1College of Nursing , Yonsei University, Seoul, Korea
2College of Nursing, Kongju National University, Gongju, Korea
3College of Nursing, Jeonbuk National University, Jeonju, Korea
4College of Nursing & Research Institute of Nursing Innovation, Kyungpook National University, Daegu, Korea
5Research Institute of Nursing Science, College of Nursing, Seoul National University, Seoul, Korea
6College of Nursing, Ewha Womans University, Seoul, Korea
7College of Nursing Science, Kyung Hee University, Seoul, Korea
8College of Nursing, The Catholic University of Korea, Seoul, Korea
9Red Cross College of Nursing, Chung-Ang University, Seoul, Korea
10College of Nursing, Ajou University, Suwon, Korea
11Mo-Im Kim Nursing Research Institute, College of Nursing, Yonsei University, Seoul, Korea
*Corresponding author: Sue Kim, Mo-Im
Kim Nursing Research Institute, College of Nursing, Yonsei University, 50-1
Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea, E-mail:
suekim@yuhs.ac
• Received: December 15, 2024 • Accepted: January 20, 2025
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
The prevalence of postpartum depression (PPD) in Asia is reported to range from
13.53% to 22.31%. However, there remains a gap in the identification of PPD,
particularly regarding cultural cutoff points. Therefore, the purpose of this
scoping review was to determine the prevalence and associated factors of PPD in
Eastern, South-eastern, Western, and Southern Asian countries and analyze the
cutoff points of the Edinburgh Postnatal Depression Scale (EPDS) used across
these countries. Following Arksey and O'Malley’s five-step scoping
review framework, the population was defined as mothers, the concept as the
EPDS, and the context as the Asian region. A literature search was conducted
using PubMed, Embase, CINAHL, PsycINFO, and Web of Science. The data analysis
focused on demographic characteristics, EPDS cutoffs and features, PPD
prevalence, and its associated factors. Nineteen studies were selected. Most
countries used translated versions of the EPDS with demonstrated reliability and
validity. The cutoff scores varied, with most using scores of 10 or higher. The
prevalence of PPD ranged from 5.1% to 78.7%. Key associated factors for PPD
included cultural factors such as relationships with in-laws and preferences for
the newborn’s sex. To improve the accuracy of PPD screening in Asia, the
EPDS should be used consistently, and appropriate cutoff criteria must be
established. In addition, prevention strategies and programs that reflect the
cultural characteristics and social context of Asia need to be developed for the
early detection and prevention of PPD.
The postpartum period is a critical transitional phase for women, characterized by
significant physical and psychological changes. During this period, the prevalence
of depression is reported to be more than twice as high as at other times in a
woman’s life [1]. Postpartum depression
(PPD) is considered a precursor to major depressive disorder and is defined by
symptoms such as sadness, excessive crying, anxiety, agitation, low mood, loss of
interest, and sleep disturbance [2]. PPD can
progress to long-term depressive illness, particularly when accompanied by thoughts
of self-harm [3]. PPD typically begins 6 weeks
after childbirth and ranges in severity from mild to severe [4,5]. The prevalence of
PPD has been estimated at 17.2%, with reported rates in Asia ranging from 13.53% to
22.32% [6]. Despite its prevalence, PPD
remains among the most underdiagnosed and undertreated forms of depression, and
there is limited awareness regarding the importance of prevention and
intervention.
Several instruments have been used to identify PPD promptly, including the Edinburgh
Postnatal Depression Scale (EPDS), the PPD Screening Scale, and Beck's
Depression Inventory. The EPDS is considered the most reliable of these instruments
in terms of its sensitivity, specificity, and clinical validity for measuring PPD in
the postpartum period [7]. Moreover, the EPDS
includes a specific item on suicidal ideation, which is critical for evaluating the
severity of depression and facilitating timely referrals to mental health services
[8].
PPD is associated with various demographic and psychosocial factors, including low
economic status, low education, single motherhood, major stressful events, lack of
social and family support, history of depression, and unplanned pregnancy [9,10]. In
Asian cultures, traditional support from in-laws or female relatives can provide
physical and psychological comfort; however, it can also lead to interpersonal
conflict and emotional distress [4,5,11].
Furthermore, a longstanding cultural preference for male offspring, particularly for
the first child, is found in regions such as Eastern Asia, South-eastern Asia,
Western Asia (including Arab countries and Türkiye), and Southern Asia
(including India), which may contribute to the development of PPD [5].
Studies have systematically reviewed the prevalence and associated factors of PPD.
However, these studies were limited in scope, either focusing on single countries
within Asia [12,13] or providing broad reviews of the global literature [6] that lacked an Asia-specific context. In
2024, a systematic review was conducted in Asian cultural contexts [5], but it did not address the characteristics
of the EPDS in these contexts, such as culture-specific cutoff points, nor did it
explore cultural factors influencing PPD.
To fill this research gap, this study aimed to compare and analyze the prevalence of
PPD across Asian countries, examine the EPDS cutoffs used in each country, and
identify the cultural, psychosocial, and demographic factors associated with
PPD.
Methods
Ethical statement
As a scoping review of the existing literature, this study did not require
approval from the institutional review board or informed consent.
Study design
This study employed a scoping review design following the five-step framework
proposed by Arksey and O'Malley [14]. The process included (a) identification of research questions,
(b) literature search, (c) selection of relevant literature, (d) data analysis,
and (e) summarizing and reporting the findings [14]. The study adhered to the Preferred Reporting Items for
Systematic Reviews and Meta-Analysis Extension for Scoping Review (PRISMA ScR)
reporting guidelines for topical scoping reviews [15].
Step 1: identification of the research question
The primary research question was: "What are the recent research trends in
Asian countries regarding maternal PPD?" The specific research questions
were: (a) What is the prevalence of PPD among Asian mothers, (b) How do the EPDS
cutoffs differ across Asian countries, and (c) What are the cultural,
psychosocial, and demographic factors influencing PPD?
Step 2: literature search
A literature search was conducted between October 7 and October 14, 2024, in five
electronic databases: PubMed, Embase, CINAHL (EBSCO), PsycINFO, and Web of
Science, using a combination of three main search terms: “postpartum
depression,” “EPDS,” and “Asia.” Asian
countries were defined based on the United Nations Geoscheme [16], including countries from Eastern Asia,
South-eastern Asia, Southern Asia, and Western Asia.
Search strategies were developed by two researchers (authors L, M) using Boolean
operators to combine Medical Subject Headings (MeSH) with keywords and synonyms.
The final search strategies were reviewed by a professional librarian at the
authors’ institution. The search strategies for each database are
detailed in Supplement
1. The search was restricted to titles and abstracts using the final
search strategy in each database. Additionally, a supplementary search for
relevant literature not identified by the database search was conducted using
Google Scholar for 7 days following October 14, 2024.
Step 3: selection and exclusion criteria
Studies were included if they 1) were peer-reviewed journal articles addressing
the prevalence and factors associated with PPD in Asian mothers, 2) included the
usage of EPDS, 3) were written in English, and 4) were published from January 1,
2020 to September 30, 2024. The exclusion criteria were as follows: 1) gray
literature such as dissertations, case reports, posters, or abstracts; (b)
review articles or qualitative studies; (c) articles for which the full text was
not available; (d) studies that did not include outcomes at 6–8 weeks
postpartum; and (e) studies that did not address cultural, psychosocial, or
demographic factors associated with PPD (e.g., only included biological markers,
etc.).
The screening process was conducted independently by two researchers (authors L,
M). In the first phase, titles and abstracts of all retrieved studies were
reviewed based on the inclusion and exclusion criteria. In the second phase, the
full texts of the selected studies were reviewed using the same criteria for the
final selection. Any disagreements at any stage were resolved through
discussion. If no consensus was reached, a third researcher (author K) was
consulted.
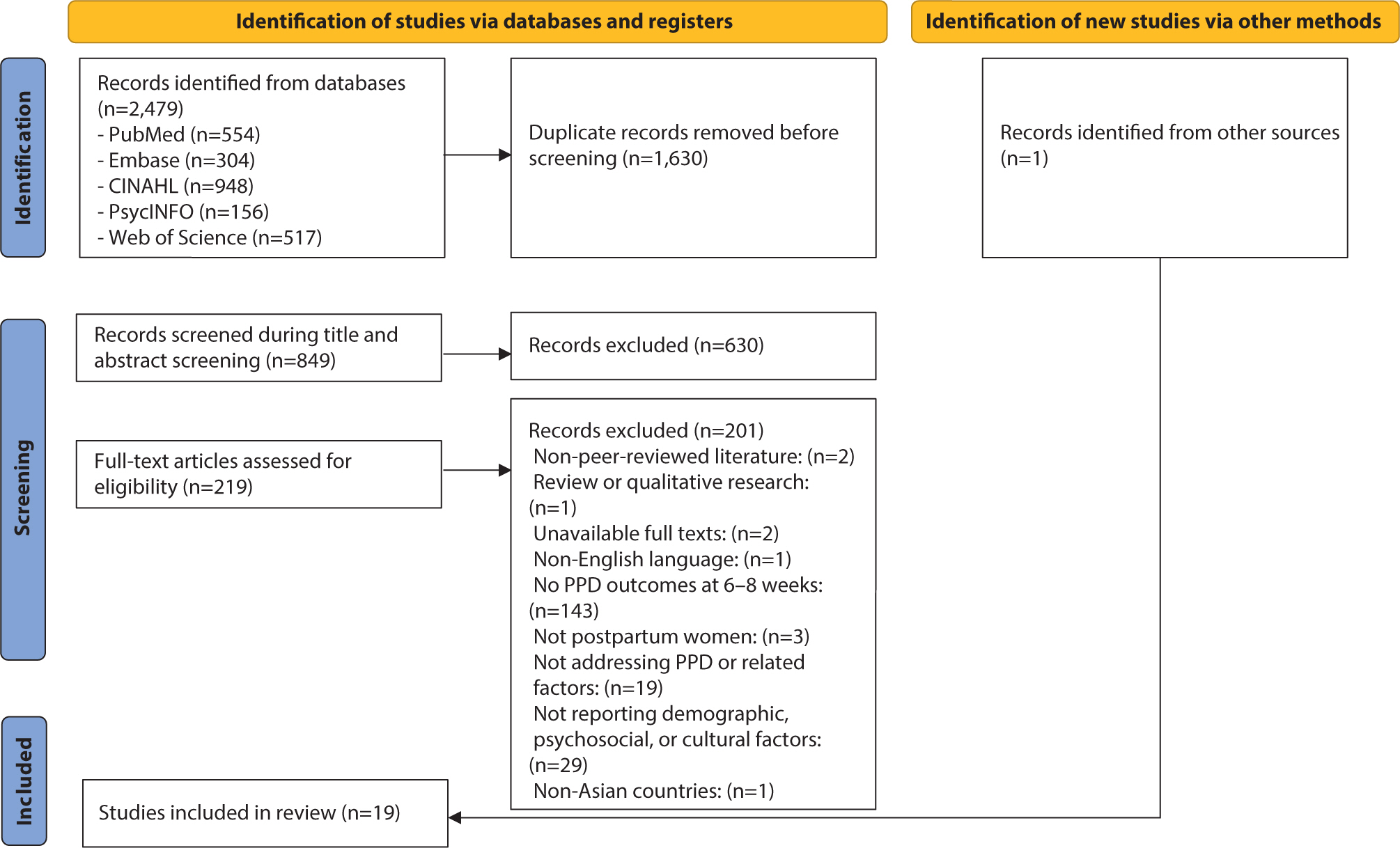
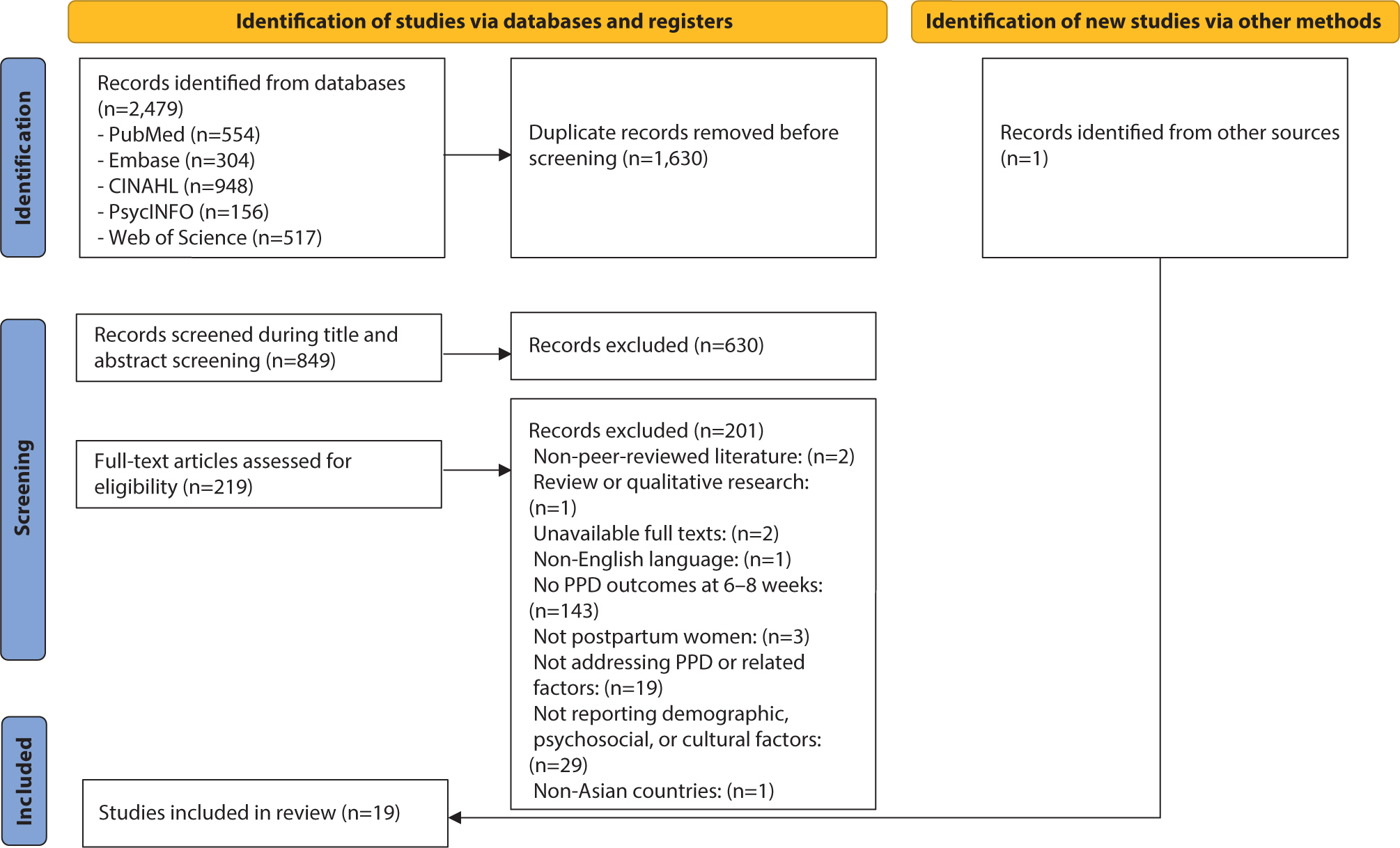
The initial search yielded 2,480 studies. After excluding duplicates, 850 studies
remained for screening. Based on titles and abstracts, 629 studies were
excluded, leaving 221 studies for full-text review. After applying the inclusion
and exclusion criteria to the full texts, 202 studies were excluded, and 19
studies [4,8–10,17–31] were finally selected for analysis (Fig. 1). The bibliographic management software EndNote 20
was used to store retrieved studies and remove duplicates.
A draft analysis framework was developed to record the data from the selected
literature, and the final analysis framework was finalized through research
meetings. The framework consisted of five main categories: publication
characteristics, study characteristics, EPDS characteristics, participant
characteristics, and study outcomes. All data were extracted, and frequency
analysis and descriptive statistics were performed using Microsoft Excel
2020.
Results
General characteristics of the selected studies
Table 1 summarizes the general
characteristics of the selected studies. The analysis of 19 studies revealed
that publications originated from 10 countries. China accounted for the largest
share with 7 studies (36.8%) [19–25], followed by
India with 3 studies (15.79%) [26–28], and Saudi
Arabia with 2 studies (10.53%) [8,31]. One study (5.26%) each was conducted
in Bhutan [17], Cambodia [18], South Korea [29], Laos [10],
Myanmar [4], the Philippines [30], and Türkiye [9].
Table 1.
General characteristics of the selected studies (n=19)
The distribution of studies over the past 5 years showed an increasing trend,
despite a dip during the COVID-19 pandemic. Specifically, 6 studies (31.58%)
were published in 2020 [9,10,21,24,27,30], 3 studies
(15.79%) in 2021 [22,23,29], and 1 study (5.26%) each in 2022 and 2023 [19,31]. The year 2024 saw a significant rise, with 8 studies (42.11%)
[4,8,17,18,20,25,26,28].
Regarding study design, the majority were cross-sectional (n=17, 89.47%) [4,8,10,17–28,30,31], one was a prospective cohort study (5.26%) [29], and one was a prospective longitudinal
study (5.26%) [9]. The number of
participants ranged from 65 to 4,813. One study [29] included both mothers and their spouses. Two studies [18,30] recruited participants from primary health care centers, while
17 studies [4,8–10,17,19–29,31] recruited participants from
hospitals.
General characteristics of the participants
The general characteristics of the participants are summarized in Table 2. Twelve studies reported the mean
age of participants, which was calculated to be 28.06±4.44 years. The age
range of participants varied across the studies; some included mothers aged 16
years and older [10], while others
included those aged 17 years and older [17,31]. Additionally, two
studies [19,24] focused on older mothers, aged 35 years or older.
Table 2.
Detailed characteristics of the selected studies (n=19)
- Age range: 17−48
years - Included mothers with a history of psychiatric
disorders
4–8 weeks
Translated and pilot-tested
(n=30)
- ≥11 - Mean score of
suspected PPD: 14.17±3.44
47 (14.97%)
- Poor relationship with
friends/in-laws - Perceived changes in body image,
perceived increased stress during pregnancy, and perceived
stress after delivery - History of pregnancy
complications, negative delivery experience, and poor health
status of the newborn
- Mean age: 28.6 years -
Included mothers with a history of psychiatric
disorders - Mothers with singleton pregnancy, and no
thyroid disorders
6–8 weeks
Translated and pilot-tested
(n=11)
- ≥10 - Mean score:
6.65±4.27
133 (30.2%)
- Poor relationship with spouse and
mother-in-law - Dissatisfaction with economic status,
unplanned pregnancy, and spouse’s employment in manual
labor/farming/factory work
- Mean age of PPD mothers:
28.25±3.785 (vs 29.57±4.123 in non-PPD) -
Excluded history of psychiatric disorders, pregnancy
complications, and medical conditions
6–7 weeks
Chinese version
≥10
73 (14.5%)
- Co-habitation with in-laws -
Younger maternal age and history of pregnancy complications
- Mothers ≥18 years, with
healthy term births, and no postpartum complications - No
information on psychiatric history
6 weeks
Chinese version
- ≥13 - Mean score:
8.18±5.80
279 (23.2%)
- Lower familial support, lower social
support from colleagues or friends, mother-in-law as the primary
caregiver of mother and newborn, and dissatisfaction with
childbirth experiences - Lower level of education,
unplanned pregnancy, and lower economic status
- Mean age: 26.25±3.90 -
Excluded mothers with a history of psychiatric
disorders - Mothers with Primiparity, and no pregnancy
complications
6 weeks
Chinese version
- ≥10 - Mean score:
13.94±5.70
118 (78.7%)
- Gap between familial expectations
for fetal sex and actual sex of the newborn, poor relationship
with spouse, mother-in-law, and one’s parents -
Higher parenting stress, the gap between perceived and actual
family support - Younger maternal age, lower economic
status, and poor health condition of the newborn
- Mean age: 21.58±2.31 -
Excluded mothers with a history of psychiatric
disorders - Mothers with no abortions/ medical
terminations
6–8 weeks
No information on EPDS version
≥13
22 (33.8%)
- Living in an extended family
structure, pressure from the family to become pregnant, pressure
for a female child, and poor relationship with spouse, in-laws,
and one’s parents - Younger maternal age, lower
level of education, lower economic status, history of pregnancy
complications, multiple fetuses, and unplanned pregnancy
- Mean age: 28.1
(16−44) - Included mothers with a history of
psychiatric disorders - Mothers with a singleton
pregnancy, and no thyroid disorders
6–8 weeks
Translated and pilot-tested
(n=20)
- ≥10 - Mean score:
7.1±4.6
136 (31.8%)
- Poor relationship with spouse,
one’s parents, and mother-in-law - Dissatisfaction
with childbirth experiences - Higher education levels of
participants and spouses, unplanned pregnancy, multiparity,
housewife, and spousal unemployment
- Married mothers aged 18−49
years - Excluded mothers with a history of psychiatric
disorders
6 weeks
Arabic version
- ≥10 - Mean score:
2.54±4.5
15 (5.6%)
- Living in an extended family
structure - Lower level of education, spousal
unemployment, lower economic status, multiple fetuses, history
of pregnancy complications
- Mean age: 27.3±5.2 -
Mean age of PPD mothers: 28.2±5.2 (vs 27.2±5.2
non-PPD) - No information on psychiatric history -
Mothers with Primiparity and a singleton pregnancy
6–8 weeks
Turkish version
≥13
44 (18%)
- Increased marital conflict -
Increased perceived stress during pregnancy
Regarding obstetric characteristics, 3 studies [9,22,25] focused on primiparity, and 6 studies [4,9,10,18,22,29] included only mothers of singleton
births. Nine studies [8,19,20,24–26,28–30] included
mothers with no psychiatric history, and 7 [10,18,20–22,25,28] recruited only participants with no health problems or
complications related to pregnancy and birth. One study [26] excluded mothers with a history of abortion or induced
termination of pregnancy, and another [27] excluded cases where the infant had health conditions.
Edinburgh Postnatal Depression Scale characteristics by country
Edinburgh Postnatal Depression Scale version
A total of 16 studies (84.21%) described the EPDS version used, with 13
(68.42%) using translated versions validated for reliability and validity in
their respective countries. Six of those used the Chinese version [20–25], followed by Hindi [27,28], Arabic [8,31], Korean [29], Burmese
[4], and Turkish [9] versions. Three studies (17.79%) used
translations done by the researchers, pilot-tested but without reported
psychometric analyses: these were from Bhutan [17], Cambodia [18], and Laos [10].
The EPDS is typically validated for reliability and validity within each
country, with a standard cutoff of 13 or higher frequently adapted to fit
the local cultural context [32].
However, among these 19 studies, there was variability in cutoff points,
even within the same country.
A cutoff point of 10 or higher was most commonly used, appearing in 10 out of
the 19 studies (42.11%). These studies spanned various regions: India [28] in Southern Asia; Cambodia [18], Laos [10], Myanmar [4],
and the Philippines [30] in
Southeastern Asia; Saudi Arabia [8] in
Western Asia; and South Korea [29]
along with China [20,23,25] in Eastern Asia. Two studies from Cambodia [18] and Laos [10] cited research on EPDS cutoff points in primary
healthcare settings in non-English-speaking countries [33]. Meanwhile, studies from China [23], South Korea [29], Myanmar [10], and Saudi Arabia [8]
referenced validation studies of the EPDS translated into their respective
languages [34–37]. Additionally, 2 studies from China
[22,24] utilized cutoffs based on research assessing the
clinical significance of EPDS cutoffs in English-speaking mothers [38].
A cutoff point of 9 or higher was reported in one study (5.26%) conducted in
China [19], referencing a prior
validation study of the Chinese version of the EPDS [39]. One study (5.26%) from Bhutan [17] used a cutoff of 11 or higher,
which based its criteria on a systematic review of EPDS cutoffs in the
global literature [40]. Another study
(5.26%) from India [27] used a cutoff
point of 12 or higher but did not provide details on a specific rationale or
evidence for this criterion.
In contrast, a cutoff point of 13 or higher was reported in six studies from
China [21,22,24], India
[26], Saudi Arabia [31], and Türkiye [9]. The rationale for this cutoff
included a validation study of the Turkish EPDS version [41] and a previously validated Arabic
version that was assessed for reliability and validity [42]. Conversely, two Chinese studies
[21,22] cited a systematic review of EPDS cutoff points in
global literature [43] and the
original developer’s publication on the EPDS [44]. Two other studies [24,26] did not provide a
rationale for their chosen cutoff points. However, the original developer of
the EPDS [44] recommended that cutoff
points for translated versions of the EPDS might not be universally
applicable across different cultures and emphasized the importance of
establishing semantic, technical, diagnostic, and conceptual equivalence
when adapting the EPDS for various cultural contexts.
Edinburgh Postnatal Depression Scale mean scores
Nine studies (47.37%) reported mean EPDS scores and SD, although one [17] provided only the mean for
participants suspected of having PPD. The remaining 8 studies [4,8,10,18,21,22,25,27] showed a mean EPDS score of 7.75±5.09.
The mean and SD of EPDS scores from studies conducted in South-Eastern Asia,
specifically in Cambodia [18], Laos
[10], and Myanmar [4], were calculated to be
6.72±4.71. A study from India [27] in Southern Asia reported slightly higher values
(7.67±5.9), while a study from Saudi Arabia [8] in Western Asia reported lower values
(2.54±4.5). The unusually low EPDS mean score in the Saudi study
[8] may be attributed to the
demographic characteristics of the participants, over 90% of whom had a
university education or higher and resided in nuclear family settings.
Prevalence and associated factors of postpartum depression
Prevalence
The prevalence of PPD ranged from 5.1% [8] to 78.7% [25]. In
Eastern Asia, South Korea [29]
reported 24.6%, while Chinese studies ranged from 11.6% [23] to 78.7% [25]. In South-eastern Asia, reported prevalence was
30.2% in Cambodia [18], 31.8% in Laos
[10], 31.9% in Myanmar [4], and 16.4% in the Philippines [30]. In Southern Asia, Bhutan [17] reported 14.9%, while rates in
India ranged from 17.4% [28] to 33.8%
[26]. In Western Asia,
Türkiye [9] reported 18%,
whereas Saudi Arabia reported the lowest rates (5.1% [31] and 5.6% [8]). Thus, the lowest prevalence was found in Saudi Arabia, while
the highest was found in China.
Cultural factors
Various cultural factors contributing to PPD were identified in 18 studies
(Table 3), with a particular
focus on family relationships. The most frequently mentioned factor was poor
relationships with in-laws (n=7), followed by negative relationships with
the spouse (n=4) and the mother's own parents (n=3). Additionally,
living with in-laws (n=2) and having the mother-in-law as the primary
caregiver for the mother and newborn (n=1) were also reported as
contributing factors.
Table 3.
Classification of factors associated with PPD
Factors
Categories
n
References
Cultural
Poor relationship with
in-laws
7
10,17,18,24–27
Poor relationship with spouse
4
10,18,25,26
Poor relationship with
parents
3
10,25,26
Co-habitation with in-laws
2
20,23
Female newborn
2
24,28
Gap between familial expectations
for fetal sex and actual sex of the newborn
2
24,25
Living in an extended family
structure
2
8,26
Living in a nuclear family
2
4,28
Mother-in-law as the primary
caregiver of mother and newborn
1
21
Pressure from the family to become
pregnant
1
26
Pressure for a female child
1
26
Psychosocial
Lower familial support
4
4,19,21,27
Lower social support
4
21,22,29,31
Higher daily life stress
2
23,29
Higher parenting stress
2
25,29
Dissatisfaction with marriage
2
27,29
Dissatisfaction with childbirth
experiences
2
10,21
Dissatisfaction with economic
status
2
4,18
Perceived increased stress during
pregnancy
2
9,17
Perceived stress after
delivery
1
17
Symptoms of postpartum
post-traumatic stress disorder
1
22
Perceived changes in body
image
1
17
Gap between perceived and actual
family support
1
25
Lower level of self-esteem
1
29
Increased marital conflict
1
9
Demographic
History of pregnancy
complications
6
8,17,19,20,26,27
Unplanned pregnancy
6
4,10,18,21,26,28
Lower economic status
5
8,21,25,26
Lower level of education
4
8,19,21,26
Younger maternal age
3
20,25,26
Multiparity
3
10,28,30
Poor health condition of the
newborn
3
17,22,25
Spousal unemployment
2
8,10
Housewife
2
10,23
Primiparity
2
23,24
Multiple fetuses
2
8,26
Higher education levels of
participants and spouses
1
10
Negative delivery experience
1
17
Spouse’s employment in
manual labor/farming/factory work
1
18
Having a professional
occupation
1
30
PPD, postpartum depression.
The influence of newborn sex also emerged as a significant cultural factor,
particularly when the newborn was female (n=2) or when there was a
discrepancy between family expectations and the actual sex of the newborn
(n=2). Additionally, one study identified family pressure to conceive as a
factor linked to PPD.
Psychosocial factors
Thirteen studies identified psychosocial factors associated with PPD [4,9,10,17–19,21–23,25,27,29,31]. The most commonly reported factors
were low family support and low social support from colleagues or friends,
each mentioned in four studies. Other factors included high levels of daily
life stress, parenting stress, dissatisfaction with marriage, childbirth
experiences, and economic status, each cited in two studies.
Demographic factors
The most commonly reported demographic factors included pregnancy
complications and unplanned pregnancies, each cited in six studies. These
were followed by low economic status, reported in five studies; low level of
education, in four studies; and young maternal age, multiparity, and poor
neonatal health, each noted in three studies. Less frequently mentioned
factors were spousal unemployment, the mother's occupation as a
housewife, primiparity, and multiple fetuses, each reported in two
studies.
Discussion
This study found that the prevalence of PPD was lowest in Saudi Arabia at 5.1% [8] and highest in China at 78.7% [25]. These findings are somewhat consistent
with previous reports, which have shown PPD prevalence in Asian countries to range
from 4.9% to 93% [5]. Earlier studies have
indicated variability in PPD prevalence across Asia, with the lowest rates reported
in South Korea [5,6] and the highest in Japan [5] or Afghanistan [6]. However,
considering that Korean nurses exhibited significantly higher rates of PPD (45.9%)
compared to their US counterparts (3.4%) [45], it is crucial to carefully examine variations in sampling methods,
participant characteristics, and the use of culturally sensitive cutoffs.
Among the cultural factors associated with PPD, a negative relationship with in-laws
has been identified as a contributing factor, consistent with findings from a
previous study in Japan [46]. This may be
linked to Confucian influences that emphasize recognition and affirmation by the
extended family in Asia. Similarly, the extended family—a traditional family
structure in Asian countries—has been reported to increase the risk of PPD
[46]. However, while some studies have
identified the extended family as a factor [8,26], others have pointed to the
nuclear family structure as associated with PPD [4,28]. Interestingly, living with
a mother-in-law was found to be a significant factor for PPD, aligning with results
from a previous study in China [47]. Our
findings regarding cultural factors related to the newborn’s sex also mirror
those of the earlier study conducted in China [47], suggesting that Confucian preferences for boys in Asian countries
may contribute to familial conflict and, consequently, increase the risk of PPD.
In terms of the psychosocial factors associated with PPD, a lack of family and social
support was identified as a key factor. Family support during the postpartum period
is crucial for maternal well-being, as close relationships and daily interactions
with the spouse and other family members offer both emotional and practical support
[4]. This observation aligns with the
findings of systematic reviews from Western Asia, which analyzed the relationship
between social support and PPD [1,48]. These insights suggest that healthcare
providers should consider the family environment and educate spouses and family
members about PPD. Regarding demographic characteristics, unplanned pregnancies, low
education levels, low income, and younger maternal age have been significantly
associated with PPD. These associations are consistent with studies conducted in
Western Asia [1,11].
This study has limitations. Strict inclusion criteria may have excluded some articles
that contained relevant insights into PPD. In addition, most included studies were
cross-sectional, limiting conclusions about causality. Some recent research suggests
that environmental factors (e.g., endocrine disruptors, and air pollution) could
also influence PPD [49,50]. Future research should consider these factors to gain a
more comprehensive understanding of PPD. Despite these limitations, this review
highlights the need for consistent use of the EPDS and the establishment of
standardized cutoff points to enhance the accuracy of PPD screening in Asian
countries. It also emphasizes the importance of strengthening family and community
support systems to improve maternal psychological well-being and prevent PPD.
Developing prevention strategies and programs that reflect Asia’s diverse
cultural and social contexts will be key to the early detection and prevention of
PPD.
In conclusion, the prevalence of PPD in Asian countries widely varied, ranging from
5.1% to 78.7%. Although most studies used translated EPDS versions that had been
previously validated for reliability and validity, there was variability in the EPDS
cutoff points, even within individual countries such as India, Saudi Arabia, and
China. This variability underscores the need for a standardized approach to using
the EPDS, including adopting internationally recognized standardized translations
and establishing consistent cutoff criteria that take into account the cultural
characteristics of Asian countries.
This study identified that cultural factors, including relationships with in-laws and
issues related to the sex of the newborn, are significant in the context of PPD
among Asian mothers. To definitively establish the connection between cultural
influences and PPD, further prospective cohort or population-based studies are
required.
Authors' contributions
Project administration: Moon B, Kim HK, Nho JH, Choi H, Chung CW, Kang SJ, Kim
JH, Lee JY, Park S, Shin G, Song JE, Kim S
Conceptualization: Kim HK, Nho JH, Kim S
Methodology & Data curation: Moon B, Lee MH, Kim S
Funding acquisition: not applicable
Writing – original draft: Moon B
Writing – review & editing: Moon B, Kim HK, Nho JH, Choi H, Chung
CW, Kang SJ, Kim JH, Lee JY, Park S, Shin G, Song JE, Lee MH, Kim S
Conflict of interest
No potential conflict of interest relevant to this article was reported.
1. Harandi TF, Taghinasab MM, Nayeri TD. The correlation of social support with mental health: a
meta-analysis. Electron Physician 2017;9(9):5212-5222.
3. Iliadis SI, Skalkidou A, Ranstrand H, Georgakis MK, Axfors C, Papadopoulos FC. Self-harm thoughts postpartum as a marker for long-term
morbidity. Front Public Health 2018;6:34
4. Wyunn KM, Than Wai ZZ, Ei Swe KE, Inthaphatha S, Nishino K, Yamamoto E. Factors associated with postpartum depression among Myanmar women
in Yangon: a cross-sectional study. Heliyon 2024;10(13):e33425.
5. Yaqoob H, Ju XD, Bibi M, Anwar S, Naz S. A systematic review of risk factors of postpartum depression.
Evidence from Asian culture. Acta Psychol 2024;249:104436
7. Hewitt CE, Gilbody SM, Brealey S, Paulden M, Palmer S, Mann R, et al. Methods to identify postnatal depression in primary care: an
integrated evidence synthesis and value of information
analysis. Health Technol Assess 2009;13(36):1-145.
8. Alshowkan A, Shdaifat E. Factors influencing postpartum depression in Saudi women: a
cross-sectional descriptive study. Womens Health Nurs 2024;30(2):164-173.
9. Çankaya S. The effect of psychosocial risk factors on postpartum depression
in antenatal period: a prospective study. Arch Psychiatr Nurs 2020;34(3):176-183.
10. Inthaphatha S, Yamamoto E, Louangpradith V, Takahashi Y, Phengsavanh A, Kariya T, et al. Factors associated with postpartum depression among women in
Vientiane Capital, Lao People's Democratic Republic: a
cross-sectional study. PLoS One 2020;15(12):e0243463.
11. Alshikh Ahmad H, Alkhatib A, Luo J. Prevalence and risk factors of postpartum depression in the
Middle East: a systematic review and meta–analysis. BMC Pregnancy Childbirth 2021;21:1-12.
12. Keser Özcan N, Boyacıoğlu NE, Dinç H. Postpartum depression prevalence and risk factors in Turkey: a
systematic review and meta-analysis. Arch Psychiatr Nurs 2017;31(4):420-428.
13. Upadhyay RP, Chowdhury R, Salehi A, Sarkar K, Singh SK, Sinha B, et al. Postpartum depression in India: a systematic review and
meta-analysis. Bull World Health Organ 2017;95(10):706-717C.
15. Tricco AC, Lillie E, Zarin W, O'Brien KK, Levac D, Peters MDJ, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and
explanation. Ann Intern Med 2018;169(7):467-473.
17. Zangmo S, Boonchieng W, Suvanayos C, Gyeltshen K, Siewchaisakul P. Prevalence and factors associated with postpartum depression
among Bhutanese mothers: a cross-sectional study. Womens Health Nurs 2024;30(3):238-249.
18. Guechhorng I, Inthaphatha S, Nishino K, Takahashi Y, Hamajima N, Yamamoto E. Determinants of postpartum depression among women in Kampong
Chhnang Province, Cambodia. Arch Psychiatr Nurs 2024;50:60-66.
19. Chen L, Shi Y. Analysis of influencing factors and the construction of
predictive models for postpartum depression in older pregnant
women. World J Psychiatry 2023;13(12):1079-1086.
20. He J, Li Y, Chen L, Zhang Y. Non-biological factors associated with postpartum depression
among women in Shenzhen: a case-control study. Front Public Health 2024;12:1417861
21. Liu Y, Guo N, Li T, Zhuang W, Jiang H. Prevalence and associated factors of postpartum anxiety and
depression symptoms among women in Shanghai, China. J Affect Disord 2020;274:848-856.
22. Liu Y, Zhang L, Guo N, Jiang H. Postpartum depression and postpartum post-traumatic stress
disorder: prevalence and associated factors. BMC Psychiatry 2021;21(1):487
23. Peng S, Lai X, Du Y, Meng L, Gan Y, Zhang X. Prevalence and risk factors of postpartum depression in China: a
hospital-based cross-sectional study. J Affect Disord 2021;282:1096-1100.
24. Xiong R, Deng A. Incidence and risk factors associated with postpartum depression
among women of advanced maternal age from Guangzhou, China. Perspect Psychiatr Care 2019;56(2):316-320.
25. Yi F, Ahn S. Effects of postpartum fatigue, parenting stress, and family
support on postpartum depression in Chinese first-time mothers: a
cross-sectional study. Womens Health Nurs 2024;30(3):226-237.
26. Begum S, Anitha S, Sushantha . A cross-sectional study on magnitude of post-partum depression
and factors associated with it among postnatal mothers visiting a tertiary
care setting in Mangalore, Karnataka. Indian J Public Health Res Dev 2024;15(3):371-377.
27. Murry LL, Devi YS, Joshi P, Dabas S, Kumari V, Singh KJ. Postpartum depression and its risk factors among Indian
women. Nurs J India 2020;111(4):186-190.
28. Priya T, Kaushal S, Dogra P, Dogra V. Prevalence and risk factors of postpartum depression in
sub-Himalayan region. Med J Armed Forces India 2024;80(2):161-165.
29. Yoo H, Ahn S, Park S, Kim J, Oh J, Koh M. Factors influencing prenatal and postpartum depression in Korea:
a prospective cohort study. Korean J Women Health Nurs 2021;27(4):326-336.
30. Labrague LJ, McEnroe-Petitte D, Tsaras K, Yboa BC, Rosales RA, Tizon MM, et al. Predictors of postpartum depression and the utilization of
postpartum depression services in rural areas in the
Philippines. Perspect Psychiatr Care 2019;56(2):308-315.
31. Alhusaini NA, Zarban NA, Shoukry ST, Alahmadi M, Gharawi NK, Arbaeyan R, et al. Prevalence of postpartum depression among mothers giving birth at
King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia from
2020 until 2022. Cureus 2022;14(11):e31365.
32. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item
Edinburgh postnatal depression scale. Br J Psychiatry 1987;150(6):782-786.
33. Bennett HA, Einarson A, Taddio A, Koren G, Einarson TR. Prevalence of depression during pregnancy: systematic
review. Obstet Gynecol 2004;103(4):698-709.
34. Lee DTS, Yip SK, Chiu HFK, Leung TYS, Chan KPM, Chau IOL, et al. Detecting postnatal depression in Chinese women: validation of
the Chinese version of the Edinburgh Postnatal Depression
Scale. Br J Psychiatry 1998;172(5):433-437.
35. Kim YK, Hur JW, Kim KH, Oh KS, Shin YC. Clinical application of Korean version of Edinburgh Postnatal
Depression Scale. J Korean Neuropsychiatr Assoc 2008;47(1):36-44.
36. Ing H, Fellmeth G, White J, Stein A, Simpson JA, McGready R. Validation of the Edinburgh Postnatal Depression Scale (EPDS) on
the Thai–Myanmar border. Trop Doct 2017;47(4):339-347.
37. Hanach N, Radwan H, Fakhry R, Dennis WB, Faris ME, Obaid RS, et al. Prevalence and risk factors of postpartum depression among women
living in the United Arab Emirates. Soc Psychiatry Psychiatr Epidemiol 2023;58(3):395-407.
39. Yu J, Zhang Z, Deng Y, Zhang L, He C, Wu Y, et al. Risk factors for the development of postpartum depression in
individuals who screened positive for antenatal depression. BMC Psychiatry 2023;23(1):557
40. Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for
screening to detect major depression among pregnant and postpartum women:
systematic review and meta-analysis of individual participant
data. Br Med J 2020;371:m4022
41. Engindeniz AN, Küey L, Kültür S. Turkish version of the Edinburgh Postpartum Depression Scale:
reliability and validity study. In. Psychiatric Organization of Türkiye editor. In: Proceedings of the Spring Symposiums I; 1996; Ankara (TR), Psychiatric Organization of Türkiye. 1996;p. 51-52.
42. Montazeri A, Torkan B, Omidvari S. The Edinburgh Postnatal Depression Scale (EPDS): translation and
validation study of the Iranian version. BMC Psychiatry 2007;7:11
44. Cox J. Thirty years with the Edinburgh Postnatal Depression Scale:
voices from the past and recommendations for the future. Br J Psychiatry 2019;214(3):127-129.
45. Kim O, Kim B, Kim SY, Cho E, Lee HY, Cha C, et al. Comparison of factors associated with postpartum depression from
two cohorts of nurses: the Korea Nurses' Health Study and the
Nurses' Health Study 3. Occup Environ Med 2023;80(4):209-217.
46. Honjo K, Kimura T, Baba S, Ikehara S, Kitano N, Sato T, et al. Association between family members and risk of postpartum
depression in Japan: does “who they live with” matter? -The
Japan environment and Children's study. Soc Sci Med 2018;217:65-72.
47. Peng S, Lai X, Qiu J, Du Y, Yang J, Bai Y, et al. Living with parents-in-law increased the risk of postpartum
depression in Chinese women. Front Psychiatry 2021;12:736306
49. Kim JH, Shin HS, Lee WH. Impact of endocrine-disrupting chemicals in breast milk on
postpartum depression in Korean mothers. Int J Environ Res Public Health 18;9:4444
50. Lamichhane DK, Jung DY, Shin YJ, Lee KS, Lee SY, Ahn K, et al. Association of ambient air pollution with depressive and anxiety
symptoms in pregnant women: a prospective cohort study. Int J Hyg Environ Health 2021;237:113823
Psychological intervention for postpartum depression: A systematic review and network meta-analysis Keke Qin, Dong Liu, Yong Yu, Renming Deng Journal of Affective Disorders.2026; 400: 121189. CrossRef
Predictive analysis of birth intention using machine learning Hyun Kyoung Kim Journal of Investigative Medicine.2026;[Epub] CrossRef
Prevalence and determinants of postpartum depression among new mothers attending a tertiary care hospital in Rawalpindi Pakistan Shaista Zulfiqar, Wania Khalid, Eleesha Shakeel, Kashaf Noor Ali, Fatima Ul Zahra, Tanzeela Rehman Discover Public Health.2026;[Epub] CrossRef
- Age range: 17−48
years - Included mothers with a history of psychiatric
disorders
4–8 weeks
Translated and pilot-tested
(n=30)
- ≥11 - Mean score of
suspected PPD: 14.17±3.44
47 (14.97%)
- Poor relationship with
friends/in-laws - Perceived changes in body image,
perceived increased stress during pregnancy, and perceived
stress after delivery - History of pregnancy
complications, negative delivery experience, and poor health
status of the newborn
- Mean age: 28.6 years -
Included mothers with a history of psychiatric
disorders - Mothers with singleton pregnancy, and no
thyroid disorders
6–8 weeks
Translated and pilot-tested
(n=11)
- ≥10 - Mean score:
6.65±4.27
133 (30.2%)
- Poor relationship with spouse and
mother-in-law - Dissatisfaction with economic status,
unplanned pregnancy, and spouse’s employment in manual
labor/farming/factory work
- Mean age of PPD mothers:
28.25±3.785 (vs 29.57±4.123 in non-PPD) -
Excluded history of psychiatric disorders, pregnancy
complications, and medical conditions
6–7 weeks
Chinese version
≥10
73 (14.5%)
- Co-habitation with in-laws -
Younger maternal age and history of pregnancy complications
- Mothers ≥18 years, with
healthy term births, and no postpartum complications - No
information on psychiatric history
6 weeks
Chinese version
- ≥13 - Mean score:
8.18±5.80
279 (23.2%)
- Lower familial support, lower social
support from colleagues or friends, mother-in-law as the primary
caregiver of mother and newborn, and dissatisfaction with
childbirth experiences - Lower level of education,
unplanned pregnancy, and lower economic status
- Mean age: 26.25±3.90 -
Excluded mothers with a history of psychiatric
disorders - Mothers with Primiparity, and no pregnancy
complications
6 weeks
Chinese version
- ≥10 - Mean score:
13.94±5.70
118 (78.7%)
- Gap between familial expectations
for fetal sex and actual sex of the newborn, poor relationship
with spouse, mother-in-law, and one’s parents -
Higher parenting stress, the gap between perceived and actual
family support - Younger maternal age, lower economic
status, and poor health condition of the newborn
- Mean age: 21.58±2.31 -
Excluded mothers with a history of psychiatric
disorders - Mothers with no abortions/ medical
terminations
6–8 weeks
No information on EPDS version
≥13
22 (33.8%)
- Living in an extended family
structure, pressure from the family to become pregnant, pressure
for a female child, and poor relationship with spouse, in-laws,
and one’s parents - Younger maternal age, lower
level of education, lower economic status, history of pregnancy
complications, multiple fetuses, and unplanned pregnancy
- Mean age: 28.1
(16−44) - Included mothers with a history of
psychiatric disorders - Mothers with a singleton
pregnancy, and no thyroid disorders
6–8 weeks
Translated and pilot-tested
(n=20)
- ≥10 - Mean score:
7.1±4.6
136 (31.8%)
- Poor relationship with spouse,
one’s parents, and mother-in-law - Dissatisfaction
with childbirth experiences - Higher education levels of
participants and spouses, unplanned pregnancy, multiparity,
housewife, and spousal unemployment
- Married mothers aged 18−49
years - Excluded mothers with a history of psychiatric
disorders
6 weeks
Arabic version
- ≥10 - Mean score:
2.54±4.5
15 (5.6%)
- Living in an extended family
structure - Lower level of education, spousal
unemployment, lower economic status, multiple fetuses, history
of pregnancy complications
- Mean age: 27.3±5.2 -
Mean age of PPD mothers: 28.2±5.2 (vs 27.2±5.2
non-PPD) - No information on psychiatric history -
Mothers with Primiparity and a singleton pregnancy
6–8 weeks
Turkish version
≥13
44 (18%)
- Increased marital conflict -
Increased perceived stress during pregnancy

 , Hyun Kyoung Kim2
, Hyun Kyoung Kim2