1Division of Cardiology, Department of Internal Medicine, Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
*Corresponding author: Hack-Lyoung Kim,
Division of Cardiology, Department of Internal Medicine, Boramae Medical Center,
Seoul National University College of Medicine, 5 Boramae-ro, Dongjak-gu, Seoul
07061, Korea, E-mail: khl2876@snu.ac.kr
• Received: February 26, 2024 • Revised: April 15, 2024 • Accepted: April 18, 2024
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Coronary artery disease (CAD) remains the leading cause of mortality worldwide,
driven primarily by atherogenesis. Recent efforts to understand sex differences
in CAD have revealed distinct patterns in disease burden, risk factors, and
clinical presentations. This review examines these sex differences in CAD,
underscoring the importance of customized diagnostic and management strategies.
Although men typically have higher rates of CAD prevalence and incidence, women
face unique challenges, such as delayed diagnosis, atypical symptoms, and lower
rates of medication prescription. Hormonal, genetic, and lifestyle factors all
play a role in these disparities, with estrogen notably reducing CAD risk in
women. Nontraditional risk factors, including chronic inflammation,
psychological stress, socioeconomic status, and reproductive history, also
contribute to CAD development and are often neglected in clinical settings.
Addressing these differences requires increased awareness, more accurate
diagnosis, and equitable healthcare access for both sexes. Furthermore, greater
inclusion of women in CAD research is essential to better understand
sex-specific mechanisms and optimize treatment outcomes. Personalizing CAD
management based on sex-specific knowledge has the potential to improve
prognosis and decrease disease incidence for both men and women.
Coronary artery disease (CAD) is the leading cause of death worldwide [1]. The formation of atherosclerotic
plaques, a process known as atherogenesis, is the primary factor in the
development of CAD [2]. Recent years have
seen a growing interest and active research into the sex differences observed in
various health conditions, including CAD. These differences are striking and
have become a focal point of scientific inquiry, highlighting the need for
disease prevention and treatment strategies that are tailored to sex-specific
characteristics [3]. To fully understand
CAD, it is essential to examine the influence of sex on its pathogenesis,
especially regarding atherogenesis. Studies have identified hormonal, genetic,
and lifestyle factors as contributors to the distinct patterns of disease
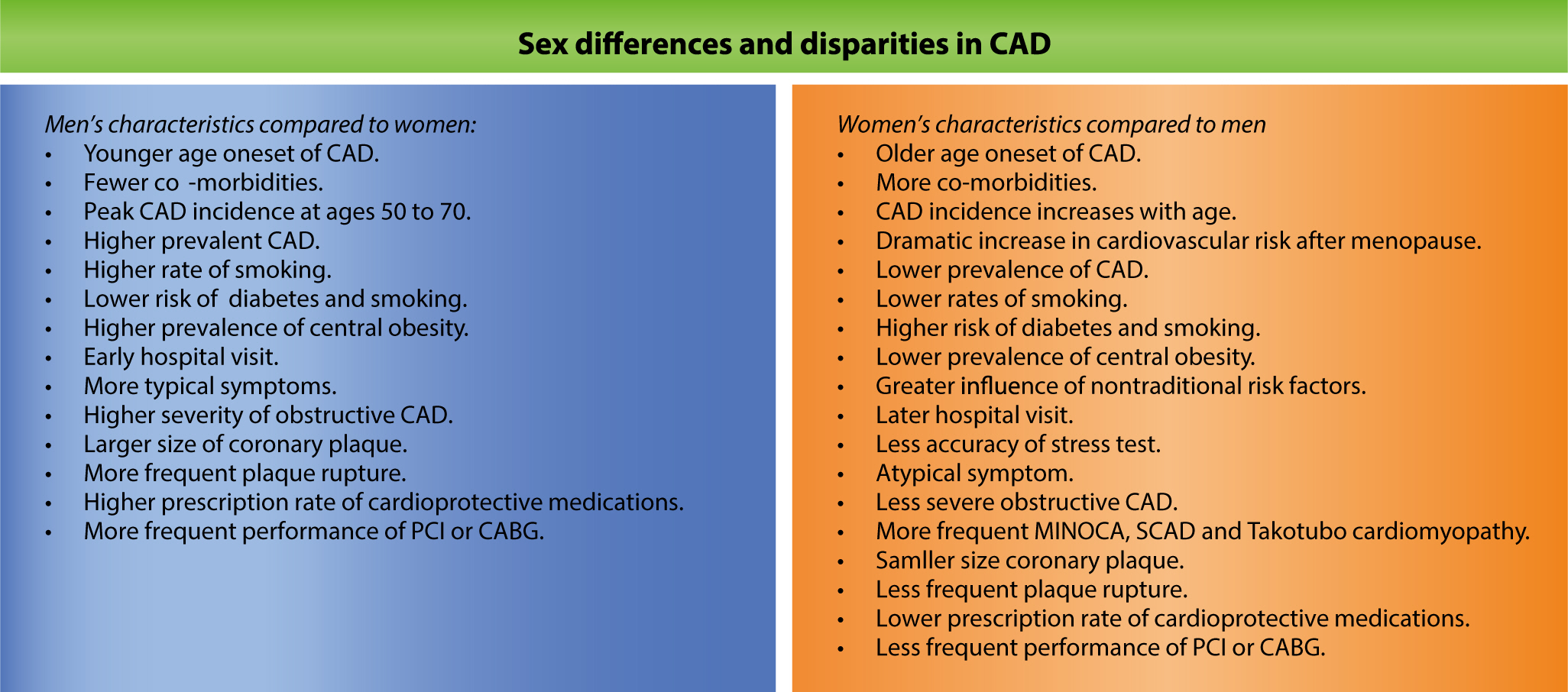
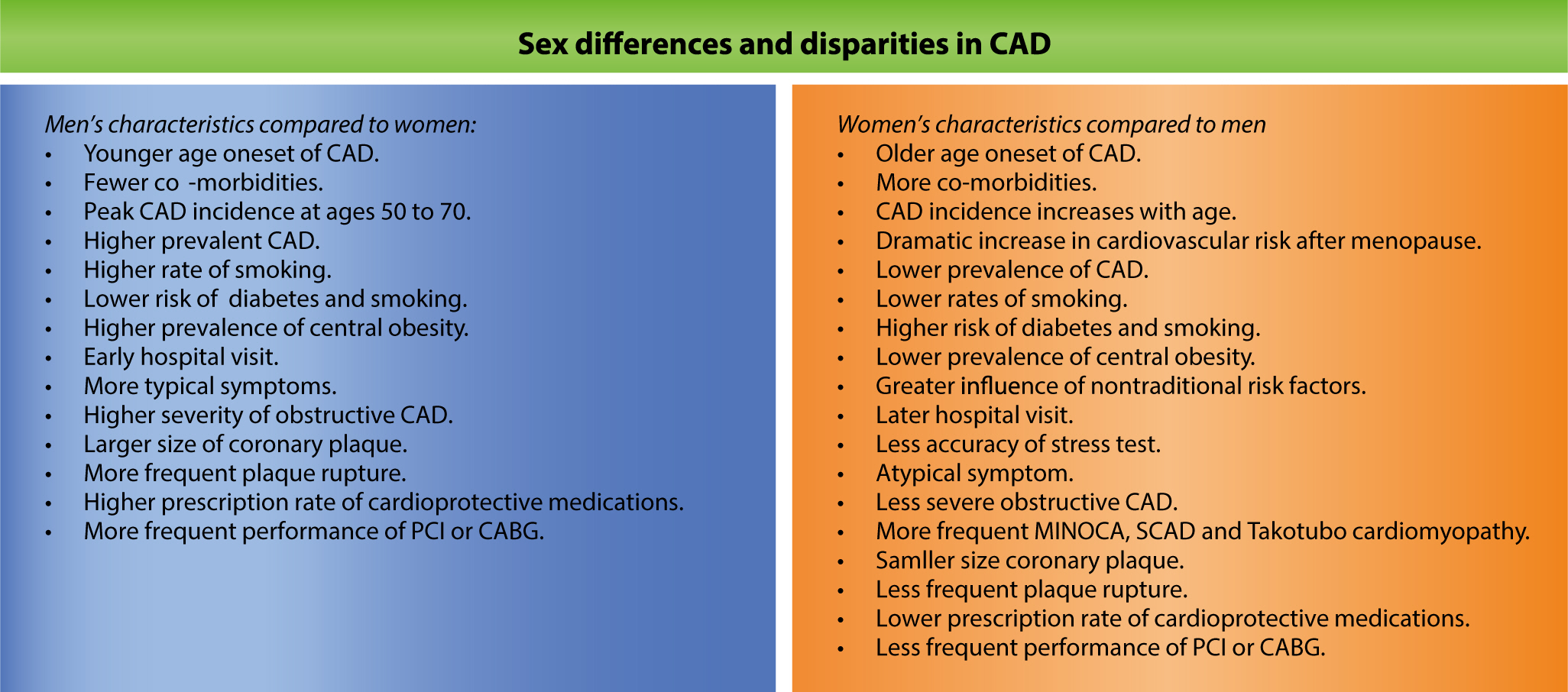
progression observed between men and women (Fig.
1).
Fig. 1.
Overview of sex differences and disparities in CAD. CAD, coronary
artery disease; PCI, percutaneous coronary intervention; CABG, coronary
artery bypass surgery; MINOCA, myocardial infarction with
non-obstructive coronary arteries; SCAD, spontaneous coronary artery
dissection.
Objectives
This review was conducted to examine the intricacies of sex differences in
coronary atherogenesis, providing a foundation for more effective and
personalized strategies in managing and preventing CAD. By highlighting the
specific needs and risks associated with each sex, healthcare providers can
better address the unique challenges presented by CAD, ultimately leading to
improved outcomes and a reduction in disease incidence [4].
Ethics statement
It is a literature database-based review; therefore, neither approval by the
institutional review board nor obtainment of informed consent was required.
Sex differences in coronary artery disease burden
Traditionally, men have exhibited a higher prevalence and incidence of CAD compared
to women. Data from the United States indicate that among all adults aged 20 years
and older, the prevalence of cardiovascular disease (CVD)—which includes CAD,
stroke, and heart failure—was 10.9% for men and 9.2% for women between 2017
and 2020 [1]. The age-adjusted CAD prevalence
in the United States in 2018 was 7.4% for men and 4.1% for women, according to the
Centers for Disease Control and Prevention. In a study of 141,459 Chinese
individuals, only 31.4% of those who underwent coronary angiography (CAG) for
suspected CAD were women, and among those who received percutaneous coronary
intervention (PCI), just 22.2% were women [5].
A Korean study that analyzed 633,907 patients hospitalized for acute myocardial
infarction (AMI) between 2002 and 2018 according to the Korean National Health
Insurance Claims Database found that women accounted for 40% of the cases [6]. Several studies examining CAG findings have
reported that obstructive lesions are more common and more severe in men than in
women [7]. While women typically experience
their first cardiovascular events later in life, the sex difference in CAD
prevalence and incidence diminishes with age [1]. A study of American adults from 2008 to 2017 found that the average
age of CAD onset was 57.4 years for men and 59.3 years for women [8]. Similarly, analyses of Korean patients who
underwent CAG for suspected CAD or PCI showed that the average age of female
patients was older than that of male patients [7,9]. According to 2021 data from
the Korean Statistical Information Service, men represented the majority of overall
AMI cases. However, the sex gap narrowed with age, and among individuals over 80
years old, the number of AMI cases in women was greater than that in men. In
American cohort analysis data, the incidence of CAD, which was significantly higher
in younger men, narrowed or even became similar to that in women aged 75 or older
[10].
Role of estrogen in coronary atherogenesis
The risk of developing CAD is high for men in their 40s to 70s. In contrast, for
women, the risk increases gradually with age and rises steeply from their 50s and
60s [11]. Based on analysis of the Framingham
cohort, in women, 40.3% of the impact of age on CVD was found to stem from
associated risk factors, greatly exceeding the 11.9% observed in men [12]. According to data from Korea’s 2013
National Health Insurance Service, men represented the majority of patients with CVD
until their 50s. However, this trend reversed in the 60–69-year range, and
among those in their 80s or older, 72.2% of cases were found in women and 27.8% in
men.
The increased risk of CAD in older women is closely related to the decrease in
systemic estrogen levels. Research suggests that the number of AMIs is negatively
associated with lifetime exposure to endogenous estrogen [13], while the later onset of menopause is linked to increased
life expectancy [14]. Although the exact
mechanisms are not yet fully understood, estrogen exerts several beneficial effects
on the cardiovascular system. Notably, this hormone promotes the relaxation of blood
vessel walls, leading to vasodilation [15].
This dilation helps to lower blood pressure and improve blood flow, thereby reducing
the cardiac workload. Additionally, estrogen has anti-inflammatory properties that
can reduce inflammation in the arteries and decrease the risk of atherosclerosis
[16]. Its antioxidant characteristics
enable it to neutralize harmful free radicals, thus reducing oxidative stress and
preventing damage to the walls of blood vessels and other cardiovascular tissues
[17]. Furthermore, estrogen influences
the distribution of body fat. After menopause, declining estrogen levels can lead to
an increased risk of abdominal obesity, which in turn promotes insulin resistance
and elevates cardiovascular risk [18].
Estrogen also improves cholesterol profile by increasing HDL cholesterol levels and
decreasing LDL levels [19]. This action helps
minimize the buildup of plaque in the arteries [20]. Additionally, estrogen supports the health and function of the
endothelium, the inner lining of blood vessels, which is crucial for regulating
blood vessel tone, preventing clot formation, and maintaining vascular health [21]. Overall, estrogen exerts cardioprotective
effects by mitigating the risk of atherosclerosis, hypertension, and thrombosis,
thereby reducing the likelihood of CVDs such as heart attack and stroke [22,23].
Sex differences in risk factors for coronary atherogenesis
Traditional risk factors
As previously mentioned, age is a primary determinant of coronary atherogenesis.
This factor exerts a more pronounced influence in women than in men,
particularly among older individuals [12].
In individuals under 65 years old, hypertension is more prevalent in men, whereas
among those over 65, the prevalence is higher in women. Women experience a
marked increase in systolic blood pressure after menopause, which can be
attributed to factors such as loss of estrogen, atherosclerosis, increased salt
sensitivity, decreased nitric oxide levels, and a rise in angiotensin II
receptors [24]. This leads to a higher
prevalence of isolated systolic hypertension in women, which is a substantial
risk factor for cardiovascular complications [24]. Overall, the influence of hypertension on the development of
CAD and stroke appears similar between sexes [25].
Studies indicate that diabetes mellitus presents a greater cardiovascular risk
for women than for men. Research involving both individuals without diabetes and
those with type 2 diabetes revealed a more pronounced increase in the risk of
coronary heart disease among women compared to men over a 13-year period [26]. Furthermore, a meta-analysis revealed
that relative to men with type 2 diabetes, women with the condition face a 46%
higher risk of mortality from coronary heart disease [27]. Another study reported that diabetes doubles the risk
of occlusive vascular mortality in men and triples it in women [28]. Consequently, intensified management
of cardiovascular risk is crucial for women with diabetes.
Women generally display higher levels of HDL cholesterol, whereas men are more
likely to have elevated levels of LDL cholesterol. However, after menopause,
women frequently see a rise in LDL cholesterol and a reduction in HDL
cholesterol, increasing their risk of CVD [29]. Although sex differences in the effects of dyslipidemia on CVD
are anticipated, the available data on this subject are scarce.
Like diabetes, smoking has a greater impact on the incidence of CAD in women than
men. A prospective cohort study found that the risk of AMI was 1.43-fold higher
in men who smoked, whereas in women, this risk was elevated by 2.24-fold [30]. Another study indicated that female
smokers experienced their first AMI earlier than male smokers [31]. To mitigate the risk of CVD, increased
attention should be directed toward women who smoke, and smoking cessation
education programs should be implemented.
The impact of obesity on the risk of developing CAD is slightly higher in men
than in women [32]. This may be
attributed to the higher prevalence of abdominal obesity in men, which further
elevates the risk of CVD [33]. However,
following menopause, the prevalence of abdominal obesity increases in women due
to estrogen depletion, with an associated increase in cardiovascular risk [18].
Nontraditional risk factors
Nontraditional risk factors, including chronic inflammation, psychological
stress, socioeconomic factors, and reproductive history, are known to influence
sex differences in CAD [34].
Chronic inflammation impairs endothelial cell function, amplifies oxidative
stress, and promotes vascular damage, which can lead to atherosclerosis [35]. Specifically, rheumatic diseases and
autoimmune diseases, which are more prevalent in women, can trigger CAD through
chronic inflammation [36].
Chronic stress elevates the secretion of stress hormones such as cortisol and
adrenaline, which in turn increases blood pressure, heart rate, and
inflammation. These physiological changes contribute to vascular damage and
thrombus formation [37]. Although stress
can induce CAD in both men and women, its effects are more pronounced in women
[38].
Women tend to have lower levels of education and income compared to men, and
these socioeconomic factors can contribute to the incidence of CAD. Lower
socioeconomic status in women can result in restricted access to healthcare
resources and preventive care for cardiovascular health [39].
Pregnancy-related factors, including gestational hypertension, preeclampsia,
gestational diabetes, miscarriage, stillbirth, and low birth weight, are also
associated with an increased risk of CAD [25,40]. Consequently, women
with these medical histories require more proactive management that extends
beyond childbirth [41].
Overall, these nontraditional risk factors are frequently overlooked and are not
sufficiently addressed in patient care relative to traditional factors. To
improve cardiovascular prognoses among women, efforts must be made to ensure
that these nontraditional risk factors are acknowledged and proactively managed
in the prevention and treatment of CAD.
Sex differences in coronary plaque
Atherosclerosis, the primary pathology underlying CAD, is an inflammatory process
driven by lipids that initiates the development of plaques within arterial walls
[35]. Endothelial dysfunction permits the
infiltration of LDL particles into the intima, which triggers an inflammatory
cascade. Adhesion molecules and cytokines facilitate the recruitment of inflammatory
cells such as monocytes, neutrophils, and T cells. Monocytes differentiate into
macrophages and form foam cells, which contribute to plaque formation. Vascular
smooth muscle cells migrate to the intima and establish a fibrous cap, which is
crucial for plaque stability. Phenotypic changes in these smooth muscle cells
further stabilize plaques through extracellular matrix production [35]. Endogenous sex hormones substantially
influence this process [42]. In women,
estrogen reduces the expression of adhesion molecules, the infiltration of
neutrophils, and the secretion of pro-inflammatory cytokines, thereby slowing the
progression of atherosclerosis. After menopause, the decline in estrogen levels
results in the loss of these protective effects. In comparison, men are more likely
to experience plaque rupture, leading to thrombus formation due to the rupture of
the fibrous cap and the exposure of thrombotic components. Plaques with thin fibrous
caps and large lipid cores are particularly vulnerable to rupture. Testosterone
appears to increase inflammatory cell infiltration and cytokine secretion, promoting
the development of atherosclerotic lesions [42]. Autopsy data from patients after sudden coronary death indicate
that men are more susceptible to the formation of blood clots and have a higher
incidence of ruptures. In contrast, women are less likely to develop thrombi, and
when they do, those thrombi are more likely to be associated with erosions [43]. Another study that analyzed the culprit
plaques in patients with myocardial infarction found that sex exerted a greater
influence on plaque characteristics than any other clinical feature [44].
Sex differences in clinical characteristics of patients with coronary artery
disease
Women with CAD typically present at an older age and with a greater number of
comorbidities than men. Notably, women often experience atypical angina symptoms,
which can complicate the diagnostic process [45]. Functional ischemic assessments and cardiac enzyme tests are
conducted less frequently in women, and these tests tend to be less accurate in
detecting CAD than in men. Furthermore, conditions such as myocardial infarction
with non-obstructive coronary arteries, spontaneous coronary artery dissection, and
Takotsubo cardiomyopathy are more prevalent among women [46]. In addition, women who undergo PCI face a higher risk of
bleeding complications than men [9].
Sex disparities in coronary artery disease
In comparison to men, women frequently delay seeking medical attention, often present
with atypical symptoms, and experience lower diagnostic accuracy. These factors lead
to comparatively late or missed diagnoses and subsequent delays in initiating
treatment [47]. Consequently, women are less
likely to undergo invasive procedures such as PCI or coronary artery bypass graft
surgery compared to men [48]. Furthermore, a
sex-based disparity is evident in the prescription rates of cardioprotective drugs.
Relative to men, women are less frequently prescribed essential medications such as
antiplatelets, renin-angiotensin system blockers, and statins, which are crucial for
managing CVD [49]. Moreover, women are
significantly underrepresented in clinical research related to CAD [50]. These sex disparities ultimately lead to
poorer cardiovascular prognoses among women.
Future directions
As mentioned above, sex differences are evident in the pathophysiology, risk factors,
clinical manifestations, and treatment responses of CAD, as well as in diagnostic
and therapeutic approaches. However, most clinical studies have not collected data
on female-specific risk factors, such as pregnancy history, age at menopause, and
polycystic ovary syndrome, and have not included this information in their analyses.
Historically, clinical research has been male-dominated, with women frequently
excluded due to factors related to fertility, breastfeeding, or menopause [51]. Awareness must be raised of these sex
differences and disparities, not only among healthcare professionals but also within
the general population. A survey of middle-aged and elderly women in Korea revealed
a very low level of awareness regarding heart disease in women [52]. The “Go Red for Women”
campaign, initiated by the American Heart Association in 2004, has raised awareness
of CVD in women and effectively reduced cardiovascular mortality within this
population, highlighting the impact of such awareness campaigns [53,54].
Furthermore, knowledge of sex-based differences must be integrated into clinical
guidelines [34]. To conduct sex-specific
analyses with sufficient statistical power, the anticipated number of patients must
be at least doubled. However, creating separate guidelines for each sex presents
several challenges and can be both complex and impractical. A more feasible approach
in clinical practice is to address sex differences within a unified set of
guidelines. In many developed Western countries, CAD recommendations consistently
underscore the importance of considering sex differences. For instance, guidelines
from these countries often highlight the need for cardiovascular care for women
after childbirth [55]. Clinicians and
researchers should be cognizant of these differences and routinely assess them in
their clinical work and research endeavors. By establishing guidelines grounded in
robust evidence, and by increasing the inclusion of women in randomized trials and
conducting comprehensive analyses of sex differences, high-quality evidence can be
progressively amassed and reflected in future recommendations [56].
Conclusion
Stark differences exist between men and women in terms of CAD burden, risk factors,
plaque characteristics, and clinical features. These distinctions highlight the need
for tailored diagnostic and therapeutic approaches for CAD in both sexes. It is also
essential to recognize the longer diagnostic timelines, delays in
procedures/surgery, and lower rates of medication prescriptions in women. Addressing
these issues requires an increased awareness of sex differences and discrimination,
as well as greater inclusion of women in clinical research to gather more complete
data on women’s cardiovascular health.
Authors' contributions
All work was done by Hack-Lyoung Kim.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, et al. Heart disease and stroke statistics—2023 update: a report
from the American Heart Association. Circulation 2023;147(8):e93-e621.
3. Vogel B, Acevedo M, Appelman Y, Noel Bairey Merz C, Chieffo A, Figtree GA, et al. The Lancet women and cardiovascular disease
commission: reducing the global burden by 2030. Lancet 2021;397(10292):2385-2438.
4. Mosca L, Barrett-Connor E, Wenger NK. Sex/gender differences in cardiovascular disease prevention: what
a difference a decade makes. Circulation 2011;124(19):2145-2154.
5. Chen SQ, Liu J, Zhou Y, Huang ZD, Xie Y, Huang HZ, et al. Sex differences in characteristics, treatments, and in-hospital
outcomes of patients undergoing coronary angiography or
intervention. Front Cardiovasc Med 2022;9:878566
6. Kim SR, Bae SA, Lee JY, Kim MS, Kim MN, Chung WJ, et al. Gender disparities in prevalence by diagnostic criteria,
treatment and mortality of newly diagnosed acute myocardial infarction in
Korean adults. Sci Rep 2023;13(1):4120
7. Kim HL, Kim HJ, Kim M, Park SM, Yoon HJ, Byun YS, et al. Sex differences in coronary angiographic findings in patients
with stable chest pain: analysis of data from the KoRean wOmen'S
chest pain rEgistry (KoROSE). Biol Sex Differ 2022;13(1):2
8. Okunrintemi V, Tibuakuu M, Virani SS, Sperling LS, Volgman AS, Gulati M, et al. Sex differences in the age of diagnosis for cardiovascular
disease and its risk factors among US adults: trends from 2008 to 2017, the
medical expenditure panel survey. J Am Heart Assoc 2020;9(24):e018764.
9. Kim HL, Jang JS, Kim MA, Seo JB, Chung WY, Kim SH, et al. Gender differences of in-hospital outcomes in patients undergoing
percutaneous coronary intervention in the drug-eluting stent
era. Medicine 2019;98(20):e15557.
10. Madhavan MV, Gersh BJ, Alexander KP, Granger CB, Stone GW. Coronary artery disease in patients ≥80 years of
age. J Am Coll Cardiol 2018;71(18):2015-2040.
13. Saltiki K, Doukas C, Kanakakis J, Anastasiou E, Mantzou E, Alevizaki M. Severity of cardiovascular disease in women: relation with
exposure to endogenous estrogen. Maturitas 2006;55(1):51-57.
14. Ossewaarde ME, Bots ML, Verbeek AL, Peeters PH, van der Graaf Y, Grobbee DE, et al. Age at menopause, cause-specific mortality and total life
expectancy. Epidemiology 2005;16(4):556-562.
15. Somani YB, Pawelczyk JA, De Souza MJ, Kris-Etherton PM, Proctor DN. Aging women and their endothelium: probing the relative role of
estrogen on vasodilator function. Am J Physiol Heart Circ Physiol 2019;317(2):H395-H404.
17. Niranjan MK, Koiri RK, Srivastava R. Expression of estrogen receptor alpha in response to stress and
estrogen antagonist tamoxifen in the shell gland of Gallus
gallus domesticus: involvement of anti-oxidant system and
estrogen. Stress 2021;24(3):261-272.
18. Janssen I, Powell LH, Kazlauskaite R, Dugan SA. Testosterone and visceral fat in midlife women: the Study of
Women's Health Across the Nation (SWAN) fat patterning
study. Obesity 2010;18(3):604-610.
20. Burke AP, Farb A, Malcom G, Virmani R. Effect of menopause on plaque morphologic characteristics in
coronary atherosclerosis. Am Heart J 2001;141(2):S58-S62.
21. Taddei S, Virdis A, Ghiadoni L, Mattei P, Sudano I, Bernini G, et al. Menopause is associated with endothelial dysfunction in
women. Hypertension 1996;28(4):576-582.
23. Iorga A, Cunningham CM, Moazeni S, Ruffenach G, Umar S, Eghbali M. The protective role of estrogen and estrogen receptors in
cardiovascular disease and the controversial use of estrogen
therapy. Biol Sex Differ 2017;8(1):33
25. Appelman Y, van Rijn BB, ten Haaf ME, Boersma E, Peters SAE. Sex differences in cardiovascular risk factors and disease
prevention. Atherosclerosis 2015;241(1):211-218.
26. Juutilainen A, Kortelainen S, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Gender difference in the impact of type 2 diabetes on coronary
heart disease risk. Diabetes Care 2004;27(12):2898-2904.
27. Huxley R, Barzi F, Woodward M. Excess risk of fatal coronary heart disease associated with
diabetes in men and women: meta-analysis of 37 prospective cohort
studies. BMJ 2006;332(7533):73-78.
28. Gnatiuc L, Herrington WG, Halsey J, Tuomilehto J, Fang X, Kim HC, et al. Sex-specific relevance of diabetes to occlusive vascular and
other mortality: a collaborative meta-analysis of individual data from 980
793 adults from 68 prospective studies. Lancet Diabetes Endocrinol 2018;6(7):538-546.
29. Abbey M, Owen A, Suzakawa M, Roach P, Nestel PJ. Effects of menopause and hormone replacement therapy on plasma
lipids, lipoproteins and LDL-receptor activity. Maturitas 1999;33(3):259-269.
30. Prescott E, Hippe M, Schnohr P, Hein HO, Vestbo J. Smoking and risk of myocardial infarction in women and men:
longitudinal population study. BMJ 1998;316(7137):1043-1047.
31. Grundtvig M, Hagen TP, German M, Reikvam A. Sex-based differences in premature first myocardial infarction
caused by smoking: twice as many years lost by women as by
men. Eur J Cardiovasc Prev Rehabil 2009;16(2):174-179.
34. Kim HL, Kim MA. Sex differences in coronary artery disease: insights from the
KoRean wOmen'S chest pain rEgistry (KoROSE). Korean Circ J 2023;53(10):655-676.
38. Vaccarino V, Sullivan S, Hammadah M, Wilmot K, Al Mheid I, Ramadan R, et al. Mental stress–induced-myocardial ischemia in young
patients with recent myocardial infarction: sex differences and
mechanisms. Circulation 2018;137(8):794-805.
39. Backholer K, Peters SAE, Bots SH, Peeters A, Huxley RR, Woodward M. Sex differences in the relationship between socioeconomic status
and cardiovascular disease: a systematic review and
meta-analysis. J Epidemiol Community Health 2017;71(6):550-557.
40. Kelly AC, Michos ED, Shufelt CL, Vermunt JV, Minissian MB, Quesada O, et al. Pregnancy and reproductive risk factors for cardiovascular
disease in women. Circ Res 2022;130(4):652-672.
41. Søndergaard MM, Hlatky MA, Stefanick ML, Vittinghoff E, Nah G, Allison M, et al. Association of adverse pregnancy outcomes with risk of
atherosclerotic cardiovascular disease in postmenopausal
women. JAMA Cardiol 2020;5(12):1390-1398.
42. Yerly A, van der Vorst EPC, Baumgartner I, Bernhard SM, Schindewolf M, Döring Y. Sex-specific and hormone-related differences in vascular
remodelling in atherosclerosis. Eur J Clin Invest 2023;53(1):e13885.
43. Yahagi K, Davis HR, Arbustini E, Virmani R. Sex differences in coronary artery disease: pathological
observations. Atherosclerosis 2015;239(1):260-267.
44. Arbustini E, Dal Bello B, Morbini P, Burke AP, Bocciarelli M, Specchia G, et al. Plaque erosion is a major substrate for coronary thrombosis in
acute myocardial infarction. Heart 1999;82(3):269-272.
45. Cho DH, Choi J, Kim MN, Kim HL, Kim YH, Na JO, et al. Gender differences in the presentation of chest pain in
obstructive coronary artery disease: results from the Korean Women's
Chest Pain Registry. Korean J Intern Med 2020;35(3):582-592.
47. Kaul P, Armstrong PW, Sookram S, Leung BK, Brass N, Welsh RC. Temporal trends in patient and treatment delay among men and
women presenting with ST-elevation myocardial infarction. Am Heart J 2011;161(1):91-97.
48. Daly C, Clemens F, Lopez Sendon JL, Tavazzi L, Boersma E, Danchin N, et al. Gender differences in the management and clinical outcome of
stable angina. Circulation 2006;113(4):490-498.
49. Zhao M, Woodward M, Vaartjes I, Millett ERC, Klipstein‐Grobusch K, Hyun K, et al. Sex differences in cardiovascular medication prescription in
primary care: a systematic review and meta‐analysis. J Am Heart Assoc 2020;9(11):e014742.
50. Agarwala A, Goldberg A. Special considerations for lipid-lowering therapy in women
reflecting recent randomized trials. Curr Atheroscler Rep 2021;23(8):42
51. Whitelaw S, Sullivan K, Eliya Y, Alruwayeh M, Thabane L, Yancy CW, et al. Trial characteristics associated with under-enrolment of females
in randomized controlled trials of heart failure with reduced ejection
fraction: a systematic review. Eur J Heart Fail 2021;23(1):15-24.
52. Kim HJ, Kim HY, Kim HL, Park SM, Cho DH, Kim M, et al. Awareness of cardiovascular disease among Korean women: results
from a nationwide survey. Prev Med Rep 2022;26:101698
53. Mosca L, Hammond G, Mochari-Greenberger H, Towfighi A, Albert MA. Fifteen-year trends in awareness of heart disease in women:
results of a 2012 American Heart Association national survey. Circulation 2013;127(11):1254-1263.
54. Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics—2018 update: a report
from the American Heart Association. Circulation 2018;137(12):e67-e492.
55. Smith GN, Louis JM, Saade GR. Pregnancy and the postpartum period as an opportunity for
cardiovascular risk identification and management. Obstet Gynecol 2019;134(4):851-862.
Diagnostic Performance of a Novel AI–Guided Coronary Computed Tomography Algorithm for Predicting Myocardial Ischemia (AI-QCTISCHEMIA) Across Sex and Age Subgroups Putri Annisa Kamila, Tara Hojjati, Nick S. Nurmohamed, Ibrahim Danad, Yipu Ding, Ruurt A. Jukema, Pieter G. Raijmakers, Roel S. Driessen, Michiel J. Bom, Pepijn van Diemen, Gianluca Pontone, Daniele Andreini, Hyuk-Jae Chang, Richard J. Katz, Andrew D. Cho Journal of the Society for Cardiovascular Angiography & Interventions.2026; 5(2): 104064. CrossRef
Factors associated with all-cause mortality in endovascularly treated patients with chronic limb-threatening ischemia Mária Rašiová, Veronika Pavlíková, Marek Hudák, Viktor Kožár, Lucia Dekanová Frontiers in Epidemiology.2026;[Epub] CrossRef
Trends in Sepsis-Associated Respiratory Disease Mortality in the United States, 1999 to 2023 Qais Bin Abdul Ghaffar, Khawaja Omar, Zoha Khan, Talha Adil, Mujtaba Azhar Siddiqui, Arbab Burhanuddin Kasi, Imran Khawaja Journal of Intensive Care Medicine.2026;[Epub] CrossRef
High-Sensitivity C-reactive Protein as a Predictive Biomarker of Coronary Artery Disease Severity: A Cross-Sectional Study in Bangladesh Md. Maruf-Ur- Rahman, Md. Rafiqul Islam, Wazeda Begum, Md. Musaddequl Alam, Md. Fakhrul Islam Khaled, A. H. M. Golam Kibria Cureus.2026;[Epub] CrossRef
Higher Dietary Antioxidant Index Is Associated with Better Lipid Profile in Women with Coronary Artery Disease Mariana Moya-García, Wendy Campos-Pérez, Mariana Pérez-Robles, Sissi Godínez-Mora, Sarai Citlalic Rodríguez-Reyes, Liliana Estefanía Ramos-Villalobos, Erika Martínez-López Healthcare.2026; 14(8): 1085. CrossRef
A cross-sectional study on the prevalence of cardiometabolic diseases and their multilevel socioeconomic impacts in Qianxinan Buyi and Miao Autonomous Prefecture, Southwest China Lianyue Wu, Yanjun Long, Xin Zou, Li Ren, Kuaifa Fang Medicine.2026; 105(23): e49109. CrossRef
Difference of Coronary Artery Disease in Women and Men in Recent Trials Geetha Subramanian, Pavithra Muthusamy, Thiagarajan Kaliyamurthy, Manohar Ganesan Indian Journal of Cardiovascular Disease in Women.2025; 10: 131. CrossRef
Mortality patterns of coronary artery diseases and atrial fibrillation in adults in the United States from 1999 to 2022: An analysis using CDC WONDER Muzamil Akhtar, Muhammad Hamza Dawood, Muheem Khan, Muhammad Raza, Mehmood Akhtar, Sultana Jahan, Matthew Bates, Aneesh Challa, Raheel Ahmed, Abdul Khaliq Naveed, Yasar Sattar The American Journal of the Medical Sciences.2025; 370(1): 59. CrossRef
Interaction between triglyceride-glucose-body mass index and age in coronary artery stenosis severity: a sex-stratified exploratory analysis Pingxiong Zeng, Jingdan Deng, Yuting Zhong, Liping Zhong, Yuanjun Zhou, Yilin Liao, Zhiyan Xu BMC Cardiovascular Disorders.2025;[Epub] CrossRef
Trends and Disparities in Mortality due to Diabetes Mellitus and Sepsis in the US Adults: 1999–2023 Asad Gul Rao, Sufyan Shahid, Neha Pervez, Ramsha Pervez, Raheel Ahmed Endocrinology, Diabetes & Metabolism.2025;[Epub] CrossRef
A Multi-Biomarker Approach to Increase the Accuracy of Diagnosis and Management of Coronary Artery Disease Lenka Hostačná, Jana Mašlanková, Dominik Pella, Beáta Hubková, Mária Mareková, Daniel Pella Journal of Cardiovascular Development and Disease.2024; 11(9): 258. CrossRef