1Department of Dermatology, Jeonbuk National University Medical School, Jeonju, Korea
2Department of Dermatology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea
3Department of Dermatology, Uijeongbu St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea
4Department of Dermatology, Incheon St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea
5Department of Dermatology, Korea University Guro Hospital, Seoul, Korea
6Department of Dermatology, Inha University Hospital, Incheon, Korea
*Corresponding author: Gwang Seong
Choi, Department of Dermatology, Inha University Hospital, 27 Inhangro, Jung-gu,
Incheon 22332, Korea, E-mail: garden@inha.ac.kr
*This is a secondary publication of Park J, Kwon SH, Lee YB, Kim HS, Jeon JH,
Choi GS. Clinical Practice Guidelines for the Diagnosis and Treatment of
Scabies in Korea: Part 2. Treatment and Prevention. Korean J
Dermatol 2023;61(8):463-471 under the permission of the editor
of the Korean Journal of Dermatology after English
translation.
• Received: October 13, 2024 • Accepted: October 13, 2024
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Treatment should be initiated for all suspected, clinical, or confirmed cases of
scabies. Patients affected should be adequately isolated, and high-risk groups
with close contact histories should be treated regardless of their symptoms.
Optimal treatment strategies can be selected based on age, clinical subtype, and
the patient's health status. In Korea, commercially available
preparations for scabies treatment include topical 5% permethrin, topical 10%
crotamiton, and oral ivermectin. Topical 5% permethrin is the first-line
selective treatment for both classic and crusted scabies. Alternative treatments
include topical 10% crotamiton and oral ivermectin. After completing treatment,
follow-up visits at 2 and 4 weeks are recommended to monitor the therapeutic
response. Treatment is considered to have failed if scabies mites or burrows are
detected, new clinical characteristics develop, or there is an aggravation of
pruritus. Scabies itch should be adequately managed with emollients, oral
antihistamines, and topical corticosteroids. Preventive measures, including
personal hygiene, patient education, and environmental control, should besd
implemented to reduce the transmission of scabies.
- Treatment for scabies should be chosen based on factors such as age,
clinical form, and overall health status. Additionally, close contacts
should be treated simultaneously with the patient, irrespective of symptom
presence.
- Topical 5% permethrin is the first-line treatment for both classic and
crusted scabies. When the use of topical 5% permethrin is not feasible,
alternative treatments include topical 10% crotamiton or oral
ivermectin.
- Treatment is deemed unsuccessful if there is an exacerbation of pruritus,
the emergence of new characteristic skin lesions such as burrows, or if
mites continue to be detected after the treatment.
When selecting an appropriate treatment for scabies infestation, it is important to
consider factors such as the patient's age, the clinical form of the disease,
and overall health status. Treatment should be administered simultaneously to both
the patient and any close contacts, including family members living in the same
household and facility staff, regardless of whether they show symptoms. In Korea,
the available scabicidal treatments include topical 5% permethrin cream, 10%
crotamiton ointment, and oral ivermectin (Table
1, Supplement
1). Although 5%–10% sulfur ointments are not commercially available
within the country, they can be specially prepared or imported as needed. Topical 5%
permethrin is the first-line treatment for both classic and crusted scabies. If the
use of topical 5% permethrin is not feasible, alternative options include 10%
crotamiton ointment or oral ivermectin.
Table 1.
Drugs available in Korea for the treatment of scabies
Drug (product)
FDA approval for scabies treatment
Domestic approval (class)
Usage (dosing)
Topical 5% permethrin (Omeclean, 30 g
cream/tube)
Yes
Yes (prescription drug)
- Adult: 25–30 g (1 tube) -
6–12 years: 15 g (1/2 tube) - 2 months–5 years:
up to 7.5 g (1/4 tube)
Topical 10% crotamiton (Uracin, 50 g
ointment/tube)
Yes (only for adults)
Yes (over-the counter drug)
Adult: 25–30 g (1/2 tube)
Oral ivermectin (Stromectol, 3
mg/tablet)
No
No (orphan drug) Indication in
KOEDC - Failure or nonadherent to topical
treatment - Widespread institutional outbreaks
FDA, Food and Drug Administration; KOEDC, Korea Orphan & Essential
Drug Center.
Treatment of classic scabies
Topical 5% permethrin
Permethrin, approved by the U.S. Food and Drug Administration (FDA) for use
in individuals aged two months and older (approved for ages two years and
older in Korea), is typically the first-line treatment for scabies. It
effectively targets all life stages of the scabies mite, including eggs, and
has been shown to be more efficacious than oral ivermectin [1]. Although a single application might
theoretically be sufficient to reduce the risk of treatment failure, it is
recommended to apply permethrin twice, one week apart, and to schedule a
follow-up visit two weeks after the initial treatment to confirm
eradication. Generally, the application should remain on the skin for at
least 8–12 hours; however, an in vitro study
suggested that maintaining 5% permethrin on the skin for only 8 hours may
not fully eradicate the mites [2].
Therefore, it is advisable to wait approximately 12 hours post-application
before washing. Studies in the early 2000s reported an approximate 95%
efficacy of 5% permethrin, while a 2020 survey in Germany indicated an
efficacy rate ranging from 80% to 100% [3]. However, more recent studies in Austria and other regions
have reported lower treatment efficacy than previously observed [4,5]. Although permethrin-resistant scabies mites have not been
definitively identified, an increase in cases suspected to involve treatment
resistance highlights the need for caution.
Topical 10% crotamiton
Crotamiton has received approval from the U.S. FDA for the treatment of
scabies infections in adults, boasting an efficacy rate of about 60%. The
typical regimen involves daily application for 3 to 5 days (e.g., on days 1,
2, 3, and 8), with each application left on the skin for 8 hours. Due to its
relatively lower efficacy and instances of treatment failure, crotamiton is
generally used as a secondary option when first-line treatments, such as
topical permethrin or oral ivermectin, are not suitable. Crotamiton is
favored in clinical practice for pediatric patients due to its minimal skin
irritation and anti-itch properties. In Korea, its use is also sanctioned
for children, though it is advised to limit extensive application in infants
and young children.
Topical 5%–10% sulfur
Sulfur is considered safe for use in infants under two months of age and in
pregnant women. It is typically applied nightly over three consecutive days,
with the final application being washed off the next day. However, its
unpleasant odor and propensity to stain may deter its use. While
sulfur-based formulations are not commercially available in Korea, they can
be self-prepared or imported for use.
Topical 1% lindane
Lindane was previously approved by the U.S. FDA; however, it is no longer
produced or used due to concerns over neurotoxicity.
Oral ivermectin
Ivermectin, introduced in 1981, remains the sole oral medication for treating
scabies, with a half-life of 12–56 hours. Although the FDA has
approved it for treating other parasitic infections such as strongyloidiasis
and onchocerciasis in the U.S., clinical experience has also established its
safety and efficacy for scabies. In 2001, France authorized the use of
ivermectin for managing scabies outbreaks in institutional settings. It is
typically employed when the first-line topical treatment, permethrin, is
unsuitable or ineffective. In Korea, ivermectin is imported under the brand
name Stromectol and is classified as an orphan drug, necessitating specific
administrative procedures for its prescription in hospitals (Supplement 2).
Ivermectin does not eliminate scabies eggs. Therefore, for classic scabies, a
dosage of 200 µg/kg is administered twice, 1–2 weeks apart, to
coincide with the mite's life cycle. This is followed by an
evaluation of the treatment's efficacy. Taking ivermectin with food
increases its absorption [6]. Its
safety in children under 15 kg and pregnant women has not been confirmed,
although serious side effects are rare in infants and pregnant women who
have taken it [7,8]. Consequently, it may be considered when other
treatments are either unavailable or have failed. While some practices
combine oral ivermectin with topical agents, the effectiveness and evidence
supporting this combined approach in the treatment of classic scabies have
not yet been conclusively established.
Treatment of crusted scabies
- The medications used to treat crusted scabies are similar to those for
classic scabies; however, the frequency of application and dosage may
differ.
- Due to is high transmissibility, isolation is recommended to prevent
the risk of spreading the infection.
- While some cases of scabies are treated solely with topical permethrin,
in countries where oral ivermectin is accessible and approved, it is
often used concurrently. For crusted scabies that is resistant to
topical permethrin alone, a combination of oral ivermectin and topical
treatments may be considered. However, there are currently no
standardized guidelines regarding the frequency and intervals of topical
applications or their combination with oral medications for treating
crusted scabies. Typically, permethrin ointment is applied daily for one
week and then twice weekly until no mites or eggs are detected [9]. Ivermectin is administered on
days 0, 1, 7, 8, and 14, with optional additional doses on days 21 and
28 [7]. The treatment regimens for
ivermectin are categorized into three phases based on the severity of
the symptoms of crusted scabies: Phase 1 includes days 0, 1, and 7;
Phase 2 includes days 0, 1, 7, 8, and 14; Phase 3 includes days 0, 1, 7,
8, 14, 21, and 28 [8].
- The removal of the thick crust associated with crusted scabies aids in
treatment. Consequently, keratolytic agents such as 5%–10%
salicylic acid, 10% urea, and 5% lactic acid, which are not typically
used in treating classic scabies, can be employed to enhance drug
penetration and improve treatment efficacy.
- If secondary bacterial infections with organisms such as
Streptococcus pyogenes or Staphylococcus
aureus are present, appropriate antibiotics should be
administered [9].
Precautions in scabies treatment
- Simultaneously treat individuals who have been in contact with or are
cohabitating with a scabies patient.
- For classic scabies, thoroughly apply the medication from the neck down
to the feet, covering all skin areas. This includes under the nails and
in skin folds, such as the groin. After applying the medication, it
should remain on the skin for an adequate period (at least 8 hours)
before it is washed off.
- For infants, young children, and certain older adults with scalp or
facial involvement, the treatment should be applied over the entire
body, including the face and scalp.
- Wearing plastic gloves during application is recommended, as excessive
absorption of the medication through the palms can cause numbness,
tingling, or a stinging sensation.
Treatment failure
Typically, itching from scabies subsides about three days after the application
of scabies treatment. However, if itching persists or worsens without
improvement, initially improves but then intensifies again, or if new burrows or
skin lesions emerge, or mites are still detected within 7–14 days
post-treatment, treatment failure should be considered. It is important to note,
however, that persistent itching alone should not be immediately considered a
sign of treatment failure. Itching may continue for several weeks due to
hypersensitivity reactions to the mites or their waste products, even after all
mites have been eliminated.
Common causes of treatment failure include improper treatment, continued close
contact with untreated infected individuals, inadequate disinfection of clothing
and bedding, and the use of topical steroids during treatment. Drug resistance
is also suspected as a potential factor. Treatment failure can occur even with
highly effective ointments if the treatment is not applied thoroughly or if
instructions are not followed carefully. However, if instructions are followed
diligently and the medication is applied thoroughly, most cases of recurrence
are due to reinfection from untreated carriers of scabies [10].
Treatment for children, pregnant women, and institutional outbreaks
Children
Permethrin is approved by the FDA as a first-line treatment for children over
2 months old and has well-established safety data. However, in Korea, it is
only approved for use in children aged 2 years and older [6,11]. For children, unlike adults, the application should cover
all areas of the body except around the eyes and mouth, including the face
[12]. Crotamiton may be
considered a second-line treatment, although it is less effective and
requires a longer treatment duration than permethrin [13]. Sulfur ointment is safe for use in very young
infants under 2 months old; however, it is not commercially available in
Korea. Lindane is contraindicated in children [5]. The safety of ivermectin has not been established
for children weighing less than 15 kg [6].
Pregnant and breastfeeding women
Permethrin is considered safe for use in pregnant and breastfeeding women and
is recommended as a first-line treatment by the Centers for Disease Control
and Prevention (CDC) [6]. However, it
is not approved for use in pregnant and breastfeeding women in Korea.
Therefore, it is important to adhere strictly to the recommended dosage and
application guidelines to avoid any potential risks. When applied, less than
2% of the permethrin dose is absorbed systemically [14]. While it is unclear whether permethrin is excreted
into breast milk, it is advisable to pause breastfeeding for five days after
its application. Sulfur ointment is also considered safe for pregnant and
breastfeeding women, but it is not commercially available in Korea. Lindane,
on the other hand, is contraindicated for use in pregnant and breastfeeding
women [15]. The safety of ivermectin
during pregnancy has not yet been established [6].
Treatment in institutional outbreaks
Mass treatment for scabies is recommended in areas where it is endemic or for
managing outbreaks in closed community settings [7]. In situations involving suspected transmission
within a community or institution, such as healthcare facilities or nursing
homes, it is advisable to treat all individuals at risk, regardless of
whether they exhibit symptoms. Oral ivermectin is the preferred option for
mass treatments due to its ease of administration compared to topical
treatments. Typically, a single dose of oral ivermectin is administered at
200 µg/kg [16], and evidence
suggests that a second dose one week later may improve treatment efficacy
(Table 2) [17].
Table 2.
Summary of drugs for scabies treatment in children, pregnant and
breastfeeding women
Drugs
Use in children
Use in pregnancy
Use in breastfeeding
Topical 5% permethrin
Safe in children ≥2 months
(FDA)
Approved
Not recommended
Topical 10% crotamiton
Safe in children
Not recommended
Not recommended
Oral ivermectin
Not approved in children
<15 kg or 5 years of age
Only recommended in France
Only recommended in France
FDA, Food and Drug Administration.
Scabies-related itching
- The itching associated with scabies can significantly affect quality of
life and may continue for some time even after all mites have been
eradicated. This necessitates proactive management from the onset.
- Moisturizers, oral antihistamines, and topical steroids can help alleviate
itching associated with scabies.
Mechanism of itching in scabies patients
The itching associated with scabies infection is thought to involve multiple
immunological mechanisms, including hypersensitivity reactions to the mites and
their secretions [18]. The innate immune
response, primarily driven by the complement system, plays a significant role,
with substantial involvement of mast cells. The T-cell-mediated response varies
between classic scabies and crusted scabies: a Th1 response is predominant in
classic scabies, while a Th2 response prevails in crusted scabies. Notably, in
crusted scabies, there is an observed infiltration of CD8+ T-cells within the
dermis and increased apoptosis of keratinocytes, which can exacerbate the
itching [19].
Additionally, the increased expression of Toll-like receptors-3, -4, and -7 in
peripheral nerves due to scabies mites, along with the activation of
protease-activated receptor-2 by proteases secreted by the mites, and certain
IgE-mediated allergic reactions are considered direct causes of scabies-related
itching. Immune responses involving macrophages, prostaglandins, and
leukotrienes also contribute to the itching. Furthermore, secondary bacterial
infections may exacerbate the itching through interleukin-31 expression and
Toll-like receptors activation [20].
Treatment of itching in scabies patients
Many scabies patients experience severe itching, which disrupts their sleep and
diminishes their quality of life, necessitating proactive itch relief treatment.
For patients with concurrent skin or systemic conditions that induce itching,
such as atopic dermatitis or chronic kidney disease, intensive treatment from
the start is advised. These conditions may foster an environment conducive to
mite survival due to compromised barriers or immune abnormalities, potentially
exacerbating the itching associated with scabies [21].
Standard approaches typically include moisturizers, topical corticosteroids, and
oral antihistamines as the first line of treatment. Moisturizers help restore
the skin barrier and prevent dryness, which aids in relieving itching [7,18,22]. Antihistamines are
commonly chosen for initial treatment, with first-generation antihistamines also
aiding in improving sleep for scabies patients [23]. Topical steroids can help manage inflammatory itching; however,
their use should be limited to areas of intense itch. Topical calcineurin
inhibitors, such as tacrolimus and pimecrolimus, are effective, particularly for
nodular scabies lesions [24]. While
systemic steroids are generally avoided due to potential side effects like
immunosuppression or increased blood glucose, short-term use may be considered
when severe itching persists after mite eradication [25]. Narrow-band UVB phototherapy is considered a safe
option, even for pregnant women and children [26].
In some cases, contact dermatitis may occur after applying topical scabicides.
Should this happen, treatment with oral antihistamines and topical steroid
ointments is recommended [18,27]. If traditional treatments do not
alleviate the itching associated with scabies, alternative therapies, including
protease-activated receptor-2 inhibitors, Th2 cytokine inhibitors, transient
receptor potential channel modulators, and gabapentin-class antidepressants,
might be considered [20]. While these
medications are not typically used in everyday practice, research has
demonstrated their efficacy in relieving itching.
Prevention and infection control
- Scabies patients require contact precautions or isolation until 24 hours
after the final application of treatment.
- Close contacts should receive a single preventive treatment, even if they
are asymptomatic, and should then be monitored for the development of
symptoms over a 6-week period.
- The patient's clothing, bedding, and linens must be laundered and
dried using heat. Additionally, medical equipment and items, as well as the
surrounding environment that the patient has touched, should be disinfected
with alcohol or other standard methods.
- When a case of scabies is identified, it is essential to isolate the
patient, manage contacts, and control the environment to prevent
transmission (Table 3).
Table 3.
Recommended measures for scabies prevention
Classic scabies
Crusted scabies
Isolation
- Maintain contact precautions for up to
24 hours after the last treatment or until the doctor determines
that the infectiousness has subsided.
- Isolate in single rooms or cohorts until
the doctor determines that the infectiousness has subsided.
Contact management
- Administer preventive
treatment once. - Medical staff, employees, caregivers, and
family members should wear disposable gloves and gowns and perform
hand washing before and after contacting the patient. -
Observe for symptoms for 6 weeks, considering the incubation
period.
Room management
- For rooms used by scabies
patients, clean daily using a dedicated vacuum cleaner or disposable
absorbent cloth during the isolation or treatment period. -
For rooms that have been vacated or after a patient has been
discharged, clean and disinfect using standard methods. -
Empty the vacuum cleaner bag daily, clean the dust collection tube,
and dispose of the absorbent cloth as infectious medical waste.
Item management
- Disinfect diagnostic
equipment such as dermoscopes, blood pressure cuffs, stethoscopes,
and wheelchairs using standard methods before they are used by
another patient. - Clean beds, sofas, etc. with a vacuum
cleaner. - Put items that cannot be laundered in a plastic
bag and store them for at least 7 days before reuse. -
Discard any remaining medication used by scabies patients.
Laundry management
- Machine wash in hot water at
50°C for 10–20 minutes and dry at a high
temperature. - Laundry handlers should wear disposable gloves
and gowns. - For items that cannot be laundered, store them
in a plastic bag for at least 7 days and dry them at 50°C or
higher. - Manage all laundry the patient uses for at least 3
days before treatment and change the patient’s clothing,
bedding, and towels daily.
Patient’s home management
- Clean the entire house with
a vacuum cleaner daily during the isolation or treatment
period. - Machine wash and dry contaminated clothing,
bedding, towels, etc. in hot water at 50°C for 10–20
minutes. - For items that cannot be laundered, store in a
plastic bag for at least 7 days and dry at 50°C or
higher.
Patient contact precautions and isolation
Effective management of scabies patients is essential to prevent transmission and
ensure optimal treatment outcomes. For classic scabies, it is important to
adhere to contact precautions throughout the treatment period. Patients should
avoid close contact with others until 24 hours after the final treatment
application or until a physician confirms that the risk of transmission has
decreased. At home, physical contact between the scabies patient and other
household members should be minimized, and sharing personal items should be
avoided. In healthcare settings, patients may be isolated in a single room or
placed in cohort isolation, depending on the resources available at the
institution. For crusted scabies, which is highly contagious, more stringent
precautions are necessary. Contact tracing and disinfection measures should be
expanded. Patients should remain in single-room or cohort isolation until a
physician confirms that the risk of transmission has decreased. Healthcare
providers, caregivers, and family members should continue to observe contact
precautions.
Contact management
Given the potential for asymptomatic latency lasting several weeks, it is
essential to manage contacts of scabies patients effectively. When a case occurs
within a family, all close contacts, including cohabitants and family members,
should undergo simultaneous treatment, regardless of whether they exhibit
symptoms [7,27,28]. Generally,
both children and adults can return to daycare, school, or work the day after
treatment. However, in some instances, their return may be postponed until the
completion of treatment is confirmed.
Close contacts should receive a single preventive treatment and be monitored for
symptoms over a 6-week period. For hospitalized scabies patients, healthcare
staff, caregivers, and family members must wear personal protective equipment,
including disposable gloves and gowns, during contact with the patient and
adhere to hand hygiene practices. Healthcare personnel who have been in contact
with scabies patients may return to work the day after receiving preventive
treatment. Any staff member who develops symptoms should immediately stop
working, undergo diagnostic testing, and receive treatment if diagnosed [21,23,27–32].
Environmental management
Scabies mites can survive off a human host for 48–72 hours, but they
generally cannot live longer than 3 days in the environment. They are killed by
exposure to temperatures above 50°C for 10 minutes. In households where a
scabies case has occurred, any clothing, bedding, or towels used by the patient
within the past three days should be machine-washed in hot water (above
50°C) for 10–20 minutes and dried on high heat. Items that cannot
be washed should be sealed in plastic bags for at least seven days, then
tumble-dried at high heat for 10–20 minutes at temperatures of
50°C or higher.
In healthcare facilities and nursing homes, patient rooms must be cleaned daily
during isolation periods. This cleaning should be performed using either a
dedicated vacuum cleaner or disposable absorbent cloths. The bags or containers
of the vacuum cleaner should be emptied and cleaned daily, with disposable bags
being replaced as needed. Additionally, the interior of the vacuum should be
sanitized. Absorbent cloths used in the cleaning process must be disposed of as
medical waste. Shared medical equipment, including dermoscopes, blood pressure
cuffs, stethoscopes, and wheelchairs, must be disinfected with either alcohol or
diluted bleach after each patient use.
Laundry from scabies patients requires careful handling on treatment days. It
should be sealed in a plastic bag and placed in a designated contaminated
laundry bin. Subsequently, it should be machine-washed at a temperature of
50°C or higher for 10–20 minutes and then heat-dried. Staff
responsible for handling this laundry must wear personal protective equipment,
which includes disposable gloves and gowns, and ensure that the patient's
laundry is kept separate from other items. Additionally, medical waste from
scabies patients should be disposed of in dedicated containers.
Conclusion
The Scabies Eradication Public Health Project Committee of the Korean Dermatological
Association has developed clinical practice guidelines specifically designed for
Korean patients. These guidelines are based on medical evidence, consensus among
domestic scabies specialists, and external validation. They provide a comprehensive
overview of the epidemiology, clinical symptoms, diagnosis, treatment, follow-up,
prevention, and management of scabies in Korea. Additionally, a clear and concise
diagnostic and treatment algorithm is included to aid healthcare professionals in
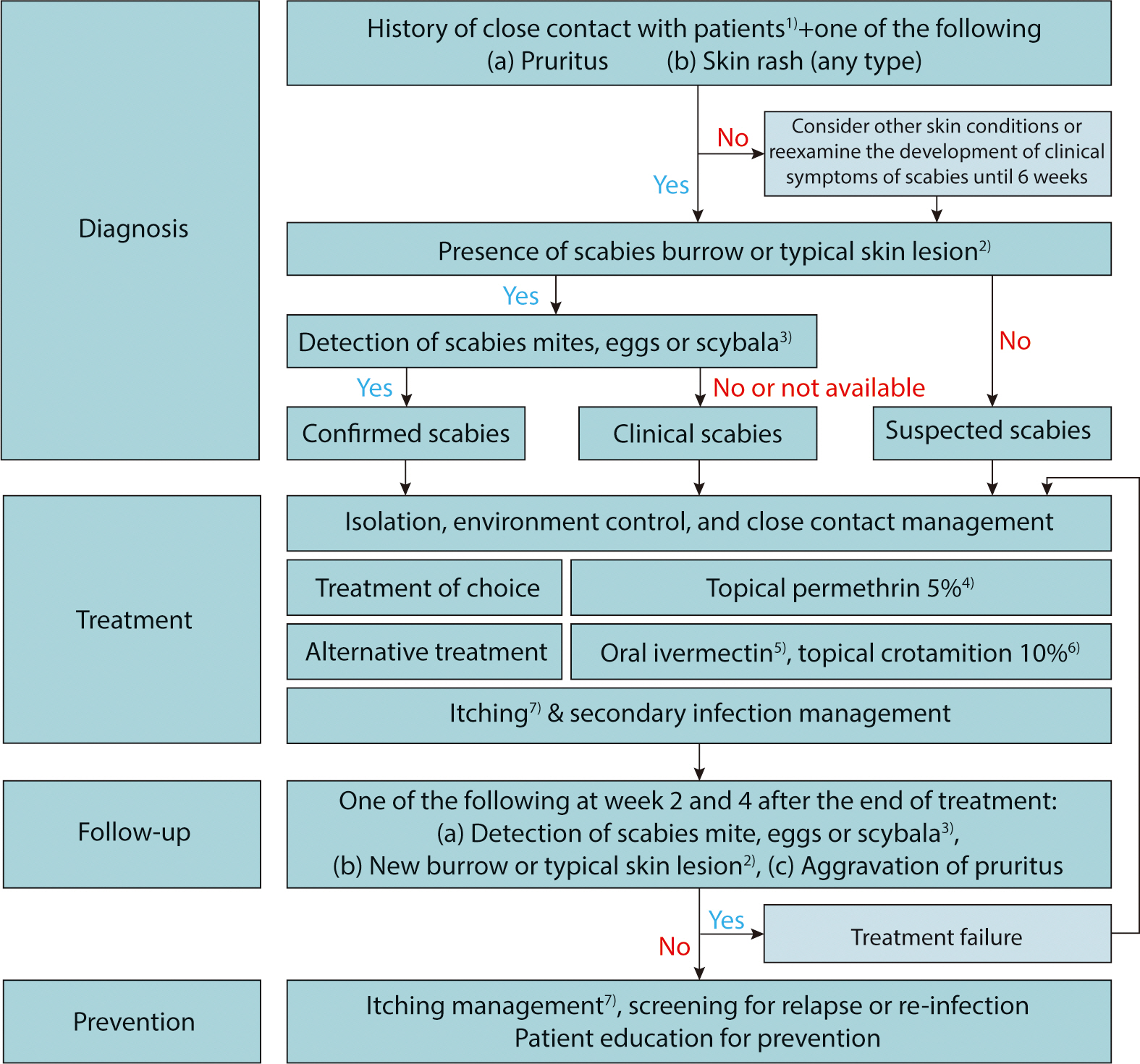
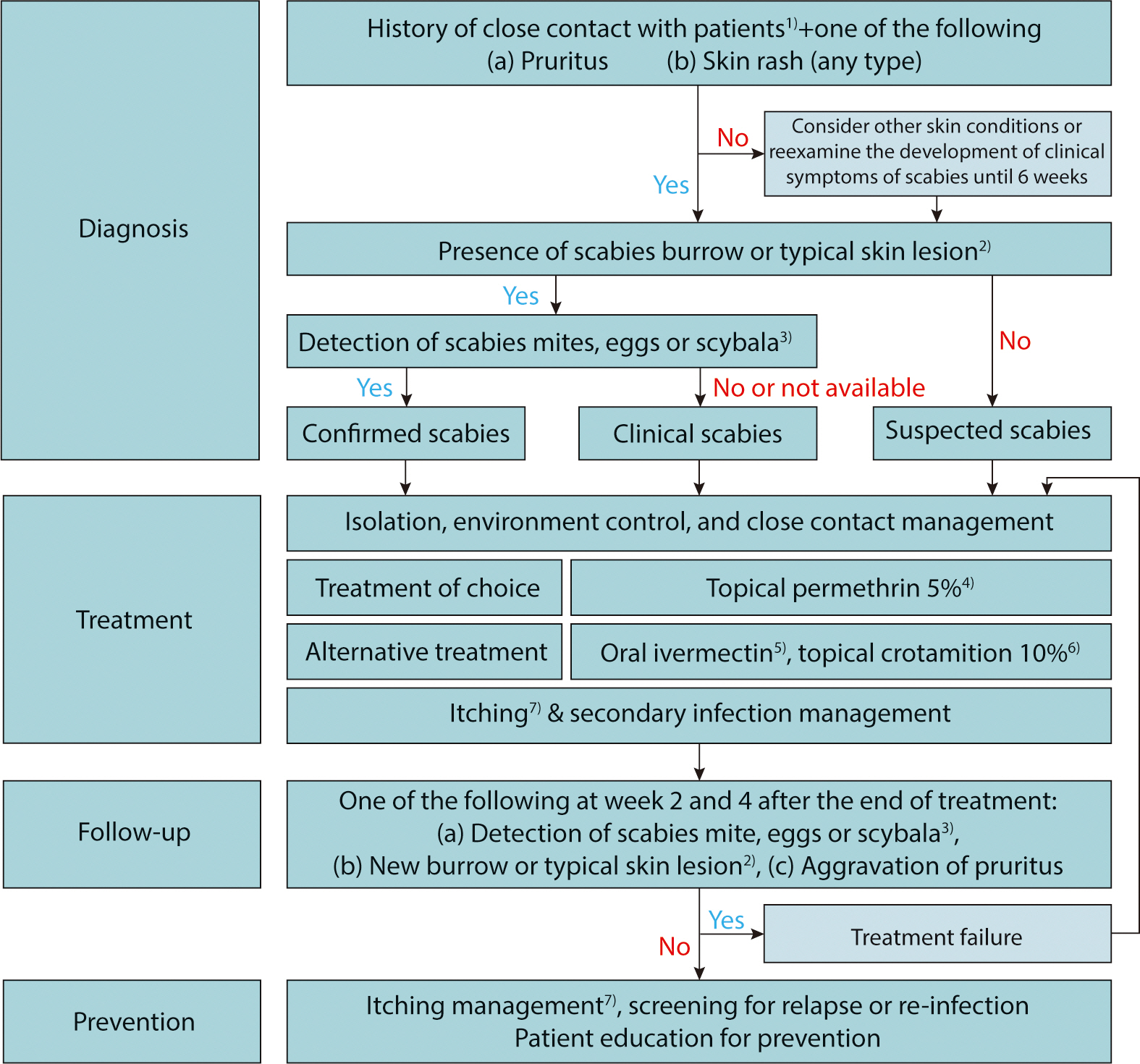
making quick decisions during scabies consultations (Fig. 1). We hope these guidelines will serve as a reliable and practical
resource for the treatment and prevention of scabies, ultimately contributing to
improved public health.
Fig. 1.
Proposed algorithm for the diagnosis and treatment of scabies in Korea.
1) One of the following: (a) Skin contact with an individual
diagnosed with scabies, (b) sexual contact with an individual diagnosed with
scabies (especially nodular scabies), (c) brief direct contact with linens
(such as towels, clothing, and bedding) used by an individual diagnosed with
scabies (especially crusted scabies); 2) One of the following:
(a) Typical erythematous papules or vesicles in a typical distribution
including the periumbilical area, inner thigh, buttock, axilla, inner
forearm, (b) multiple nodules in genital area or axilla, (c) multiple
papules, vesicles, or pustules in the palmoplantar distribution of an
infant; 3) Light microscopy, dermoscopy, or other high-resolution
imaging techniques including could be used; 4) In general, apply
on the whole body, except the face and scalp, at least 30 minutes after
taking a shower. For treatment of infants and older adults, it should be
applied to the lesion on the scalp and face; the recommended doses are as
follows: 25–30 g (1 tube) for adults, 15 g (1/2 tube) for ages
6–12 years, and up to 7.5 g (1/4 tube) for ages 2–5 years;
cleansed out after at least 8–12 hours of application. Application is
repeated after 7–10 days. For crusted scabies, 5% permethrin cream
should be applied daily for a week, then twice weekly until any mite or egg
is not identified. However, 5% permethrin cream is not permitted for use in
patients aged <2 years and pregnant or lactating women in Korea;
therefore, Centers for Disease Control and Prevention guidelines recommend
using 5% permethrin cream in patients older than 2 months and pregnant or
lactating women; 5) For classic scabies, the recommended dose is
200 μg/kg twice weekly; For crusted scabies, ivermectin is
administered on days 0, 1, 7, 8, 14, 21, and 28. Safety in patients who are
pregnant or weigh <15 kg is not established; 6) Apply
repeatedly for 3–5 days (i.e., days 1, 2, 3, and 8), and leave on for
at least 8 hours; it can be used for children and pregnant or lactating
women cautiously; 7) Emollients, H1 antihistamines, topical or
systemic steroids (in selected cases), topical calcineurin inhibitors, and
narrow-band ultraviolet B could be used.
These guidelines should be applied based on the healthcare provider's
knowledge and clinical experience, taking into account each patient's
specific circumstances, clinical subtypes, and the available healthcare environment.
Additionally, we anticipate further research on scabies involving Korean patients,
which will facilitate the development of systematic clinical guidelines supported by
new clinical evidence.
Authors' contributions
Project administration: Park J, Kwon SH, Lee YB, Kim HS, Jeon JH, Choi GS
Conceptualization: Park J, Kwon SH, Lee YB, Kim HS, Jeon JH, Choi GS
Methodology & data curation: Park J, Kwon SH, Lee YB, Kim HS, Jeon JH,
Choi GS
Funding acquisition: not applicable
Writing – original draft: Park J, Kwon SH, Lee YB, Kim HS, Jeon JH, Choi
GS
Writing – review & editing: Park J, Kwon SH, Lee YB, Kim HS, Jeon
JH, Choi GS
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was supported by the Korean Dermatological Association.
Data availability
Not applicable.
Acknowledgments
We thank the members of the Korean Society for Cutaneous Mycology and Infection for
their valuable guidance.
1. Rosumeck S, Nast A, Dressler C. Evaluation of ivermectin vs permethrin for treating scabies:
summary of a Cochrane review. JAMA Dermatol 2019;155(6):730-732.
3. Hackenberg B, Horváth ON, Petachti M, Schult R, Yenigün N, Bannenberg P. Skabiestherapie in Deutschland: ergebnisse einer bundesweiten
umfrage mit besonderem fokus auf die wirksamkeit der erstlinientherapie mit
permethrin. Hautarzt 2020;71(5):374-379.
4. Mazzatenta C, Piccolo V, Argenziano G, Bassi A. Is scabies becoming less sensitive to permethrin
therapy? J Eur Acad Dermatol Venereol 2021;35(9):e607-e609.
5. Meyersburg D, Kaiser A, Bauer JW. ‘Loss of efficacy of topical 5% permethrin for treating
scabies: an Austrian single-center study’. J Dermatolog Treat 2022;33(2):774-777.
6. Centers for Disease Control and Prevention (CDC)’s Division
of Parasitic Diseases and Malaria. Resources of health professionals - medication, in: parasites –
scabies [Internet]. Atlanta (GA): CDC; c2023 [cited 2023 Jun 12]. Available from https://www.cdc.gov/parasites/scabies/health_professionals/meds.html
7. Salavastru CM, Chosidow O, Boffa MJ, Janier M, Tiplica GS. European guideline for the management of scabies. J Eur Acad Dermatol Venereol 2017;31(8):1248-1253.
8. Executive Committee of Guideline for the Diagnosis and Treatment of
Scabies. Guideline for the diagnosis and treatment of scabies in
Japan. J Dermatol 2017;44(9):991-1014.
12. Sunderkötter C, Feldmeier H, Fölster-Holst R, Geisel B, Klinke-Rehbein S, Nast A, et al. S1 guidelines on the diagnosis and treatment of scabies –
short version. J Dtsch Dermatol Ges 2016;14(11):1155-1167.
14. van der Rhee HJ, Farquhar JA, Vermeulen NP. Efficacy and transdermal absorption of permethrin in scabies
patients. Acta Derm Venereol 1989;69(2):170-173.
15. Fölster-Holst R, Rufli T, Christophers E. Die skabiestherapie unter besonderer berücksichtigung des
frühen kindesalters, der schwangerschaft und
stillzeit. Hautarzt 2000;51(1):7-13.
16. Romani L, Whitfeld MJ, Koroivueta J, Kama M, Wand H, Tikoduadua L, et al. Mass drug administration for scabies control in a population with
endemic disease. N Engl J Med 2015;373(24):2305-2313.
20. Kim HS, Hashimoto T, Fischer K, Bernigaud C, Chosidow O, Yosipovitch G. Scabies itch: an update on neuroimmune interactions and novel
targets. J Eur Acad Dermatol Venereol 2021;35(9):1765-1776.
23. Bernigaud C, Fischer K, Chosidow O. The management of scabies in the 21st century: past, advances and
potentials. Acta Derm Venereol 2020;100(9):adv00112
27. Widaty S, Miranda E, Cornain EF, Rizky LA. Scabies: update on treatment and efforts for prevention and
control in highly endemic settings. J Infect Dev Ctries 2022;16(02):244-251.
28. May PJ, Tong SYC, Steer AC, Currie BJ, Andrews RM, Carapetis JR, et al. Treatment, prevention and public health management of impetigo,
scabies, crusted scabies and fungal skin infections in endemic populations:
a systematic review. Trop Med Int Health 2019;24(3):280-293.
30. McCarthy-Khan P. Infection prevention and control–standard operating procedure for
scabies in a healthcare setting. Geneva: Infection Prevention and Control Policy Review
Group; 2021.
31. Korea Disease Control and Prevention Agency. Guide for prevention and management of scabies and head lice. Cheongju: Korea Disease Control and Prevention Agency; 2018.
32. Korea Disease Control and Prevention Agency. Guide for prevention and management of scabies in convalescent
hospital. Cheongju: Korea Disease Control and Prevention Agency; 2019.
Figure & Data
References
Citations
Citations to this article as recorded by
Comparative effectiveness of permethrin and ivermectin on pruritus and psychological outcomes in scabies: a prospective cohort of 600 adults Mustafa Esen, Abdullah Demirbas, Esin Diremsizoglu, Gozde Ulutas Demirbas Postgraduate Medicine.2026; 138(2): 224. CrossRef
Microscopic clearance with ivermectin–permethrin combination vs. permethrin alone in noncrusted scabies: a retrospective cohort study Ye Ji Kim, Su Min Kim, Hyun Chul Jung, Sang Seok Kim, Chul Woo Kim Clinical and Experimental Dermatology.2026; 51(8): 1442. CrossRef
Clinical practice guidelines for the diagnosis and treatment of
scabies in Korea: Part 2. Treatment and prevention — a secondary
publication
Fig. 1.
Proposed algorithm for the diagnosis and treatment of scabies in Korea.
1) One of the following: (a) Skin contact with an individual
diagnosed with scabies, (b) sexual contact with an individual diagnosed with
scabies (especially nodular scabies), (c) brief direct contact with linens
(such as towels, clothing, and bedding) used by an individual diagnosed with
scabies (especially crusted scabies); 2) One of the following:
(a) Typical erythematous papules or vesicles in a typical distribution
including the periumbilical area, inner thigh, buttock, axilla, inner
forearm, (b) multiple nodules in genital area or axilla, (c) multiple
papules, vesicles, or pustules in the palmoplantar distribution of an
infant; 3) Light microscopy, dermoscopy, or other high-resolution
imaging techniques including could be used; 4) In general, apply
on the whole body, except the face and scalp, at least 30 minutes after
taking a shower. For treatment of infants and older adults, it should be
applied to the lesion on the scalp and face; the recommended doses are as
follows: 25–30 g (1 tube) for adults, 15 g (1/2 tube) for ages
6–12 years, and up to 7.5 g (1/4 tube) for ages 2–5 years;
cleansed out after at least 8–12 hours of application. Application is
repeated after 7–10 days. For crusted scabies, 5% permethrin cream
should be applied daily for a week, then twice weekly until any mite or egg
is not identified. However, 5% permethrin cream is not permitted for use in
patients aged <2 years and pregnant or lactating women in Korea;
therefore, Centers for Disease Control and Prevention guidelines recommend
using 5% permethrin cream in patients older than 2 months and pregnant or
lactating women; 5) For classic scabies, the recommended dose is
200 μg/kg twice weekly; For crusted scabies, ivermectin is
administered on days 0, 1, 7, 8, 14, 21, and 28. Safety in patients who are
pregnant or weigh <15 kg is not established; 6) Apply
repeatedly for 3–5 days (i.e., days 1, 2, 3, and 8), and leave on for
at least 8 hours; it can be used for children and pregnant or lactating
women cautiously; 7) Emollients, H1 antihistamines, topical or
systemic steroids (in selected cases), topical calcineurin inhibitors, and
narrow-band ultraviolet B could be used.
Fig. 1.
Clinical practice guidelines for the diagnosis and treatment of
scabies in Korea: Part 2. Treatment and prevention — a secondary
publication
Drugs available in Korea for the treatment of scabies
Drug (product)
FDA approval for scabies treatment
Domestic approval (class)
Usage (dosing)
Topical 5% permethrin (Omeclean, 30 g
cream/tube)
Yes
Yes (prescription drug)
- Adult: 25–30 g (1 tube) -
6–12 years: 15 g (1/2 tube) - 2 months–5 years:
up to 7.5 g (1/4 tube)
Topical 10% crotamiton (Uracin, 50 g
ointment/tube)
Yes (only for adults)
Yes (over-the counter drug)
Adult: 25–30 g (1/2 tube)
Oral ivermectin (Stromectol, 3
mg/tablet)
No
No (orphan drug) Indication in
KOEDC - Failure or nonadherent to topical
treatment - Widespread institutional outbreaks
FDA, Food and Drug Administration; KOEDC, Korea Orphan & Essential
Drug Center.
Summary of drugs for scabies treatment in children, pregnant and
breastfeeding women
Drugs
Use in children
Use in pregnancy
Use in breastfeeding
Topical 5% permethrin
Safe in children ≥2 months
(FDA)
Approved
Not recommended
Topical 10% crotamiton
Safe in children
Not recommended
Not recommended
Oral ivermectin
Not approved in children
<15 kg or 5 years of age
Only recommended in France
Only recommended in France
FDA, Food and Drug Administration.
Recommended measures for scabies prevention
Classic scabies
Crusted scabies
Isolation
- Maintain contact precautions for up to
24 hours after the last treatment or until the doctor determines
that the infectiousness has subsided.
- Isolate in single rooms or cohorts until
the doctor determines that the infectiousness has subsided.
Contact management
- Administer preventive
treatment once. - Medical staff, employees, caregivers, and
family members should wear disposable gloves and gowns and perform
hand washing before and after contacting the patient. -
Observe for symptoms for 6 weeks, considering the incubation
period.
Room management
- For rooms used by scabies
patients, clean daily using a dedicated vacuum cleaner or disposable
absorbent cloth during the isolation or treatment period. -
For rooms that have been vacated or after a patient has been
discharged, clean and disinfect using standard methods. -
Empty the vacuum cleaner bag daily, clean the dust collection tube,
and dispose of the absorbent cloth as infectious medical waste.
Item management
- Disinfect diagnostic
equipment such as dermoscopes, blood pressure cuffs, stethoscopes,
and wheelchairs using standard methods before they are used by
another patient. - Clean beds, sofas, etc. with a vacuum
cleaner. - Put items that cannot be laundered in a plastic
bag and store them for at least 7 days before reuse. -
Discard any remaining medication used by scabies patients.
Laundry management
- Machine wash in hot water at
50°C for 10–20 minutes and dry at a high
temperature. - Laundry handlers should wear disposable gloves
and gowns. - For items that cannot be laundered, store them
in a plastic bag for at least 7 days and dry them at 50°C or
higher. - Manage all laundry the patient uses for at least 3
days before treatment and change the patient’s clothing,
bedding, and towels daily.
Patient’s home management
- Clean the entire house with
a vacuum cleaner daily during the isolation or treatment
period. - Machine wash and dry contaminated clothing,
bedding, towels, etc. in hot water at 50°C for 10–20
minutes. - For items that cannot be laundered, store in a
plastic bag for at least 7 days and dry at 50°C or
higher.
Table 1.
Drugs available in Korea for the treatment of scabies
FDA, Food and Drug Administration; KOEDC, Korea Orphan & Essential
Drug Center.
Table 2.
Summary of drugs for scabies treatment in children, pregnant and
breastfeeding women
FDA, Food and Drug Administration.
Table 3.
Recommended measures for scabies prevention