rotator cuff. An axillary
view is beneficial for ruling out shoulder dislocation in cases of trauma. The
rotator cuff can be examined using ultrasonography (US) or MRI. US is
cost-effective and allows for real-time examination of the shoulder joint by the
physician. It can determine the size and location of tears, although the results
are highly subjective and depend on the operator [10]. A study found that preoperative US identified mixed
hyperechoic and hypoechoic foci in the supraspinatus tendon with a sensitivity
of 93%, a specificity of 94%, a positive predictive value of 82%, and a negative
predictive value of 98%. MRI is considered the gold standard for imaging the
rotator cuff tendons [13]. It provides a
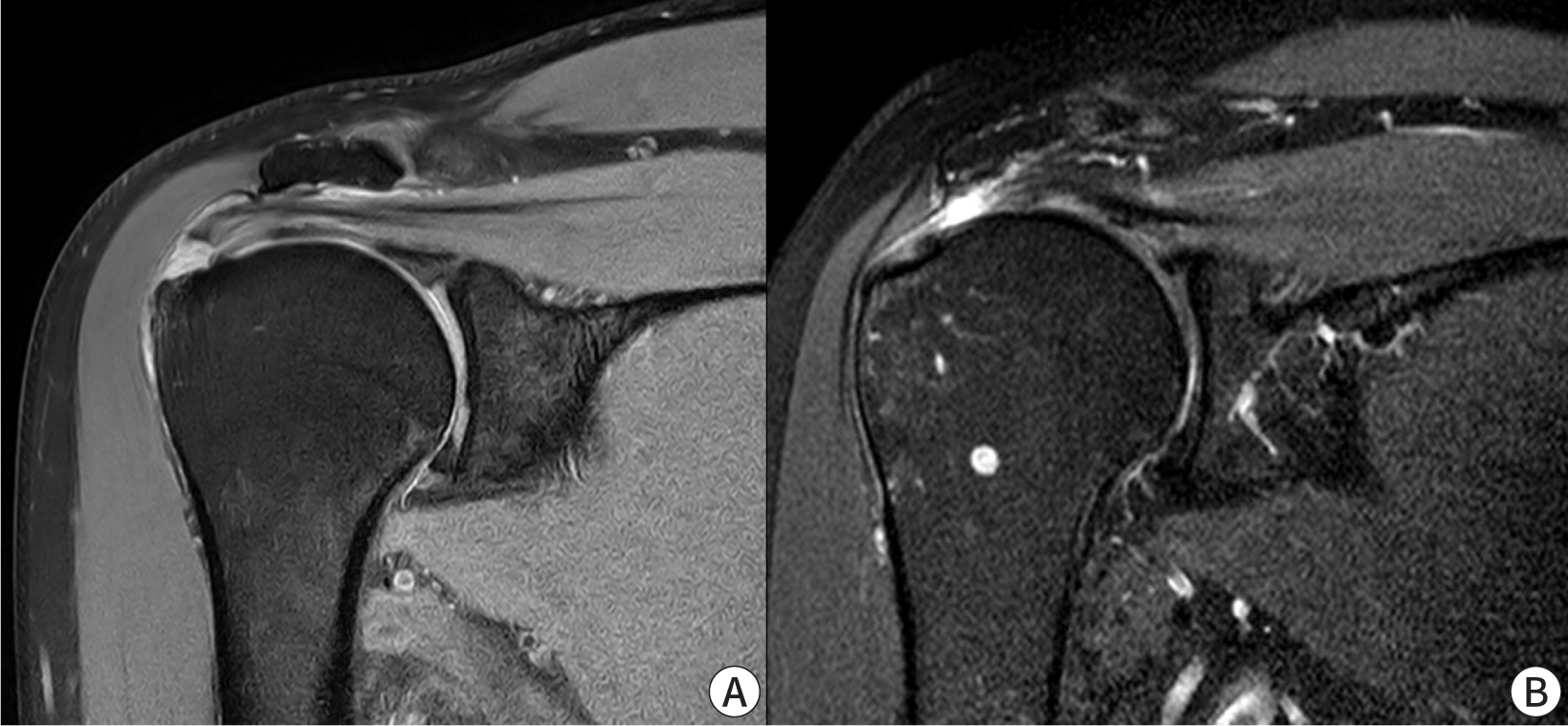
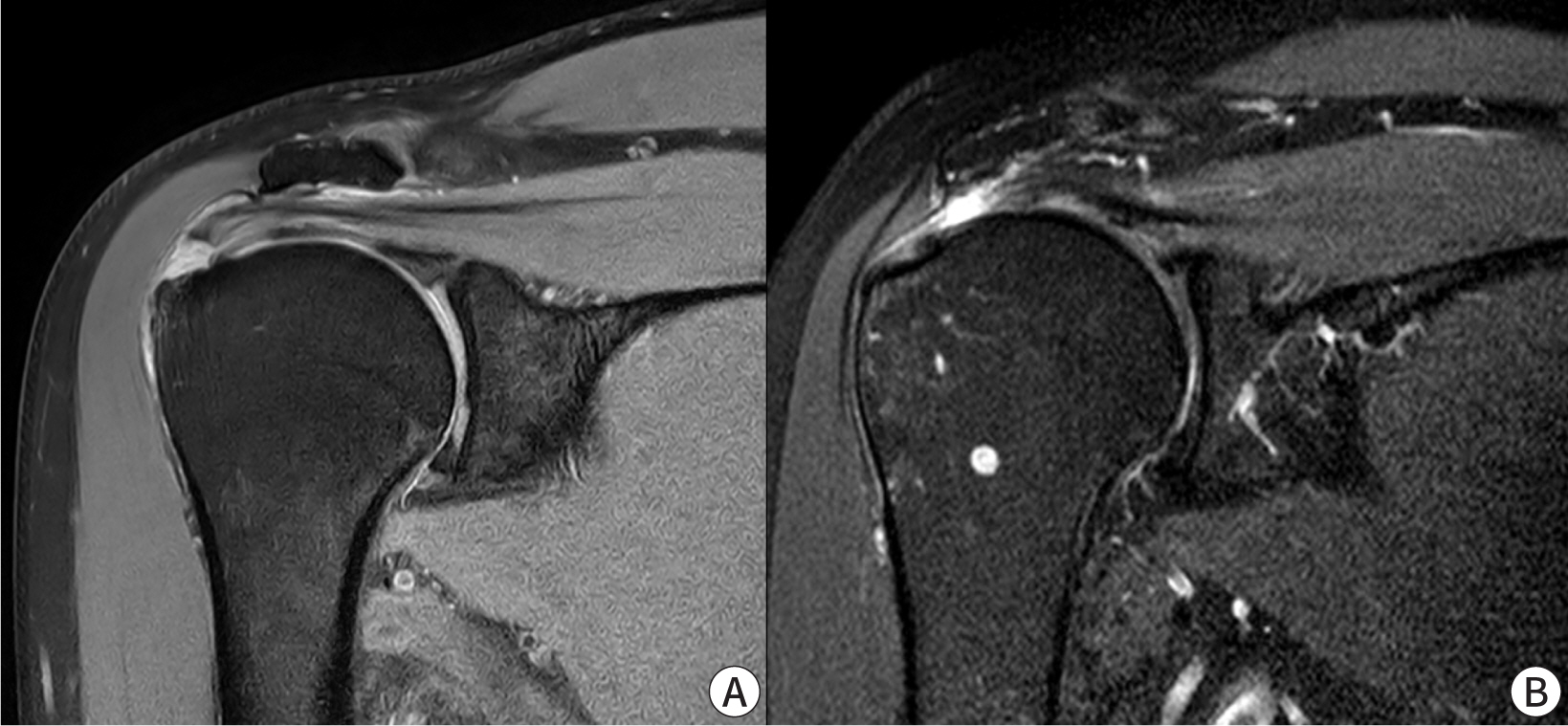
comprehensive assessment of the entire rotator cuff musculotendinous unit (Fig. 3). The presence of muscle atrophy and
fatty infiltration can indicate the chronicity of tears, aiding in treatment
decisions. Another study showed that MRI and US have similar diagnostic accuracy
for detecting full-thickness RCTs. However, it noted that US had lower
sensitivity than MRI in evaluating partial-thickness tears [14]. A diagnosis of partial-thickness tears
is made when there is no evidence of tendon discontinuity on T1-weighted images,
and MRI shows an increased signal in the rotator cuff. A partial-thickness RCT
appears as an increased signal on T2-weighted images with a focal defect that is
either intra-tendinous or limited to one surface and does not extend through the
entire tendon. Rotator cuff tendinitis may cause increased rotator cuff signal
and reduced anatomical definition on T1-weighted and proton density images,
similar to the appearance of partial-thickness RCT. However, tendinitis is
differentiated from partial-thickness RCT by the presence of only moderate or
decreased signal on T2-weighted images [15].
Fig. 2.
The presence of osteophytes on the greater tuberosity and acromion of
the humerus indicates that there is a high possibility of a rotator cuff
tear. Provided by the authors.
Fig. 3.
Magnetic resonance images show a partial tear of the supraspinatus
tendon (A), and a complete tear of the supraspinatus tendon (B).
Provided by the authors.
Treatment
The goal of treatment is to restore normal shoulder function and biomechanics and
to improve functional ability. The success of nonsurgical treatment for RCTs
often depends on the size of the tear and the patient’s level of
activity. Generally, the more active the patient and the larger the tear, the
greater the likelihood that surgical intervention will be necessary [16]. In cases of acute RCTs, it is
important to initially administer short-term anti-inflammatory medications,
coupled with a few days of relative rest and activity modification.
Additionally, light exercise during this period is essential to maintain joint
range and prevent adhesions. Once the inflammation has subsided and the pain is
somewhat managed, it is important to promptly start an exercise program. This
program should focus on strengthening the muscles of the internal and external
rotators, as well as those around the scapula, and should be implemented
swiftly. Such exercise programs can positively impact clinical outcomes, even if
surgery becomes necessary later [16].
Patients opting for nonsurgical treatment should be informed that while this
approach may alleviate symptoms and enhance function, it does not repair the
tear [6]. It is also important to convey
that tears initially deemed reparable may become irreparable over time.
Furthermore, the outcomes of surgery following unsuccessful non-operative
treatment may be less favorable than those of primary repair [10].
Exercise and manual therapy
Exercise and manual therapy guided by a physical therapist represent the most
commonly chosen initial treatment for older adult patients with RCTs [17]. A well-structured physical therapy
regimen should include re-education of muscle recruitment, scapular
stabilization, coordination of muscle contractions, and enhancement of
proprioception [10]. Once
inflammation and pain have subsided, a specialized physical therapy program
should be initiated, aimed at eliminating capsular contracture and restoring
full range of motion. As range of motion improves, the focus should shift to
strengthening the rotator cuff and periscapular musculature. The role of the
rotator cuff in dynamically stabilizing the shoulder joint is maximized
through progressive resistive exercises using elastic bands or free weights.
Numerous studies have reported that exercise protocols effectively provide
pain relief and satisfaction for the majority of older adult patients with
RCTs [18–20]. However, functional outcomes may be superior with
surgical repair in cases of smaller tears that are amenable to surgery
[20].
Corticosteroid injections
Corticosteroid injections are commonly utilized to treat tendon pathology due
to their potent anti-inflammatory properties. Numerous studies have
suggested that these injections can enhance pain scores and functional
outcomes [21,22]. However, caution is advised when using these
injections repeatedly, as they may compromise the internal structural
integrity of the tendon. A systematic review indicated that subacromial
corticosteroid injections provide only short-term pain relief and are
ineffective in the comprehensive management of RCTs [23]. Another systematic review on the use of
corticosteroid injections for RCTs concluded that corticosteroid injections
are not efficacious [24]. Although no
studies have specifically targeted the older adult population, a prospective
randomized study involving patients with a mean age of 62 years found that
62.5% of those who received steroid injections were dissatisfied and
ultimately opted for surgery. Consequently, the evidence supporting the use
of corticosteroids in managing RCTs is limited, suggesting their role may be
confined to short-term pain management. Additionally, corticosteroid
injections are associated with risks such as joint infection, tendon
weakening, localized bruising, and a mild increase in blood sugar levels.
Therefore, corticosteroid injections may be considered as a treatment option
to alleviate pain, thereby facilitating physiotherapy.
Platelet-rich plasma injections
Platelet-rich plasma (PRP) is an autologous blood product that contains
platelets in supraphysiological concentrations, which can activate various
growth factors involved in tissue repair processes [25]. It possesses anti-nociceptive, anti-inflammatory,
and regenerative properties [26].
Additionally, in vitro studies of tenocytes from
degenerative RCTs have demonstrated that PRP increases cell proliferation
and extracellular matrix synthesis [27,28]. However, clinical
studies on PRP injections for RCTs have yielded mixed results. A systematic
review reported that PRP injections were associated with better pain relief
and functional outcomes compared to control interventions [29]. Two studies have explored the
effects of PRP on healing after surgical repair in RCTs, but they have not
conclusively shown clear clinical benefits [30,31]. Prospective
randomized clinical trials comparing PRP to saline injections have indicated
that PRP was no more effective than a placebo in improving quality of life,
pain, disability, and shoulder range of motion. In contrast, another
randomized prospective study found that PRP yielded superior results in
terms of pain, function, and range of motion compared to dry needling [32]. A systematic review highlighted
that the evidence regarding the optimal site for PRP injection in partial
thickness RCTs remains unclear. PRP has shown improvements in functional
outcomes for patients with partial thickness RCTs, regardless of the
injection site. However, further research is necessary to determine the
optimal concentration, injection frequency, and candidate selection for PRP
therapy [33].
Osteoarthritis
Anatomy and etiology
The GHJ is structurally a ball-and-socket joint and functionally considered a
diarthrodial, multiaxial joint. The glenohumeral articulation involves the
humeral head and the glenoid cavity of the scapula, representing the primary
articulation of the shoulder girdle. Normally, the articular surfaces of the GHJ
are concentric, smooth, and securely bonded to the underlying bone. However, if
the glenoid concavity is compromised, stabilization of the humeral head is lost.
In an arthritic GHJ, the smooth, concentric joint surfaces deteriorate due to
damage to the articular cartilage and the underlying bone. A review article
noted that in cases of osteoarthritis, glenoid retroversion increased from
8° to 11° [34].
Degenerative joint disease, a common form of glenohumeral arthritis, occurs when
the articular cartilage deteriorates due to heavy use, cumulative minor
traumatic episodes, underlying structural defects in the joint, anomalies in
cartilage composition, or a combination of these factors. Osteoarthritis, the
most prevalent joint disease, is a non-inflammatory condition characterized by
the weakening and deformation of joint cartilage, leading to abnormal bone
formation on and around the joint surface. Osteoarthritis represents both a
mechanical and biological phenomenon that arises when the normal processes of
degeneration and formation of articular cartilage and subchondral bone fail.
Although the causes are varied, it ultimately impacts all tissues of the movable
joint, leading to joint dysfunction [35].
The majority of osteoarthritis cases in the GHJ are linked to non-specific
factors, primarily advancing age, while specific risk factors are more commonly
observed in younger patients [35].
Physical examination
The diagnosis of shoulder osteoarthritis is based on a combination of specific
symptoms, physical examination findings, and radiographic evidence of changes to
the bone. The most common initial symptom is a progressive, activity-related
pain that is deep within the joint and often localized to the posterior aspect.
As the condition worsens, patients frequently experience pain at night. For
many, this pain is also present at rest and disrupts sleep [36]. The examination process starts by
identifying which movements the patient finds most problematic. Understanding
these limitations helps in determining potential treatment options. The
evaluation then proceeds with a thorough assessment of shoulder mobility. This
includes testing forward elevation, abduction, external rotation, external
rotation in abduction, internal rotation, internal rotation in abduction, and
cross-body adduction. These tests evaluate the range of motion of the humerus
relative to the thorax. For a more detailed assessment of glenohumeral motion,
the examiner can stabilize the scapula with one hand while using the other to
assess flexion, extension, and internal and external rotation of the humerus
relative to the scapula. Demonstrating the difference in motion between the
affected shoulder and the contralateral, normal or less affected shoulder can be
informative for both the patient and family members.
Muscle strength in the shoulder girdle muscles is assessed using manual muscle
testing [37]. However, this method is
subject to inter-observer variability. Hand-held dynamometers provide clinicians
with a valuable tool for quantitatively assessing muscle strength and validating
the effects of interventions. Previous studies have introduced reliable clinical
assessment methods for scapular motion, which are categorized into visual
observation and objective assessment. Changes in scapular position and motion
patterns are referred to as "scapular dyskinesis" [38]. The current guideline for assessing
scapular dyskinesis clinically is to employ the dynamic scapular dyskinesis test
[38]. Objective assessments of
scapular position and motion utilize a digital inclinometer. To evaluate
scapular upward rotation, the angle of inclination measured along the scapular
spine with the digital inclinometer is recorded.
Radiological imaging
Shoulder imaging is crucial for confirming diagnoses, assessing the severity of
pathological changes, aiding in surgical planning, and enhancing patient
comprehension of their condition. Standard plain films are vital for evaluating
patients with shoulder arthritis. Employing proper radiographic techniques is
essential to capture the necessary images for effective treatment planning
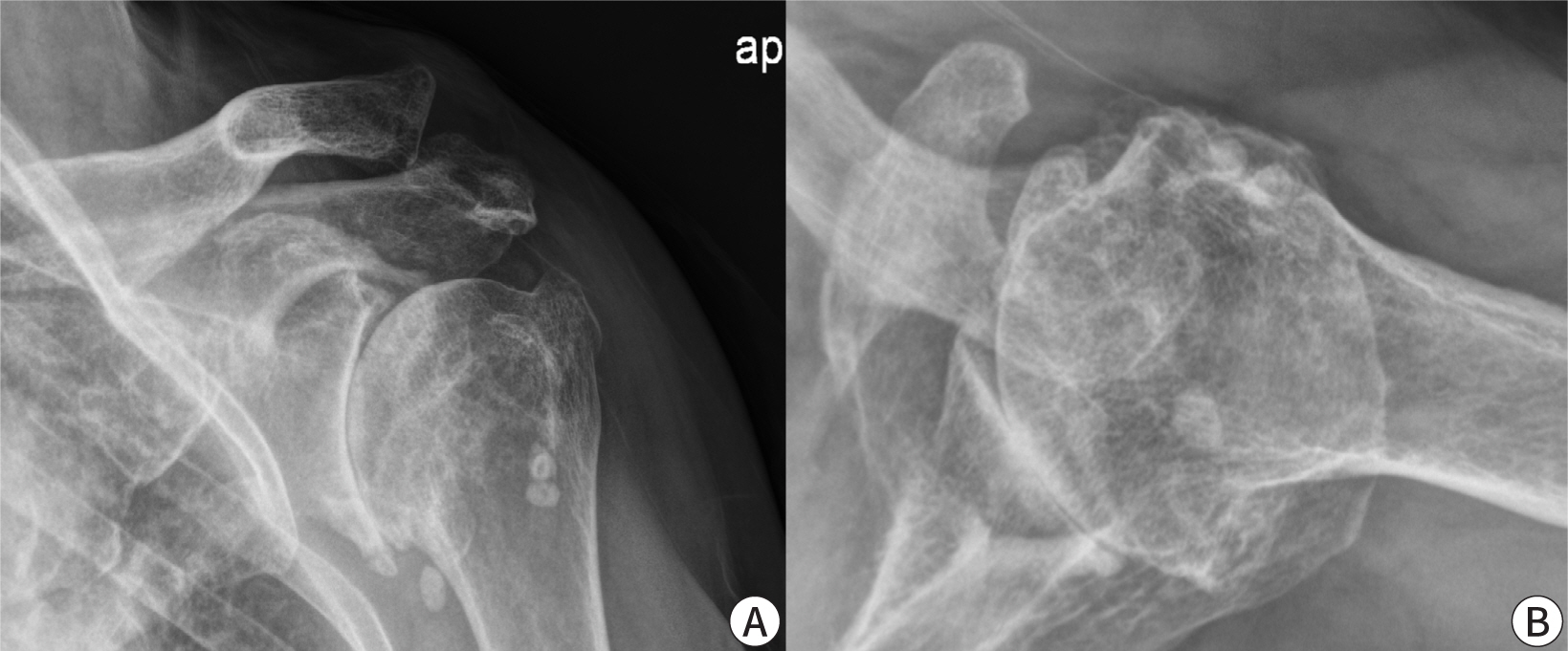
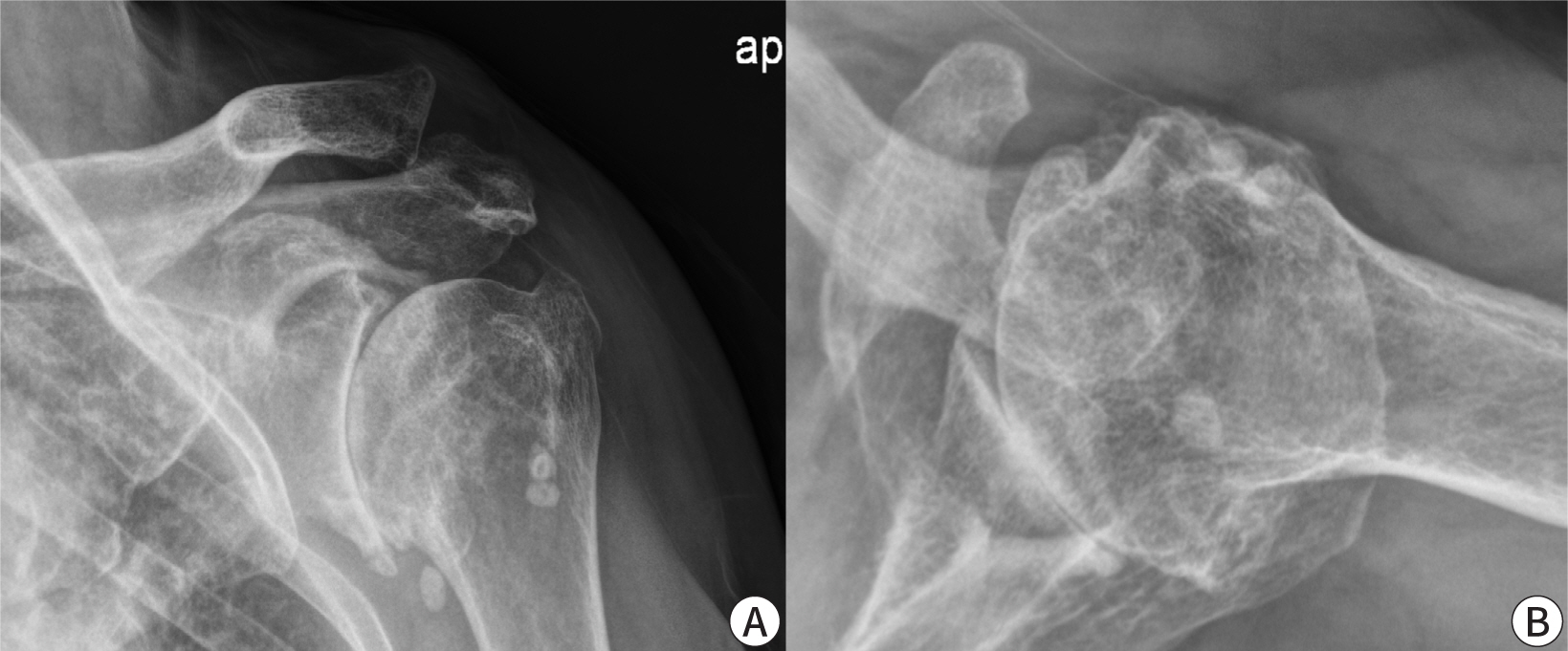
(Fig. 4).
Fig. 4.
Anteroposterior and axillary-lateral plain X-ray images of
osteoarthritis of the shoulder joint show narrowing of the joint space
and formation of osteophytes. Provided by the authors.
The first image is an anteroposterior view captured with the X-ray beam directed
through the GHJ in the scapular plane. This perspective reveals the
superior-inferior positioning of the scapula, the presence of osteophytes on the
scapular head and scapula, joint space narrowing, the extent of medial
displacement of the humerus relative to the lateral acromion line, the condition
of the humerus and scapula, the presence of loose bodies, and any collapse or
deformity of the humeral head [39].
The second image is an axillary view captured with the arm functionally elevated
in the scapular plane, oriented to display both the scapular notch and the
scapular neck. This perspective offers a distinct visualization of the humeral
anatomy, the quantity of glenoid bone, the shape of the glenoid, its version
relative to the scapular plane, and the relationship between the humeral head
and the glenoid.
Standardized anteroposterior and axillary views provide detailed insights into
the thickness of the cartilaginous space between the humeral head and the
glenoid, the relative positioning of the humeral head in relation to the
glenoid, the presence of osteophytes, the degree of osteopenia, and the extent
of bone deformities and erosions [39,40].
CT scans may be helpful for patients considering surgery, as they can provide a
greater understanding of scapular, glenoid, and humeral anatomy and factors that
may influence implant selection and placement.
Laboratory test
Laboratory tests of blood or joint fluid are not always required for evaluating
an arthritic shoulder, except in two cases: when inflammatory or septic
arthritis is suspected. In such instances, tests like rheumatoid factor,
anti-cyclic citrullinated peptide antibody, C-reactive protein, and erythrocyte
sedimentation rate may be useful [41].
Treatment
Activity modification
Most patients with shoulder osteoarthritis wish to maintain their daily,
work, and recreational activities. However, continued full participation in
these activities may exacerbate their arthritis symptoms. Typically, jobs
that require pushing heavy loads or applying shock loads, as well as certain
recreational activities, can accelerate the progression of the disease and
its symptoms. Making modifications in occupational and recreational
activities can alleviate symptoms and extend the lifespan of the natural
joint. Occupational therapy can facilitate workplace adjustments and may
also recommend adaptive changes at home. Modifying sports activities can
prove beneficial as well. Another crucial element of nonsurgical management
involves optimizing the patient’s overall health through regular
aerobic exercise.
Exercise and manual therapy
Shoulder osteoarthritis is commonly linked to joint contracture and stiffness
due to adhesions involving the GHJ capsule, rotator cuff muscles, and the
non-articular humeroscapular motion interface. Disuse or tendon rupture can
lead to weakness in the deltoid and cuff muscles. However, shoulder function
can often be enhanced through a gentle range of motion and strengthening
exercise program [42]. The exercise
program starts with active shoulder range of motion exercises performed
within a pain-free range. As pain decreases, passive shoulder range of
motion exercises are introduced. Joint mobilization is a therapeutic
technique used to enhance joint function and accessory motion, which can
lead to pain relief and increased range of motion. Combining a structured
exercise program with joint mobilization has proven effective in reducing
pain and improving function in patients with various shoulder disorders
[43]. Muscle strengthening begins
with low-intensity resistance training using elastic bands for movements
such as external and internal rotation, abduction, and forward flexion. This
is complemented by modified push-ups against a wall to introduce gentle
load-bearing. In more advanced phases, the program includes isometric
exercises, where static pressure is applied against an immovable object to
build stability, and light weightlifting to mimic functional tasks like
overhead reaching. These exercises are carefully monitored to ensure they
remain pain-free and are adjusted according to individual tolerance, thereby
facilitating gradual improvements in strength, range of motion, and overall
shoulder function.
NSAIDs
NSAIDs, such as ibuprofen, naproxen, and celecoxib, are widely used to
relieve pain and reduce inflammation in arthritis. These drugs inhibit
cyclooxygenase (COX) enzymes, thereby decreasing the production of
prostaglandins that are responsible for mediating inflammation and pain. In
osteoarthritis, NSAIDs have shown greater pain reduction compared to
acetaminophen [44]. Selective COX-2
inhibitors, such as celecoxib, are associated with fewer gastrointestinal
side effects than non-selective NSAIDs. In addition to oral administration,
topical NSAIDs are frequently used in treatment regimens. Due to their
effective pain relief and anti-inflammatory properties, NSAIDs are
recommended as the first-line therapy in the conservative management of
shoulder osteoarthritis [45].
Corticosteroid injections
Intra-articular corticosteroid injections offer targeted relief for moderate
to severe joint inflammation. Medications like triamcinolone or
methylprednisolone are injected directly into the affected joint, providing
strong anti-inflammatory effects. These injections are especially effective
for acute flare-ups, quickly reducing swelling and pain. However, their
repeated use can lead to complications such as cartilage damage, joint
infection, or systemic side effects, including hyperglycemia. Consequently,
their use is more appropriate for short-term symptom management rather than
long-term treatment [46,47]. One study suggested limiting the
number of injections to a maximum of three to reduce the risk of infection
and other adverse effects [48].
Neuropathic pain remedies
In cases where arthritis pain includes neuropathic components, medications
such as gabapentin or pregabalin can be effective. These drugs function by
modulating calcium channel activity within the nervous system, which reduces
the transmission of pain signals. They are particularly beneficial in
scenarios where conventional pain relievers are inadequate for managing
nerve-related pain. However, common side effects such as dizziness, fatigue,
and weight gain necessitate careful dose adjustments to minimize adverse
effects, particularly in older adult patients.
Platelet-rich plasma injections
PRP therapy involves drawing a patient's blood, concentrating the
platelets, and then injecting the plasma into the affected joint to
encourage healing and tissue regeneration. Platelets release growth factors
that can reduce inflammation and stimulate the repair of cartilage. PRP is
recognized as a regenerative treatment option and has demonstrated the
potential to enhance symptoms and functionality in cases of osteoarthritis
[49]. However, one study
indicated that serious complications, such as infections and inflammatory
reactions necessitating multiple surgical interventions, can arise following
biologic injection therapy [50].
Conclusion
Shoulder pain in older adults often results from chronic degenerative RCTs or
osteoarthritis, which can lead to functional impairment and a reduced quality of
life. Early detection through comprehensive physical examinations and imaging is
crucial for effective management. Nonsurgical approaches such as physical therapy,
activity modification, pharmacotherapy, and innovative treatments like PRP can help
alleviate pain, maintain mobility, and possibly postpone the need for surgery.
However, each treatment option has its own advantages and drawbacks. Developing
tailored, individualized treatment plans is critical for ensuring safer outcomes,
especially considering the unique comorbidities present in older populations.
Ultimately, timely, evidence-based care is key to preserving independence and
enhancing overall well-being in the daily lives of older adults.
Authors' contributions
Project administration: Jeong HS
Conceptualization: Jeong HS
Methodology & data curation: Kim KJ
Funding acquisition: not applicable
Writing – original draft: Kim KJ, Jeong HS
Writing – review & editing: Kim KJ, Jeong HS
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Burner T, Abbott D, Huber K, Stout M, Fleming R, Wessel B, et al. Shoulder symptoms and function in geriatric
patients. J Geriatr Phys Ther 2014;37(4):154-158.
2. Kukkonen J, Ryösä A, Joukainen A, Lehtinen J, Kauko T, Mattila K, et al. Operative versus conservative treatment of small, nontraumatic
supraspinatus tears in patients older than 55 years: over 5-year follow-up
of a randomized controlled trial. J Shoulder Elbow Surg 2021;30(11):2455-2464.
3. Meng C, Jiang B, Liu M, Kang F, Kong L, Zhang T, et al. Repair of rotator cuff tears in patients aged 75 years and older:
does it make sense? A systematic review. Front Public Health 2022;10:1060700
4. Pogorzelski J, DelVecchio BM, Hussain ZB, Fritz EM, Godin JA, Millett PJ. Superior capsule reconstruction for massive rotator cuff tears -
key considerations for rehabilitation. Int J Sports Phys Ther 2017;12(3):390-401.
5. Radhakrishnan R, Goh J, Tan AHC. Partial-thickness rotator cuff tears: a review of current
literature on evaluation and management. Clin Shoulder Elb 2024;27(1):79-87.
6. Riley GP, Harrall RL, Constant CR, Chard MD, Cawston TE, Hazleman BL. Tendon degeneration and chronic shoulder pain: changes in the
collagen composition of the human rotator cuff tendons in rotator cuff
tendinitis. Ann Rheum Dis 1994;53(6):359-366.
9. Diebold G, Lam P, Walton J, Murrell GAC. Relationship between age and rotator cuff retear: a study of
1,600 consecutive rotator cuff repairs. J Bone Joint Surg 2017;99(14):1198-1205.
14. Lenza M, Buchbinder R, Takwoingi Y, Johnston RV, Hanchard NCA, Faloppa F. Magnetic resonance imaging, magnetic resonance arthrography and
ultrasonography for assessing rotator cuff tears in people with shoulder
pain for whom surgery is being considered. Cochrane Database Syst Rev 2013;2013(9):CD009020
18. Kuhn JE, Dunn WR, Sanders R, An Q, Baumgarten KM, Bishop JY, et al. Effectiveness of physical therapy in treating atraumatic
full-thickness rotator cuff tears: a multicenter prospective cohort
study. J Shoulder Elbow Surg 2013;22(10):1371-1379.
19. Merolla G, Paladini P, Saporito M, Porcellini G. Conservative management of rotator cuff tears: literature review
and proposal for a prognostic. Prediction score. Muscles Ligaments Tendons J 2011;1(1):12-19.
20. Moosmayer S, Lund G, Seljom U, Svege I, Hennig T, Tariq R, et al. Comparison between surgery and physiotherapy in the treatment of
small and medium-sized tears of the rotator cuff: a randomised controlled
study of 103 patients with one-year follow-up. J Bone Joint Surg Br 2010;92(1):83-91.
21. Rajani AM, Shah UA, Mittal ARS, Gupta S, Garg R, Rajani AA, et al. Effects of glenohumeral corticosteroid injection on stiffness
following arthroscopic rotator cuff repair: a prospective, multicentric,
case-control study with 18-month follow-up. Clin Shoulder Elb 2023;26(1):64-70.
24. Koester MC, Dunn WR, Kuhn JE, Spindler KP. The efficacy of subacromial corticosteroid injection in the
treatment of rotator cuff disease: a systematic review. J Am Acad Orthop Surg 2007;15(1):3-11.
25. Chen X, Jones IA, Park C, Vangsness CT Jr.. The efficacy of platelet-rich plasma on tendon and ligament
healing: a systematic review and meta-analysis with bias
assessment. Am J Sports Med 2018;46(8):2020-2032.
26. Strauss FJ, Nasirzade J, Kargarpoor Z, Stähli A, Gruber R. Effect of platelet-rich fibrin on cell proliferation, migration,
differentiation, inflammation, and osteoclastogenesis: a systematic review
of in vitro studies. Clin Oral Investig 2020;24(2):569-584.
28. Jo CH, Kim JE, Yoon KS, Shin S. Platelet-rich plasma stimulates cell proliferation and enhances
matrix gene expression and synthesis in tenocytes from human rotator cuff
tendons with degenerative tears. Am J Sports Med 2012;40(5):1035-1045.
29. Barman A, Mishra A, Maiti R, Sahoo J, Thakur KB, Sasidharan SK. Can platelet-rich plasma injections provide better pain relief
and functional outcomes in persons with common shoulder diseases: a
meta-analysis of randomized controlled trials. Clin Shoulder Elb 2022;25(1):73-89.
30. Rodeo SA, Delos D, Williams RJ, Adler RS, Pearle A, Warren RF. The effect of platelet-rich fibrin matrix on rotator cuff tendon
healing: a prospective, randomized clinical study. Am J Sports Med 2012;40(6):1234-1241.
31. Weber SC, Kauffman JI, Parise C, Weber SJ, Katz SD. Platelet-rich fibrin matrix in the management of arthroscopic
repair of the rotator cuff: a prospective, randomized, double-blinded
study. Am J Sports Med 2013;41(2):263-270.
32. Rha D, Park GY, Kim YK, Kim MT, Lee SC. Comparison of the therapeutic effects of ultrasound-guided
platelet-rich plasma injection and dry needling in rotator cuff disease: a
randomized controlled trial. Clin Rehabil 2013;27(2):113-122.
33. Dakkak M, Saleem A, Patel D, Yeager M, Oliveira L, Gilot G, et al. A systematic review of randomized control trials looking at
functional improvement of rotator cuff partial thickness tears following
platelet-rich-plasma injection: a comparison of glenohumeral joint vs.
subacromial bursa vs. intratendinous injection locations. JSES Int 2024;8(3):464-471.
34. Jo YH, Kim DH, Lee BG. When should reverse total shoulder arthroplasty be considered in
glenohumeral joint arthritis? Clin Shoulder Elb 2021;24(4):272-278.
35. Ibounig T, Simons T, Launonen A, Paavola M. Glenohumeral osteoarthritis: an overview of etiology and
diagnostics. Scand J Surg 2021;110(3):441-451.
37. Vijian K, Cheng YT, Idris Z, Izaini Ghani AR, Abdul Halim S, Abdullah JM. Manual muscle testing of the scapula and the upper limb through
bedside examination. Malays J Med Sci 2023;30(1):198-212.
38. D'Antonio L, Fiumana G, Reina M, Lodi E, Porcellini G. Breaking the operator variability in Kibler's scapular
dyskinesis assessment. Musculoskelet Surg 2024;108(3):347-357.
39. Märtens N, März V, Bertrand J, Lohmann CH, Berth A. Radiological changes in shoulder osteoarthritis and pain
sensation correlate with patients' age. J Orthop Surg Res 2022;17(1):277
41. Bouillanne O, Morineau G, Dupont C, Coulombel I, Vincent JP, Nicolis I, et al. Geriatric nutritional risk index: a new index for evaluating
at-risk elderly medical patients. Am J Clin Nutr 2005;82(4):777-783.
42. Yamamoto N, Szymski D, Voss A, Ishikawa H, Muraki T, Cunha RA, et al. Non-operative management of shoulder osteoarthritis: current
concepts. J ISAKOS 2023;8(5):289-295.
43. Ho CYC, Sole G, Munn J. The effectiveness of manual therapy in the management of
musculoskeletal disorders of the shoulder: a systematic
review. Man Ther 2009;14(5):463-474.
44. Pincus T, Koch G, Lei H, Mangal B, Sokka T, Moskowitz R, et al. Patient preference for placebo, acetaminophen (paracetamol) or
celecoxib efficacy studies (PACES): two randomised, double blind, placebo
controlled, crossover clinical trials in patients with knee or hip
osteoarthritis. Ann Rheum Dis 2004;63(8):931-939.
46. Kim YT, Kim TY, Lee JB, Hwang JT. Glenohumeral versus subacromial steroid injections for
impingement syndrome with mild stiffness: a randomized controlled
trial. Clin Shoulder Elb 2023;26(4):390-396.
49. Elfatah AMA, Taeimah MO, Hasan MM, Ismael MSAA. Effect of platelet rich plasma therapy for shoulder
osteoarthritis: double blinded randomized controlled study. QJM Int J Med 2023;116(Suppl 1):134-135.
Conservative treatment of older adult patients with shoulder
diseases: a narrative review
Fig. 1.
The active range of motion is assessed by forward elevation (A),
external rotation with the elbow at the side of the body (B), and the
internal rotation angle is usually assessed by the height of the
vertebral body (yellow line) from behind (C). Provided by the authors
after consent of the examinee.
Fig. 2.
The presence of osteophytes on the greater tuberosity and acromion of
the humerus indicates that there is a high possibility of a rotator cuff
tear. Provided by the authors.
Fig. 3.
Magnetic resonance images show a partial tear of the supraspinatus
tendon (A), and a complete tear of the supraspinatus tendon (B).
Provided by the authors.
Fig. 4.
Anteroposterior and axillary-lateral plain X-ray images of
osteoarthritis of the shoulder joint show narrowing of the joint space
and formation of osteophytes. Provided by the authors.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Conservative treatment of older adult patients with shoulder
diseases: a narrative review