1Department of Internal Medicine and Liver Research Institute, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
*Corresponding author: Su Jong Yu,
Department of Internal Medicine and Liver Research Institute, Seoul National
University Hospital, Seoul National University College of Medicine, 101
Daehak-ro, Jongno-gu, Seoul 03080, Korea, E-mail:
ydoctor2@snu.ac.kr
• Received: November 29, 2024 • Revised: January 4, 2025 • Accepted: January 7, 2025
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Hepatocellular carcinoma with portal vein tumor thrombosis presents a significant
therapeutic challenge due to its poor prognosis and limited treatment options.
This review thoroughly examines diagnostic methods, including imaging techniques
and classification systems such as the Japanese Vp and Cheng’s
classifications, to aid in clinical decision-making. Treatment strategies
encompass liver resection and liver transplantation, particularly living donor
liver transplantation after successful downstaging, which have shown potential
benefits in selected cases. Locoregional therapies, including hepatic arterial
infusion chemotherapy, transarterial chemoembolization, transarterial
radioembolization, and external beam radiation therapy, remain vital components
of treatment. Recent advancements in systemic therapies, such as sorafenib,
lenvatinib, and immune checkpoint inhibitors (e.g., atezolizumab plus
bevacizumab) have demonstrated improvements in overall survival and
progression-free survival. These developments underscore the importance of a
multidisciplinary and personalized approach to improve outcomes for patients
with hepatocellular carcinoma and portal vein tumor thrombosis.
In recent years, treatment strategies for hepatocellular carcinoma (HCC) have
significantly advanced, incorporating locoregional therapies, surgical
resection, liver transplantation (LT), and systemic therapies, including
immunotherapy [1–3]. Despite these advancements, portal vein
tumor thrombosis (PVTT) continues to pose a major challenge in the treatment of
HCC. It represents a critical prognostic factor associated with advanced
disease, limited therapeutic options, and poor clinical outcomes [4–6].
The American Association for the Study of Liver Diseases (AASLD), the European
Association for the Study of the Liver (EASL), and groups in the Asia-Pacific
region have published region-specific guidelines for treating HCC with PVTT.
These guidelines account for differences in clinical practices, resource
availability, and patient characteristics [7–11]. Despite these
efforts, a consensus on the best treatment approach has yet to be reached,
making the management of HCC with PVTT a significant clinical challenge.
Objectives
This review comprehensively summarizes and analyzes treatment strategies for HCC
with PVTT. By integrating the latest research evidence and clinical insights,
this article provides guidance on identifying the most optimal treatment
strategies for HCC with PVTT in real-world clinical settings.
Ethics statement
As this study is a literature review, it did not require institutional review board
approval or individual consent.
Diagnosis and classification of portal vein tumor thrombosis
PVTT is the most prevalent type of macrovascular invasion (MVI) in HCC, with its
occurrence at diagnosis ranging from 10% to over 40% [5,12,13]. It can be identified via imaging techniques, particularly
on three-phase contrast-enhanced CT scans, where it presents as solid lesions within
the portal vein across all phases. These lesions are marked by contrast enhancement
during the arterial phase and subsequent washout in the portal venous phase [14]. In contrast, portal vein thrombosis (PVT),
often resulting from complications related to cirrhosis or splenectomy, does not
show arterial phase enhancement and can be managed with anticoagulant therapy. Thus,
accurately differentiating PVTT from PVT is crucial [15]. Another diagnostic tool, 18F-fluorodeoxyglucose (FDG)
positron emission tomography/CT, has proven highly effective in distinguishing
between malignant and benign thrombi. Malignant thrombi show moderate to high FDG
uptake, unlike their benign counterparts [16,17]. The non-invasive
diagnostic criteria for differentiating PVTT from PVT, referred to as A-VENA, rely
on the presence of three or more indicators: alpha-fetoprotein levels exceeding
1,000 ng/dL, venous expansion, thrombus enhancement, neovascularity, and proximity
to HCC [18].
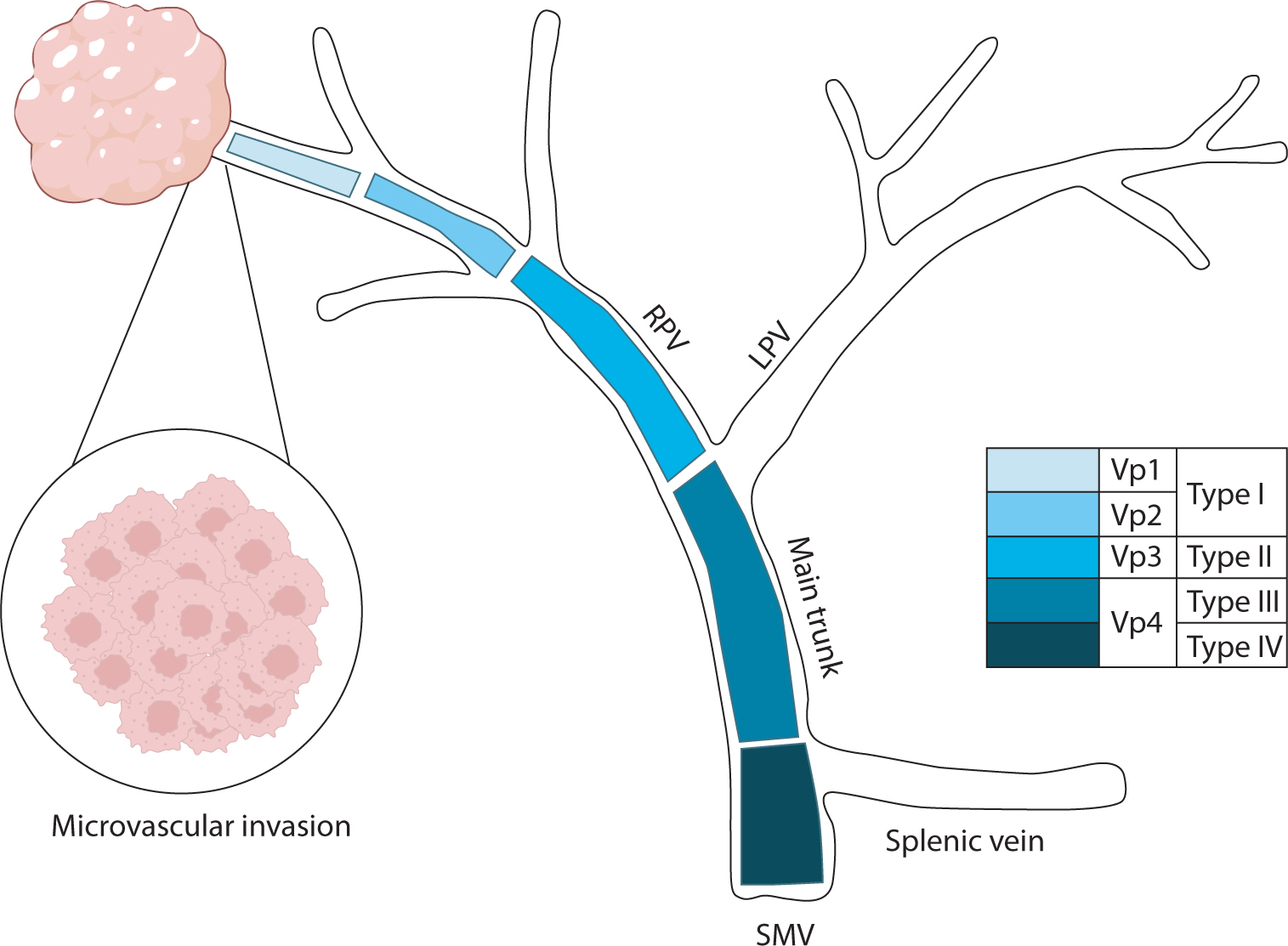
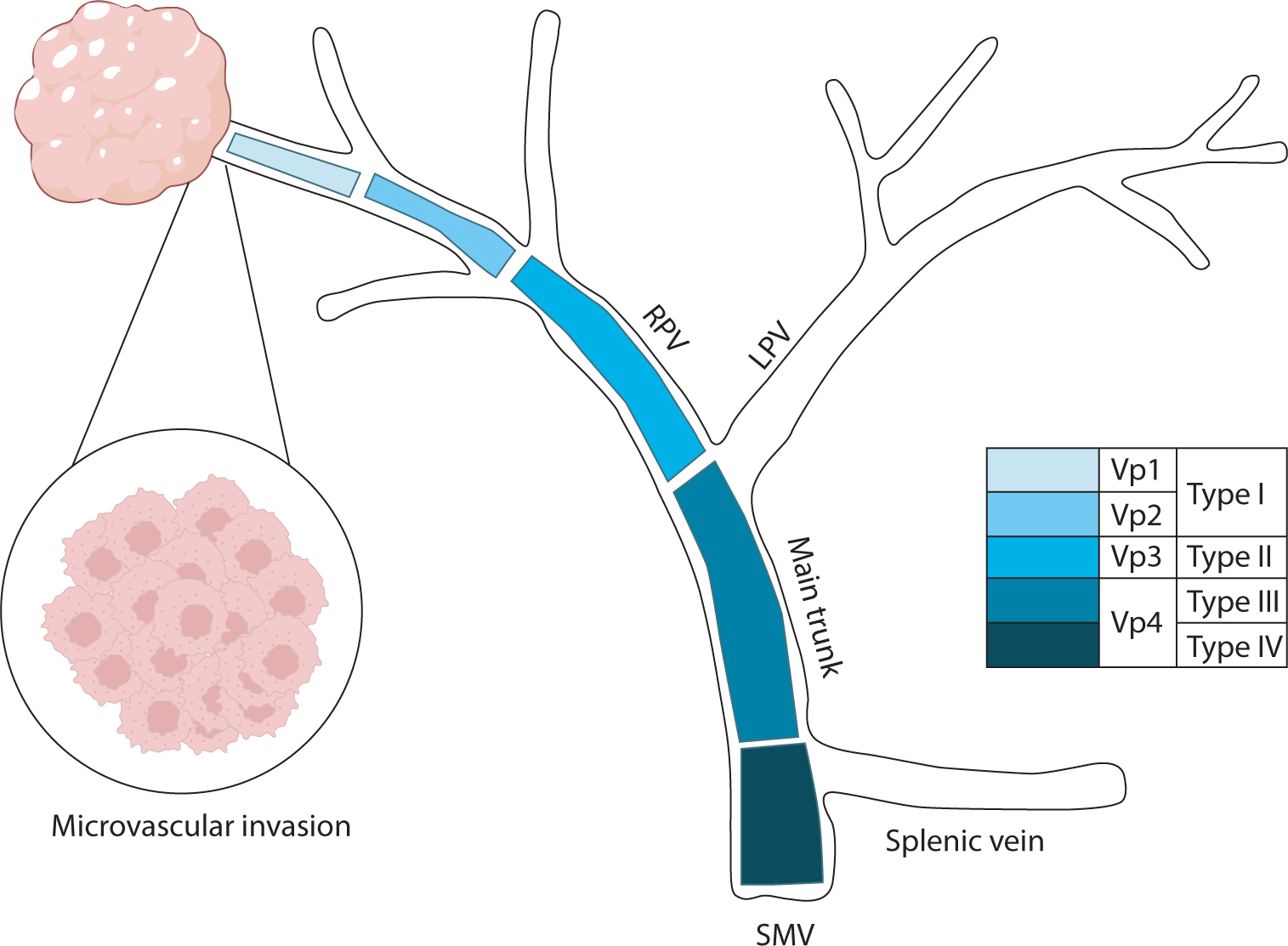
Two widely used systems for assessing the extent of PVTT are the Japanese Vp
classification [19] and Cheng’s
classification, as illustrated in Fig. 1 [20]. The VP classification divides the extent
of tumor thrombus in the portal vein into four levels: Vp1, which involves the
segmental branches of the portal vein; Vp2, affecting the second-order branches;
Vp3, involving the first-order branches; and Vp4, which affects the main trunk of
the portal vein and/or the contralateral branch. Cheng’s classification also
delineates four grades: type I, where the tumor thrombus is located in the segmental
or sectoral branches of the portal vein or higher; type II, involving the right or
left portal vein; type III, affecting the main portal vein; and type IV, involving
the superior mesenteric vein.
Fig. 1.
Classification of portal vein tumor thrombosis in hepatocellular
carcinoma. RPV, right portal vein; LPV, left portal vein; SMV, superior
mesenteric vein.
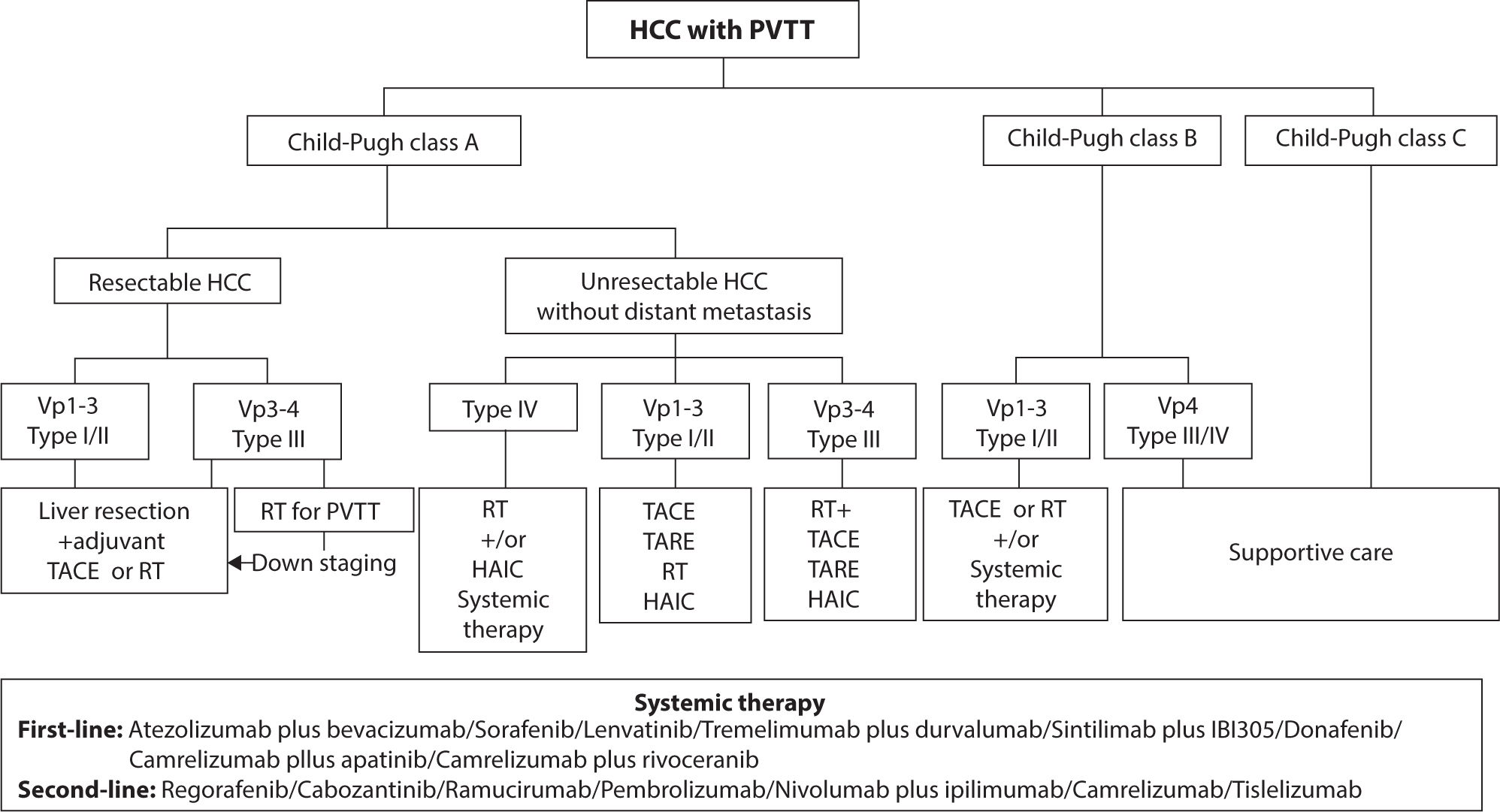
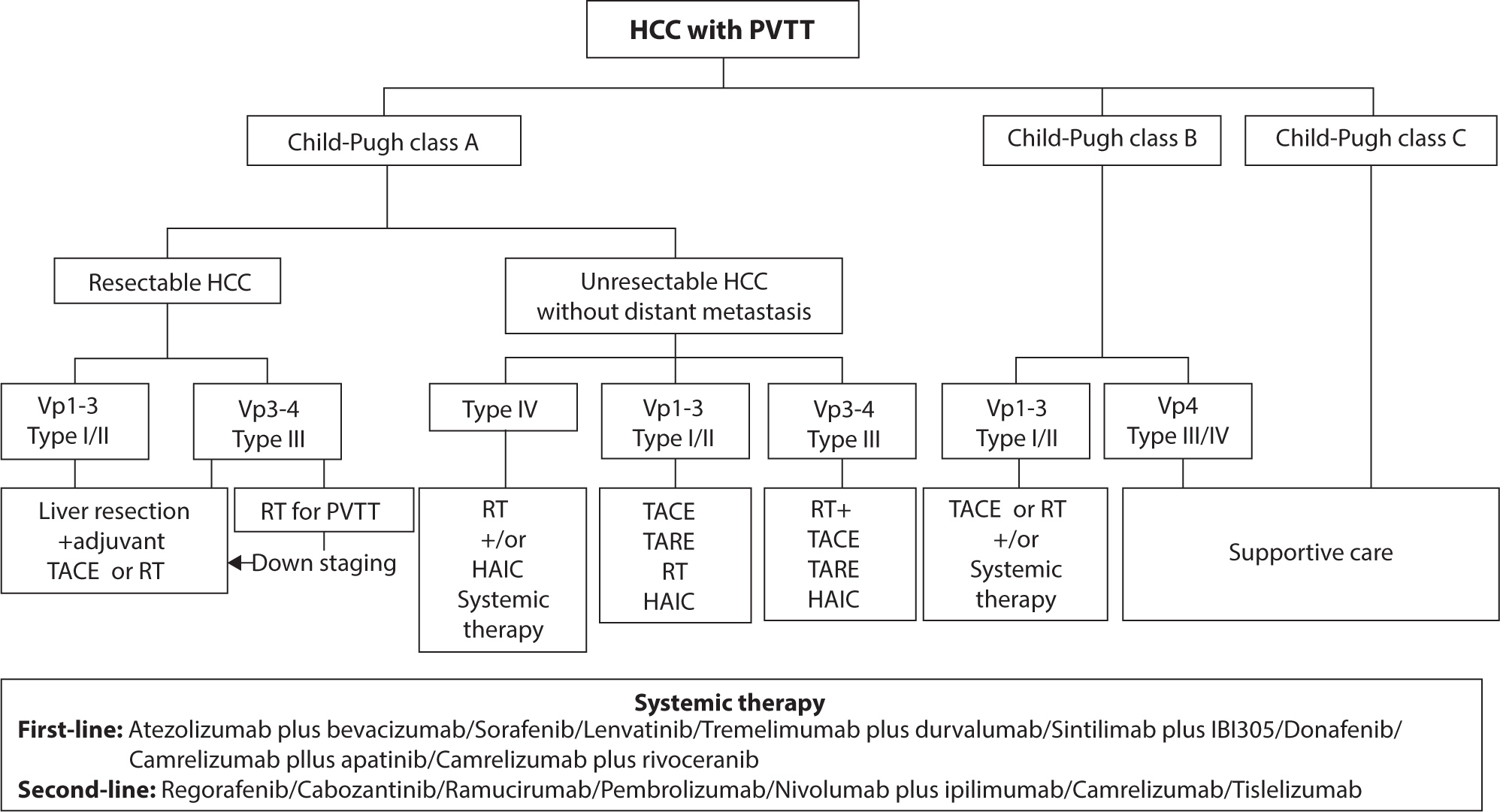
Treatment options for hepatocellular carcinoma with portal vein tumor
thrombosis
The current evidence-based treatment algorithms for HCC patients with PVTT are
presented in Fig. 2.
Liver resection is a curative treatment for patients with HCC and, according to
the Barcelona Clinic Liver Cancer (BCLC) staging system, is considered feasible
only in early-stage HCC (BCLC stage 0 or A). The presence of PVTT, regardless of
tumor size or extent, is classified as BCLC stage C, making liver resection
contraindicated [21]. However, in the
Asia-Pacific region, liver resection is performed for selected patients outside
the BCLC staging system, with several studies demonstrating moderately favorable
outcomes. Retrospective analyses have shown that liver resection significantly
improves overall survival (OS) in patients with HCC and PVTT, particularly in
those with Child-Pugh class A liver function, except in cases involving Vp4 PVTT
[22]. A systematic review of 29
studies found that the median OS was longer in patients undergoing liver
resection compared to those receiving systemic therapy. The location and extent
of PVTT were critical factors influencing survival outcomes, with patients
exhibiting distal portal vein branch invasion achieving a 5-year survival rate
of 45%, while those with main trunk invasion had survival rates of less than 15%
[23]. Clinical guidelines in Korea
recommend liver resection for HCC patients with PVTT if the main portal trunk is
not involved and liver function is well-preserved [8]. Similarly, Japanese guidelines permit liver resection in
cases of portal vein invasion up to the first branch (Vp1–[3]) [9]. In China, liver resection is advised for patients with Child-Pugh
class A liver function, PVTT types I or II, and an ECOG performance status of
0–1. Patients with type III PVTT are also considered eligible for liver
resection either directly or after tumor downstaging through radiotherapy [7].
Liver transplantation
PVTT has traditionally been viewed as an absolute contraindication due to its
strong association with high recurrence rates and poor prognosis [24,25]. Additionally, the use of deceased donor LT in managing HCC with
PVTT is limited by the scarcity of available donor organs. However, advancements
in surgical techniques have led to an increased adoption of living donor LT for
patients with HCC and PVTT. With improvements in locoregional therapies for HCC
with PVTT, LT following successful downstaging has emerged as a key area of
interest. Retrospective analyses indicate that patients with segmental PVTT who
underwent living donor LT experienced significantly better OS and disease-free
survival (DFS) rates than those with lobar PVTT [26]. Similarly, studies involving patients with major vascular
invasion who underwent downstaging using 3D conformal radiation therapy (RT) and
transarterial chemoembolization (TACE) prior to LT showed significantly higher
3-year DFS and OS rates for those meeting the Milan criteria than those who did
not [26].
Hepatic artery infusion chemotherapy
Hepatic arterial infusion chemotherapy (HAIC) is a commonly used treatment for
advanced HCC. This method involves delivering chemotherapeutic agents such as
platinum/oxaliplatin and 5-fluorouracil directly into intrahepatic tumor lesions
via a catheter or pump. HAIC is recommended for HCC patients who have major
portal vascular invasion and Child-Pugh A liver function but are not eligible
for hepatectomy, radiofrequency ablation, TACE, or systemic therapy [9]. A meta-analysis of six studies
demonstrated that HAIC outperformed sorafenib in HCC patients with PVTT,
particularly in those with types III-IV PVTT. HAIC showed better OS,
progression-free survival (PFS), and disease control rate, although it was
associated with higher rates of myelosuppression [27]. Additionally, a phase III randomized controlled trial
(SILIUS study) from Japan reported that combining HAIC with sorafenib improved
OS compared to sorafenib alone in patients with Vp4 PVTT. However, no
significant difference in median OS was observed for patients with Vp1-3 PVTT
[28]. Furthermore, a study comparing
TACE-HAIC combined with targeted therapy and immunotherapy to TACE alone in HCC
patients with PVTT showed superior outcomes for the combination group, with
significantly better OS [29].
Transarterial chemoembolization
TACE is a widely utilized technique for managing unresectable HCC with PVTT
[30]. It is particularly considered
for patients with good liver function and sufficient collateral circulation
around the obstructed portal vein [31,32]. In patients with type
III/IV PVTT, its application remains controversial due to the associated risks
of liver infarction and hepatic failure, although TACE has shown potential to
extend OS [33]. A meta-analysis of 13
trials involving 1,933 patients was conducted to assess the safety and efficacy
of TACE in managing HCC with PVTT. The study found that patients with PVTT in
the main portal vein trunk had significantly worse survival rates compared to
those with segmental PVTT (P<0.001) [34]. The limited effectiveness of TACE as a standalone therapy
highlights the importance of combining it with other treatment modalities to
improve OS in patients with HCC and PVTT [35]. A study comparing the effectiveness of TACE combined with RT
against sorafenib therapy demonstrated that the combination therapy achieved a
median OS of 12.8 months, significantly higher than the 10.0 months observed
with sorafenib alone (P=0.04) [36]. An
analysis of 25 studies, including 2,577 patients, revealed that combining TACE
with RT significantly improved the 1-year survival rate compared to TACE alone
[37]. This finding suggests that the
TACE and RT combination could serve as a primary treatment approach for HCC
patients with MVI [38]. The median OS was
significantly longer in the TACE and sorafenib combination group compared to the
sorafenib monotherapy group (8.9 vs. 5.9 months, P=0.009), with improved OS
observed in patients with MVI (hazard ratio [HR] 0.64; 95% CI 0.44–0.92;
P=0.02) [39]. The clinical outcomes of
combining TACE with immune checkpoint inhibitors are still limited, and further
research is needed to establish their efficacy and potential benefits.
Transarterial radioembolization
Transarterial radioembolization (TARE) with yttrium-90 microspheres is recognized
as an effective treatment option for HCC patients with PVTT, offering a unique
approach that combines microembolization with targeted radiotherapy [40]. Two phase III studies found no
significant difference in OS between TARE and sorafenib [41,42]. However, a
meta-analysis of 17 trials revealed higher 6-month and 1-year OS rates in the
TARE group (76% and 47%, respectively) compared to the sorafenib group (54% and
24%) [43]. A case report suggested that
concurrent TARE and combination therapy with atezolizumab plus bevacizumab could
be an effective and safe treatment regimen for patients with infiltrative HCC
and PVTT [44]. Nonetheless, retrospective
studies and clinical trials are warranted to validate these findings. Existing
evidence suggests that TARE is an effective treatment for HCC patients with
PVTT, with response rates ranging from 50% to 75% and a median survival time of
approximately 10 months [40]. Although
internal radiotherapy is a more invasive treatment, it delivers a sustained high
dose of radiation to PVTT while sparing nearby normal liver tissue, making it
particularly beneficial for patients with malignant portal vein stenosis or
occlusion [45].
External beam radiation therapy
For patients with unresectable HCC and all types of PVTT, RT is recommended,
targeting both the primary tumor and PVTT lesions. Advances in technologies such
as three-dimensional conformal RT, intensity-modulated RT, and stereotactic body
RT (SBRT) have enabled higher radiation doses to be delivered to the targeted
areas while protecting adjacent normal tissues [46,47]. Target localization
for RT often utilizes CT and magnetic resonance imaging fusion based on lipiodol
deposition following TACE [48]. The
optimal irradiation area remains a topic of debate and should be personalized.
In cases where the hepatic lesion is small and PVTT is nearby, both the tumor
and PVTT can be targeted simultaneously. For larger tumors or distant PVTT,
irradiation may be focused exclusively on the PVTT [49]. Studies have shown that RT, either as a standalone
treatment or combined with other modalities, improves survival and quality of
life in these patients. When comparing sorafenib and RT in HCC patients with
Vp3-4 PVTT, RT showed a significantly better median OS after propensity score
matching (10.9 vs. 4.8 months; P=0.025) [50]. Similarly, in a Korean multicenter retrospective cohort study
using propensity score matching, RT demonstrated an improved response rate in
HCC patients with PVTT [51]. The efficacy
of SBRT combined with sorafenib compared to SBRT alone was retrospectively
assessed in patients with HCC and PVTT [52]. The findings demonstrated that the combination therapy resulted
in longer median PFS (6 vs. 3 months) and median OS (12.5 vs. 7 months) than
SBRT alone, although these differences were not statistically significant.
Systemic therapy
Atezolizumab with bevacizumab
The combination of atezolizumab and bevacizumab has been established as a
first-line systemic therapy for unresectable HCC, as demonstrated by its
superiority over sorafenib in the IMbrave150 trial [53]. This regimen has demonstrated a strong antitumor
effect in advanced HCC with Vp4 PVTT and is associated with minimal impact on
hepatic function in the early stages of treatment [54], along with a favorable initial response [55]. Updated efficacy and safety data from
the IMbrave150 trial show that patients with MVI experienced improved median OS
and PFS when treated with atezolizumab plus bevacizumab compared to those
treated with sorafenib (Tables 1, 2) [56]. Additionally, therapeutic outcomes of atezolizumab plus
bevacizumab and lenvatinib have been found comparable for managing HCC with PVTT
[57]. A multicenter cohort study
conducted in South Korea demonstrated that atezolizumab plus bevacizumab
achieved superior 1-year survival and PFS rates compared to TACE plus RT in HCC
patients with PVTT and no metastasis. These findings suggest that atezolizumab
plus bevacizumab should be considered a primary treatment option for this
patient group [58].
Table 1.
Overall survival in clinical trials of first-line or second-line
systemic therapy for unresectable HCC with PVTT
Subgroup analyses from multiple clinical trials of immune checkpoint inhibitors
have assessed clinical outcomes in patients with HCC and MVI (Tables 1, 2). The HIMALAYA trial evaluated the clinical outcomes of combining
tremelimumab with durvalumab versus using sorafenib alone. It showed a trend
toward improved OS in patients with HCC and MVI, although the results did not
reach statistical significance [59]. The
CARES-310 trial compared camrelizumab plus rivoceranib with sorafenib and
demonstrated statistically significant improvements in both OS and PFS for
patients with HCC and MVI [60]. In the
context of second-line treatment, the KEYNOTE-240 trial, which compared
pembrolizumab to placebo, was the sole study to specifically analyze clinical
outcomes in patients with HCC and MVI. Despite not achieving statistical
significance, pembrolizumab exhibited a trend toward better OS and PFS compared
to placebo [61]. Notably, unlike the
IMbrave150 trial, these clinical trials excluded patients with Vp4 or type
III/IV PVTT.
Sorafenib
Sorafenib, an orally administered multi-kinase inhibitor, was the first targeted
therapy approved for HCC patients with PVTT, based on the results of two phase
III randomized, double-blind, placebo-controlled trials [62,63]. The SHARP
trial reported a median survival time of 10.7 months [63], whereas an Asia-Pacific study reported a median
survival time of 6.5 months [10].
However, real-world outcomes may be less favorable due to potential selection
bias in clinical trials [10,64]. The phase III STAH study suggested
that combining sorafenib with TACE might improve OS in HCC patients with PVTT
compared to sorafenib alone, although the difference was not statistically
significant [65]. Additionally, a
randomized controlled trial involving 99 patients with HCC, cirrhosis, and PVTT
found that combining sorafenib with radiofrequency ablation significantly
improved OS rates compared to sorafenib monotherapy [66].
Lenvatinib
Lenvatinib, a multi-kinase inhibitor with antiangiogenic properties, has been
shown to be effective in treating advanced HCC, as evidenced by a randomized
phase III noninferiority trial [67]. In
comparison to sorafenib, lenvatinib not only demonstrated similar median
survival times but also achieved a higher objective response rate and longer PFS
[67]. Additionally, a case report
highlighted that after 11 months of treatment with lenvatinib for advanced HCC
with PVTT, the PVTT became undetectable, and the vascularization of the primary
tumor had resolved [68].
Conclusion
The management of HCC with PVTT requires a multidisciplinary approach that
incorporates locoregional therapies, systemic treatments, and surgical
interventions, all tailored to the specific clinical context of each patient. Recent
advancements, such as immune checkpoint inhibitors and combination strategies like
TACE with RT, have shown considerable promise in enhancing clinical outcomes. These
developments highlight the critical need for personalized treatment strategies to
navigate the complexities and improve the prognosis for this high-risk
population.
Authors' contributions
Project administration: Park J, Yu SJ
Conceptualization: Park J, Yu SJ
Methodology & data curation: Park J, Yu SJ
Funding acquisition: not applicable
Writing – original draft: Park J, Yu SJ
Writing – review & editing: Park J, Yu SJ
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Teufel A, Kudo M, Qian Y, Daza J, Rodriguez I, Reissfelder C, et al. Current trends and advancements in the management of
hepatocellular carcinoma. Dig Dis 2024;42(4):349-360.
2. Sankar K, Gong J, Osipov A, Miles SA, Kosari K, Nissen NN, et al. Recent advances in the management of hepatocellular
carcinoma. Clin Mol Hepatol 2024;30(1):1-15.
3. Yang X, Yang C, Zhang S, Geng H, Zhu AX, Bernards R, et al. Precision treatment in advanced hepatocellular
carcinoma. Cancer Cell 2024;42(2):180-197.
4. Chan SL, Mo FKF, Johnson PJ, Liem GS, Chan TC, Poon MC, et al. Prospective validation of the Chinese University Prognostic Index
and comparison with other staging systems for hepatocellular carcinoma in an
Asian population. J Gastroenterol Hepatol 2011;26(2):340-347.
5. Llovet JM, Bustamante J, Castells A, Vilana R, Del Carmen Ayuso M, Sala M, et al. Natural history of untreated nonsurgical hepatocellular
carcinoma: rationale for the design and evaluation of therapeutic
trials. Hepatology 1999;29(1):62-67.
6. Connolly GC, Chen R, Hyrien O, Mantry P, Bozorgzadehd A, Abt P, et al. Incidence, risk factors and consequences of portal vein and
systemic thromboses in hepatocellular carcinoma. Thromb Res 2008;122(3):299-306.
7. Sun J, Guo R, Bi X, Wu M, Tang Z, Lau WY, et al. Guidelines for diagnosis and treatment of hepatocellular
carcinoma with portal vein tumor thrombus in China (2021
edition). Liver Cancer 2022;11(4):315-328.
8. Korean Liver Cancer Association, National Cancer Center (NCC)
Korea. 2022 KLCA-NCC Korea practice guidelines for the management of
hepatocellular carcinoma. Korean J Radiol. 2022 23(12):p. 1126-1240.
9. Kudo M, Kawamura Y, Hasegawa K, Tateishi R, Kariyama K, Shiina S, et al. Management of hepatocellular carcinoma in Japan: JSH consensus
statements and recommendations 2021 update. Liver Cancer 2021;10(3):181-223.
11. Finn RS, Zhu AX, Farah W, Almasri J, Zaiem F, Prokop LJ, et al. Therapies for advanced stage hepatocellular carcinoma with
macrovascular invasion or metastatic disease: a systematic review and
meta‐analysis. Hepatology 2018;67(1):422-435.
13. Minagawa M, Makuuchi M. Treatment of hepatocellular carcinoma accompanied by portal vein
tumor thrombus. World J Gastroenterol 2006;12(47):7561-7567.
14. Hennedige T, Venkatesh SK. Advances in computed tomography and magnetic resonance imaging of
hepatocellular carcinoma. World J Gastroenterol 2016;22(1):205-220.
15. Ponziani FR, Zocco MA, Campanale C, Rinninella E, Tortora A, Maurizio LD, et al. Portal vein thrombosis: insight into physiopathology, diagnosis,
and treatment. World J Gastroenterol 2010;16(2):143-155.
16. Agarwal KK, Shah D, Shah N, Mayank M. Differentiation of malignant thrombus from bland thrombus of the
portal vein in patient with hepatocellular carcinoma on 18F-FDG PET
CT. Clin Nucl Med 2017;42(11):e472-e474.
17. Wu B, Zhang Y, Tan H, Shi H. Value of 18F-FDG PET/CT in the diagnosis of portal vein tumor
thrombus in patients with hepatocellular carcinoma. Abdom Radiol 2019;44(7):2430-2435.
18. Sherman CB, Behr S, Dodge JL, Roberts JP, Yao FY, Mehta N, et al. Distinguishing tumor from bland portal vein thrombus in liver
transplant candidates with hepatocellular carcinoma: the A‐VENA
criteria. Liver Transpl 2019;25(2):207-216.
19. Ikai I, Yamamoto Y, Yamamoto N, Terajima H, Hatano E, Shimahara Y, et al. Results of hepatic resection for hepatocellular carcinoma
invading major portal and/or hepatic veins. Surg Oncol Clin N Am 2003;12(1):65-75.
20. Shuqun C, Mengchao W, Han C, Feng S, Jiahe Y, Guanghui D, et al. Tumor thrombus types influence the prognosis of hepatocellular
carcinoma with the tumor thrombi in the portal vein. Hepato-gastroenterology 2007;54(74):499-502.
21. Reig M, Forner A, Rimola J, Ferrer-Fàbrega J, Burrel M, Garcia-Criado Á, et al. BCLC strategy for prognosis prediction and treatment
recommendation: the 2022 update. J Hepatol 2022;76(3):681-693.
22. Kokudo T, Hasegawa K, Matsuyama Y, Takayama T, Izumi N, Kadoya M, et al. Survival benefit of liver resection for hepatocellular carcinoma
associated with portal vein invasion. J Hepatol 2016;65(5):938-943.
23. Glantzounis GK, Paliouras A, Stylianidi MC, Milionis H, Tzimas P, Roukos D, et al. The role of liver resection in the management of intermediate and
advanced stage hepatocellular carcinoma. A systematic review. Eur J Surg Oncol 2018;44(2):195-208.
24. Mazzaferro V, Llovet JM, Miceli R, Bhoori S, Schiavo M, Mariani L, et al. Predicting survival after liver transplantation in patients with
hepatocellular carcinoma beyond the Milan criteria: a retrospective,
exploratory analysis. Lancet Oncol 2009;10(1):35-43.
25. Xu X, Lu D, Ling Q, Wei X, Wu J, Zhou L, et al. Liver transplantation for hepatocellular carcinoma beyond the
Milan criteria. Gut 2016;65(6):1035-1041.
26. Choi HJ, Kim DG, Na GH, Hong TH, Bae SH, You YK, et al. The clinical outcomes of patients with portal vein tumor thrombi
after living donor liver transplantation. Liver Transpl 2017;23(8):1023-1031.
27. Liu M, Shi J, Mou T, Wang Y, Wu Z, Shen A. Systematic review of hepatic arterial infusion chemotherapy
versus sorafenib in patients with hepatocellular carcinoma with portal vein
tumor thrombosis. J Gastroenterol Hepatol 2020;35(8):1277-1287.
28. Kudo M, Ueshima K, Yokosuka O, Ogasawara S, Obi S, Izumi N, et al. Sorafenib plus low-dose cisplatin and fluorouracil hepatic
arterial infusion chemotherapy versus sorafenib alone in patients with
advanced hepatocellular carcinoma (SILIUS): a randomised, open label, phase
3 trial. Lancet Gastroenterol Hepatol 2018;3(6):424-432.
29. Yuan Y, He W, Yang Z, Qiu J, Huang Z, Shi Y, et al. TACE-HAIC combined with targeted therapy and immunotherapy versus
TACE alone for hepatocellular carcinoma with portal vein tumour thrombus: a
propensity score matching study. Int J Surg 2023;109(5):1222-1230.
31. Chung GE, Lee JH, Kim HY, Hwang SY, Kim JS, Chung JW, et al. Transarterial chemoembolization can be safely performed in
patients with hepatocellular carcinoma invading the main portal vein and may
improve the overall survival. Radiology 2011;258(2):627-634.
32. Kim HC, Chung JW, Lee W, Jae HJ, Park JH. Recognizing extrahepatic collateral vessels that supply
hepatocellular carcinoma to avoid complications of transcatheter arterial
chemoembolization. Radiographics 2005;25:suppl_1. S25-S39.
35. Luo F, Li M, Ding J, Zheng S. The progress in the treatment of hepatocellular carcinoma with
portal vein tumor thrombus. Front Oncol 2021;11:635731
36. Yoon SM, Ryoo BY, Lee SJ, Kim JH, Shin JH, An JH, et al. Efficacy and safety of transarterial chemoembolization plus
external beam radiotherapy vs sorafenib in hepatocellular carcinoma with
macroscopic vascular invasion: a randomized clinical trial. JAMA Oncol 2018;4(5):661-669.
37. Huo YR, Eslick GD. Transcatheter arterial chemoembolization plus radiotherapy
compared with chemoembolization alone for hepatocellular carcinoma: a
systematic review and meta-analysis. JAMA Oncol 2015;1(6):756-765.
38. Jin S, Choi WM, Shim JH, Lee D, Kim KM, Lim YS, et al. Subclassification of advanced-stage hepatocellular carcinoma with
macrovascular invasion: combined transarterial chemoembolization and
radiotherapy as an alternative first-line treatment. J Liver Cancer 2023;23(1):177-188.
39. Choi GH, Shim JH, Kim MJ, Ryu MH, Ryoo BY, Kang YK, et al. Sorafenib alone versus sorafenib combined with transarterial
chemoembolization for advanced-stage hepatocellular carcinoma: results of
propensity score analyses. Radiology 2013;269(2):603-611.
41. Chow PKH, Gandhi M, Tan SB, Khin MW, Khasbazar A, Ong J, et al. SIRveNIB: selective internal radiation therapy versus sorafenib
in Asia-Pacific patients with hepatocellular carcinoma. J Clin Oncol 2018;36(19):1913-1921.
43. Kim PH, Choi SH, Kim JH, Park SH. Comparison of radioembolization and sorafenib for the treatment
of hepatocellular carcinoma with portal vein tumor thrombosis: a systematic
review and meta-analysis of safety and efficacy. Korean J Radiol 2019;20(3):385-398.
44. Park MK, Yu SJ. Concurrent transarterial radioembolization and combination
atezolizumab/bevacizumab treatment of infiltrative hepatocellular carcinoma
with portal vein tumor thrombosis: a case report. J Liver Cancer 2022;22(1):69-74.
45. Tan Z, Lu J, Zhu G, Chen L, Wang Y, Zhang Q, et al. Portal vein irradiation stent plus chemoembolization versus
external radiotherapy plus chemoembolization in hepatocellular carcinoma
with portal vein tumour thrombus: a retrospective study. Cardiovasc Intervent Radiol 2021;44(9):1414-1422.
47. Kang J, Nie Q, Du R, Zhang L, Zhang J, Li Q, et al. Stereotactic body radiotherapy combined with transarterial
chemoembolization for hepatocellular carcinoma with portal vein tumor
thrombosis. Mol Clin Oncol 2014;2(1):43-50.
48. Wang MH, Ji Y, Zeng ZC, Tang ZY, Fan J, Zhou J, et al. Impact factors for microinvasion in patients with hepatocellular
carcinoma: possible application to the definition of clinical tumor
volume. Int J Radiat Oncol Biol Phys 2010;76(2):467-476.
49. Yu JI, Park HC. Radiotherapy as valid modality for hepatocellular carcinoma with
portal vein tumor thrombosis. World J Gastroenterol 2016;22(30):6851-6863.
50. Nakazawa T, Hidaka H, Shibuya A, Okuwaki Y, Tanaka Y, Takada J, et al. Overall survival in response to sorafenib versus radiotherapy in
unresectable hepatocellular carcinoma with major portal vein tumor
thrombosis: propensity score analysis. BMC Gastroenterol 2014;14:84
51. Im JH, Yoon SM, Park HC, Kim JH, Yu JI, Kim TH, et al. Radiotherapeutic strategies for hepatocellular carcinoma with
portal vein tumour thrombosis in a hepatitis B endemic area. Liver Int 2017;37(1):90-100.
52. Que J, Wu HC, Lin CH, Huang CI, Li LC, Ho CH, et al. Comparison of stereotactic body radiation therapy with and
without sorafenib as treatment for hepatocellular carcinoma with portal vein
tumor thrombosis. Medicine 2020;99(13):e19660.
53. Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TT, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular
carcinoma. N Engl J Med 2020;382(20):1894-1905.
54. Komatsu S, Fujishima Y, Kido M, Kuramitsu K, Goto T, Yanagimoto H, et al. Significant response to atezolizumab plus bevacizumab treatment
in unresectable hepatocellular carcinoma with major portal vein tumor
thrombus: a case report. BMC Gastroenterol 2021;21(1):470
55. Hiraoka A, Kumada T, Tada T, Hirooka M, Kariyama K, Tani J, et al. Atezolizumab plus bevacizumab treatment for unresectable
hepatocellular carcinoma: early clinical experience. Cancer Rep 2022;5(2):e1464.
56. Cheng AL, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, et al. Updated efficacy and safety data from IMbrave150: atezolizumab
plus bevacizumab vs. sorafenib for unresectable hepatocellular
carcinoma. J Hepatol 2022;76(4):862-873.
57. Park J, Lee YB, Ko Y, Park Y, Shin H, Hur MH, et al. Comparison of atezolizumab plus bevacizumab and lenvatinib for
hepatocellular carcinoma with portal vein tumor thrombosis. J Liver Cancer 2024;24(1):81-91.
58. Lee SK, Kwon JH, Lee SW, Lee HL, Kim HY, Kim CW, et al. A real-world comparative analysis of atezolizumab plus
bevacizumab and transarterial chemoembolization plus radiotherapy in
hepatocellular carcinoma patients with portal vein tumor
thrombosis. Cancers 2023;15(17):4423
59. Abou-Alfa GK, Lau G, Kudo M, Chan SL, Kelley RK, Furuse J, et al. Tremelimumab plus durvalumab in unresectable hepatocellular
carcinoma. NEJM Evid 2022;1(8):EVIDoa2100070
60. Qin S, Chan SL, Gu S, Bai Y, Ren Z, Lin X, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line
therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised,
open-label, international phase 3 study. Lancet 2023;402(10408):1133-1146.
61. Finn RS, Ryoo BY, Merle P, Kudo M, Bouattour M, Lim HY, et al. Pembrolizumab as second-line therapy in patients with advanced
hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase
III trial. J Clin Oncol 2020;38(3):193-202.
62. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008;359(4):378-390.
63. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific
region with advanced hepatocellular carcinoma: a phase III randomised,
double-blind, placebo-controlled trial. Lancet Oncol 2009;10(1):25-34.
64. Jeong SW, Jang JY, Shim KY, Lee SH, Kim SG, Cha SW, et al. Practical effect of sorafenib monotherapy on advanced
hepatocellular carcinoma and portal vein tumor thrombosis. Gut Liver 2013;7(6):696-703.
65. Park JW, Kim YJ, Kim DY, Bae SH, Paik SW, Lee YJ, et al. Sorafenib with or without concurrent transarterial
chemoembolization in patients with advanced hepatocellular carcinoma: the
phase III STAH trial. J Hepatol 2019;70(4):684-691.
66. Giorgio A, Merola MG, Montesarchio L, Merola F, Santoro B, Coppola C, et al. Sorafenib combined with radio-frequency ablation compared with
sorafenib alone in treatment of hepatocellular carcinoma invading portal
vein: a western randomized controlled trial. Anticancer Res 2016;36(11):6179-6183.
67. Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib versus sorafenib in first-line treatment of patients
with unresectable hepatocellular carcinoma: a randomised phase 3
non-inferiority trial. Lancet 2018;391(10126):1163-1173.
68. Takeda H, Nishijima N, Nasu A, Komekado H, Kita R, Kimura T, et al. Long-term antitumor effect of lenvatinib on unresectable
hepatocellular carcinoma with portal vein invasion. Hepatol Res 2019;49(5):594-599.
Management strategies for advanced hepatocellular carcinoma with
portal vein tumor thrombosis
Fig. 1.
Classification of portal vein tumor thrombosis in hepatocellular
carcinoma. RPV, right portal vein; LPV, left portal vein; SMV, superior
mesenteric vein.