1Department of Radiology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
2Research Institute of Radiological Sciences, Center for Clinical Imaging Data Science, and Institute for Innovation in Digital Healthcare, Yonsei University College of Medicine, Seoul, Korea
3Department of Pathology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
*Corresponding author: Hyungjin Rhee,
Department of Radiology, Severance Hospital, Yonsei University College of
Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea, E-mail:
hjinrhee@yuhs.ac
• Received: August 30, 2024 • Accepted: October 2, 2024
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Intrahepatic cholangiocarcinoma (iCCA) is a heterogeneous bile duct
adenocarcinoma with a rising global incidence and a poor prognosis. This review
aims to present a comprehensive overview of the most recent radiological
research on iCCA, focusing on its histopathologic subclassification and the use
of imaging findings to predict prognosis and inform treatment decisions.
Histologically, iCCA is subclassified into small duct (SD-iCCA) and large duct
(LD-iCCA) types. SD-iCCA typically arises in the peripheral small bile ducts and
is often associated with chronic hepatitis or cirrhosis. It presents as a
mass-forming lesion with a relatively favorable prognosis. LD-iCCA originates
near the hepatic hilum, is linked to chronic bile duct diseases, and exhibits
more aggressive behavior and poorer outcomes. Imaging is essential for
differentiating these subtypes and assessing prognostic factors like tumor size,
multiplicity, vascular invasion, lymph node metastasis, enhancement patterns,
and intratumoral fibrosis. Imaging-based prognostic models have demonstrated
predictive accuracy comparable to traditional pathological staging systems.
Furthermore, imaging findings are instrumental in guiding treatment decisions,
including those regarding surgical planning, lymphadenectomy, neoadjuvant
therapy, and the selection of targeted therapies based on molecular profiling.
Advancements in radiological research have improved our understanding of iCCA
heterogeneity, facilitating prognosis prediction and treatment personalization.
Imaging findings assist in subclassifying iCCA, predicting outcomes, and
informing treatment decisions, thus optimizing patient management. Incorporating
imaging-based approaches into clinical practice is crucial for advancing
personalized medicine in the treatment of iCCA. However, further high-level
evidence from international multicenter prospective studies is required to
validate these findings and increase their clinical applicability.
Cholangiocarcinoma (CCA) is an adenocarcinoma characterized by differentiation of
the bile duct epithelium. Based on its anatomical location, CCA is classified
into intrahepatic CCA (iCCA), perihilar CCA (pCCA), and distal CCA (dCCA) [1,2].
CCAs located more peripherally than the second confluence of the bile ducts are
classified as iCCA, those situated between the second confluence and the cystic
duct insertion site on the common bile duct are categorized as pCCA, and those
found distal to the cystic duct insertion are classified as dCCA [3]. iCCAs account for 10% to 20% of all
CCAs, while pCCAs (50% to 60%) and dCCAs (20% to 30%) are more common [3]. However, while the rates of pCCA and
dCCA are decreasing, the age-standardized incidence of iCCA has been rising
globally over the past few decades, necessitating closer attention [3]. iCCA is the second most common primary
liver cancer after hepatocellular carcinoma (HCC) and has a worse prognosis than
HCC [4]. Recently, our understanding of
iCCA has improved, and it is now recognized as a heterogeneous tumor with
diverse etiology, clinical presentation, pathology, and genetic characteristics.
The clinical significance of this heterogeneity is being increasingly
recognized.
iCCA often presents as a mass with variable shapes, including lobulated or
irregular contours, and may be associated with bile duct dilatation, vascular
encasement, and regional lymph node metastasis [5]. The enhancement patterns observed on dynamic CT or MRI are
diverse; typically, peripheral enhancement is evident in the arterial phase,
followed by centripetal enhancement in later phases [6,7]. On MRI, most
iCCAs exhibit high signal intensity on T2-weighted images relative to the
surrounding liver parenchyma, display diffusion restriction on
diffusion-weighted images, and appear hypointense in the hepatobiliary phase
when gadoxetic acid is used as a contrast medium [6–8]. The imaging
characteristics of iCCA are heterogeneous, reflecting the recently recognized
diversity of the disease. Accumulating evidence suggests that these imaging
features can be clinically applied to predict prognosis and guide treatment
decisions [9,10].
Objectives
This review provides a comprehensive overview of recent radiological research on
iCCA, emphasizing its histopathological subclassification as well as imaging
findings that aid in predicting the prognosis of iCCA and in making treatment
decisions.
Ethics statement
As this study is based on a review of the literature, neither institutional review
board approval nor informed consent was required.
Histopathologic subclassification of intrahepatic cholangiocarcinoma
In the fifth edition of the World Health Organization classification, updated in
2019, a new histological subclassification of iCCA was introduced, delineating small
duct (SD-iCCA) and large duct (LD-iCCA) types [11,12]. SD-iCCA and LD-iCCA are
distinct not only in their histopathological morphology but also in their etiology,
tumor location, gross morphology, histopathological characteristics such as
invasiveness and vascularity, molecular features, and prognosis (Table 1).
Table 1.
Comparison of characteristics between small duct and large duct
iCCA
SD-iCCA typically arises in the small bile ducts within the peripheral liver, often
in the context of chronic hepatitis and cirrhosis. It is characterized by an
exclusively mass-forming (MF) gross morphology [13]. Histologically, SD-iCCA consists of cuboidal or low columnar cells
arranged in a tubular or cord-like glandular pattern. Compared to LD-iCCA, SD-iCCA
is less frequently associated with aggressive pathological features, such as
perineural invasion, vascular invasion, and lymph node metastasis [14]. It also tends to have a higher
microvascular density (MVD) and exhibits necrosis less frequently. Overall, SD-iCCA
has a more favorable prognosis than LD-iCCA [15,16].
LD-iCCA typically originates in the large bile ducts near the hilum and is often
associated with underlying chronic bile duct diseases such as hepatolithiasis, liver
fluke infestation, or primary sclerosing cholangitis [13]. LD-iCCA frequently arises from a multistep carcinogenesis
process, with well-known precursor lesions including biliary intraepithelial
neoplasia and intraductal papillary neoplasm of the bile duct [17]. It usually develops from either periductal-infiltrating or
intraductal-growing tumors of the large bile duct [14]. These tumors can further evolve into the MF type or present as a
hybrid of the MF and either the periductal-infiltrating or the intraductal-growing
type [18]. Compared to the SD-iCCA, LD-iCCA
more frequently exhibits perineural invasion, vascular invasion, and lymph node
metastasis; it also displays lower MVD and more frequent necrosis [14,19].
LD-iCCA has a poorer prognosis than SD-iCCA due to its high invasiveness, which
leads to frequent recurrence after curative surgical resection and resistance to
chemotherapy [20,21].
Utilizing imaging findings to predict prognosis in intrahepatic
cholangiocarcinoma
Imaging assessment of the American Joint Committee on Cancer, Eighth Edition,
tumor-node-metastasis staging system
The prognosis of iCCA in clinical settings is generally stratified using the
eighth edition of the American Joint Committee on Cancer (AJCC) staging system.
This system incorporates the tumor, node, metastasis (TNM) classification [22] and was developed and validated through
pathological assessment of tumor involvement [22–25]. In iCCA
staging, the T category is defined by several factors, including the size of the
tumor (with a threshold of 5 cm), the number of tumors present, vascular
invasion, visceral peritoneal perforation, and invasion of extrahepatic organs.
The N category signifies the presence of regional lymph node metastasis, while
the M category indicates distant metastasis. Although TNM staging should be
definitively determined through pathological examination of resectable tumors,
imaging-based staging is commonly employed to predict prognosis and guide
treatment decisions for tumors prior to surgical resection or those deemed
unresectable.
The eighth edition of the AJCC provides brief guidance on the clinical TNM
classification for iCCA, noting that both contrast-enhanced CT and MRI are
valuable for detecting tumors larger than 2 cm and assessing vascular
involvement. Additionally, it indicates that magnetic resonance
cholangiopancreatography can offer additional insights into the extent of
disease. However, recent clinical practice guidelines from the European
Association for the Study of the Liver and the International Liver Cancer
Association (EASL-ILCA) recommend MRI over CT for the staging of iCCA [2]. This guidance is supported by a
multicenter retrospective study that directly compared these modalities and
revealed the superiority of MRI in staging MF-iCCAs, especially for tumors
classified as T1b, T2, and T3/T4. Specifically, MRI displayed better performance
in predicting T category components, such as tumor multiplicity, vascular
invasion, and visceral peritoneal invasion [26].
Tumor size and multiplicity
The eighth edition AJCC staging system for iCCA categorizes solitary tumors
as T1a or T1b, depending on whether the tumor is larger or smaller than 5
cm. This classification is underpinned by multiple studies demonstrating
that tumors exceeding 5 cm are linked to comparatively poor survival
outcomes and a high likelihood of recurrence [27–29].
Recent research has confirmed the reliability of preoperative imaging for
accurately estimating iCCA tumor size, revealing a median difference of less
than 0.5 cm between pathological and radiological measurements [30]. Furthermore, a study comparing the
effectiveness of CT and MRI for determining iCCA tumor size reported no
significant difference between these modalities [26].
Tumor multiplicity is another key determinant for the T category in the AJCC
staging system, with its presence categorizing a tumor as T2. Multiplicity
is defined as the presence of satellitosis, multifocal tumors, or
intrahepatic metastasis [22]. Studies
have demonstrated that tumor multiplicity is linked to poorer overall
survival and a higher risk of tumor recurrence after resection [31,32]. As previously noted, a recent study showed MRI to be
superior to CT in the imaging assessment of tumor multiplicity [26].
In both CT and MRI dynamic imaging studies, the assessment of tumor size and
the detection of satellite nodules in iCCA typically involve the use of the
portal venous phase [26,33]. Regarding MRI, hepatobiliary phase
and diffusion-weighted imaging are also useful, particularly for detecting
small lesions [34,35].
Vascular invasion
Vascular invasion, which includes both macrovascular invasion and
microvascular invasion (MiVI) observed on histopathologic examination, is a
major prognostic factor for iCCA. Specifically, it assigns a stage of T2 in
the eighth edition AJCC system [22].
Research indicates that MiVI in iCCA is significantly linked to poor overall
survival. Additionally, macrovascular invasion has been associated with
comparatively low overall and disease-free survival [36,37].
The challenge of clinical staging arises from the inability to directly
observe MiVI using CT or MRI. To address this issue, recent research has
focused on identifying imaging characteristics that can predict the presence
of MiVI in iCCA. Studies have found that MiVI is more commonly associated
with larger tumors, lobulated or irregular tumor morphology, thin-rim
enhancement during the arterial phase, penetration of the hepatic artery
within the tumor, bile duct dilation, and a high apparent diffusion
coefficient (ADC) [38–40].
Lymph node metastasis
Lymph node metastasis is widely recognized as a strong prognostic factor for
iCCA [31,41]. The conventional criteria for detecting lymph node
metastasis on CT and MRI generally involve a lymph node size threshold of 1
cm in short-axis diameter, along with imaging characteristics such as round
shape, irregular margins, and internal necrosis [42]. Recent studies have demonstrated that the
inclusion of tumor imaging factors—such as arterial phase
hypoenhancement, tumor multiplicity, bile duct involvement, periductal
infiltrating growth pattern, and a primary tumor located in the left
lobe—combined with serum tumor markers like elevated carcinoembryonic
antigen and carbohydrate antigen 19-9 (CA19-9) levels, can improve the
accuracy of lymph node metastasis detection in iCCA [43–46].
However, the diagnostic accuracy of CT and MRI for detecting lymph node
metastases is generally considered to be inadequate. The most recent
EASL-ILCA guidelines advise the routine use of 18-fludeoxyglucose positron
emission tomography-CT (18F-FDG PET-CT) for patients with
apparently resectable iCCA to achieve precise clinical nodal staging [2]. This recommendation stems from a
recent meta-analysis, which revealed that MRI has a sensitivity of 64% and a
specificity of 69% for identifying lymph node metastases. In contrast,
18F-FDG PET-CT demonstrated a sensitivity of 52% but a
notably higher specificity of 92% [47].
Radiological prognosis prediction
Subclassification of intrahepatic cholangiocarcinoma
Subclassifying iCCA based on radiological findings can be useful for
predicting prognosis, as LD-iCCA is associated with a poorer prognosis than
SD-iCCA. Imaging can be employed to assess the differences in gross
morphology between these types of iCCA. SD-iCCA typically exhibits a MF
appearance with a round or lobulated shape (Figs. 1, 2) [48]. In contrast, LD-iCCA often
displays irregular contours alongside a round or lobulated shape, frequent
bile duct involvement that is readily apparent on T2-weighted MRI, and
vascular encasement (Fig. 3) [9,10,48]. Recent studies
indicate that features such as infiltrative contours, adjacent bile duct
dilatation, the absence of arterial phase hyperenhancement, and vascular
invasion are associated with LD-iCCA and are correlated with poorer
disease-free and overall survival [48,49].
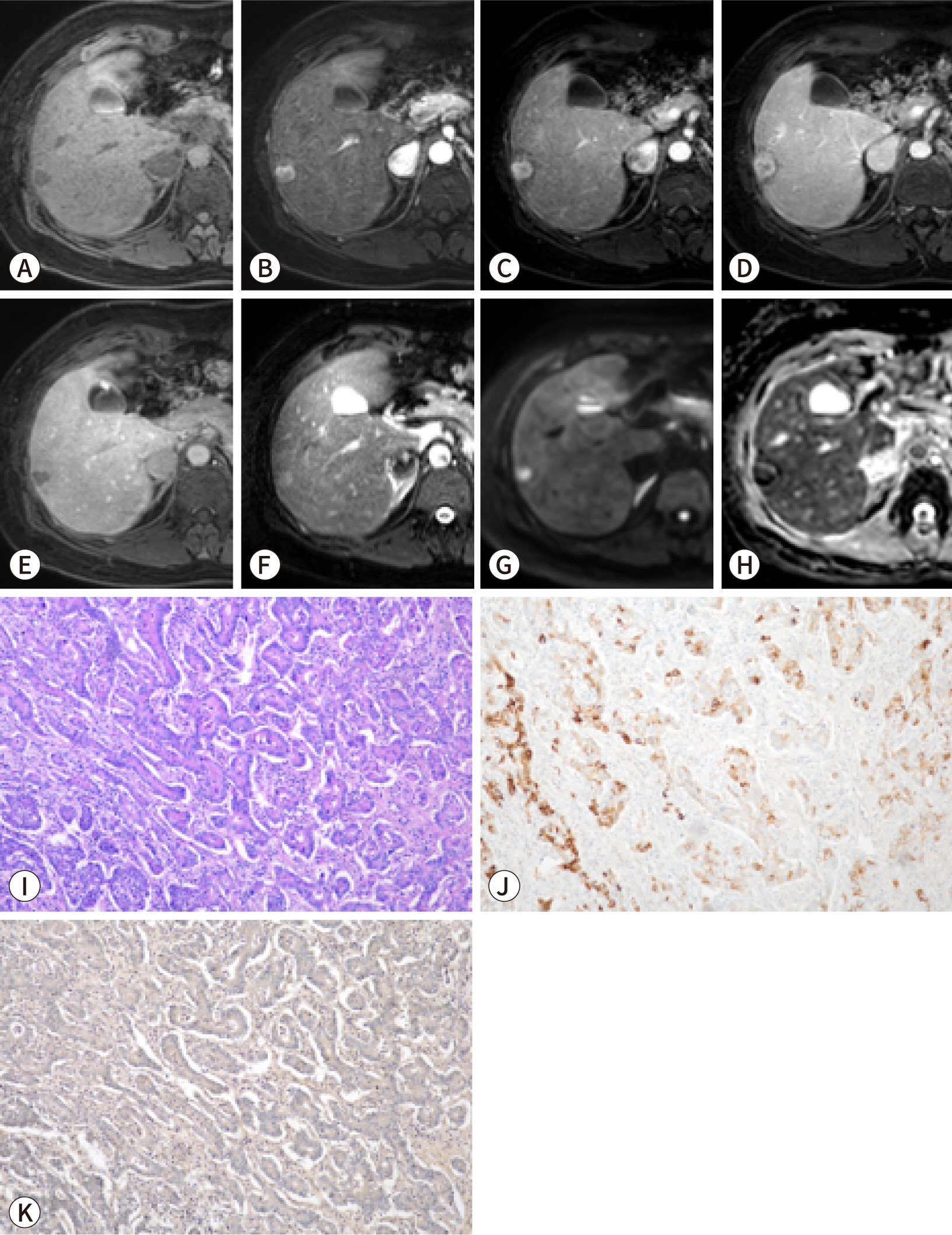
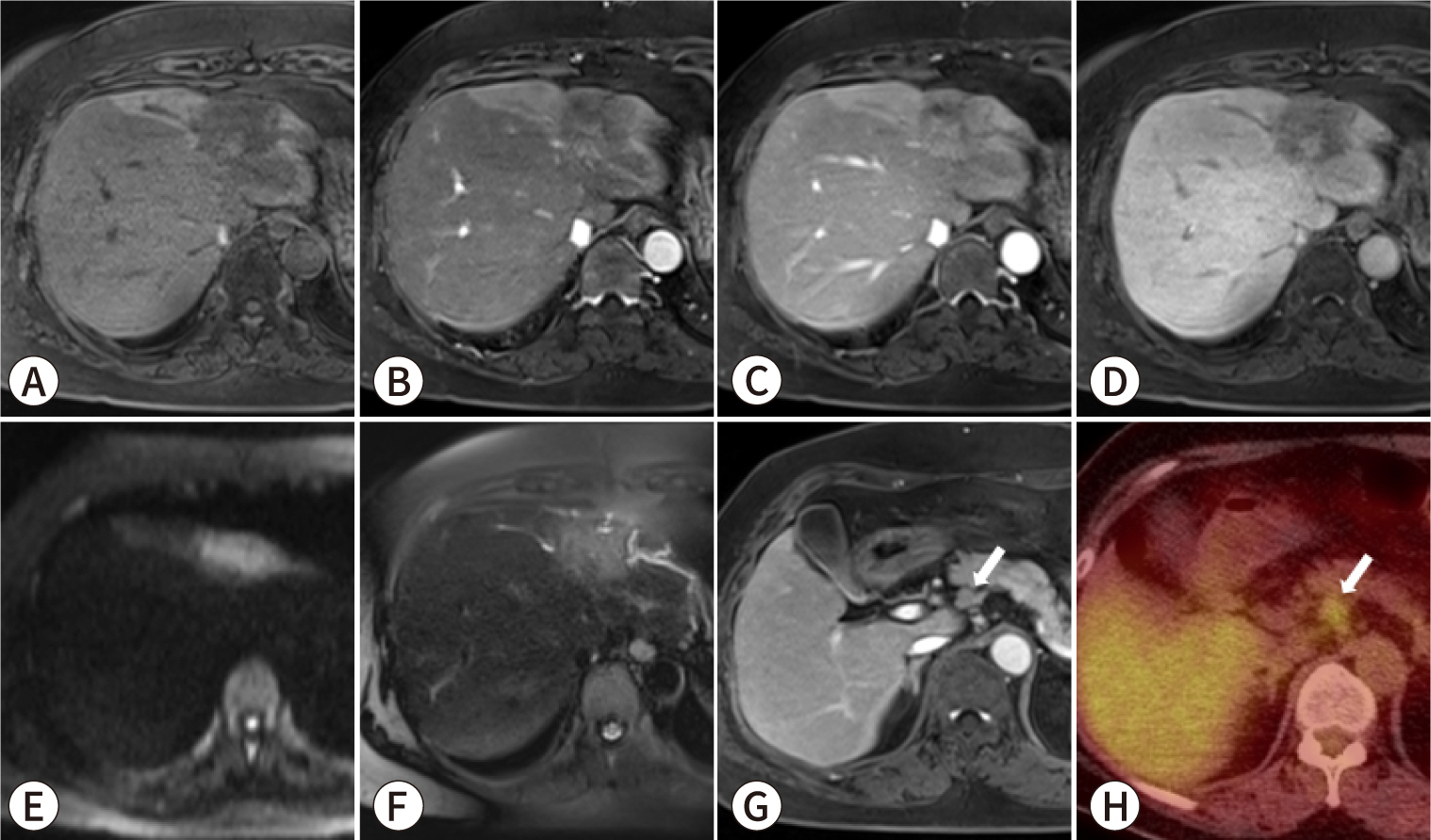
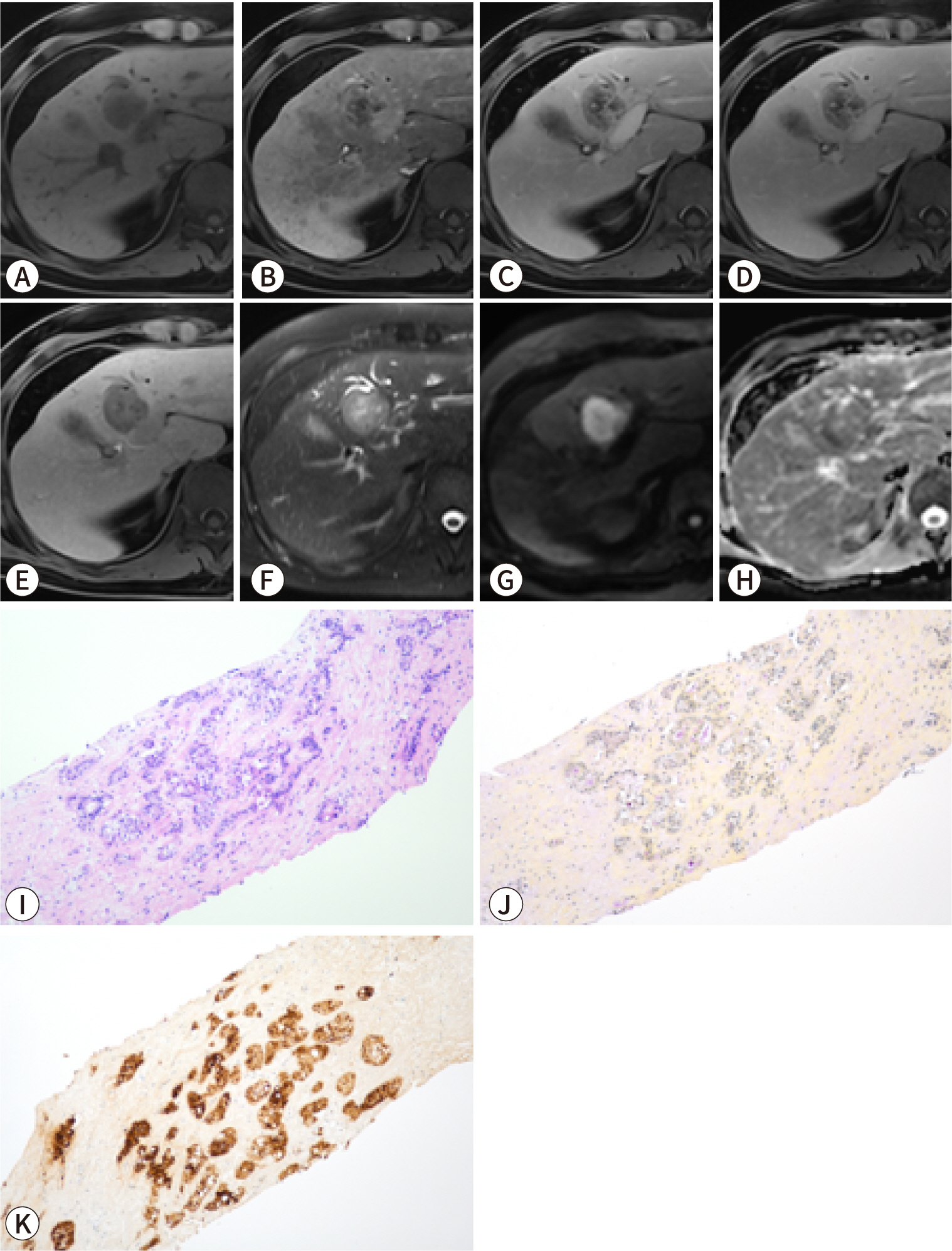
Fig. 1.
A 34-year-old female patient with liver cirrhosis and small
duct-type intrahepatic cholangiocarcinoma (iCCA). Gadoxetic
acid-enhanced MRI: (A) pre-contrast T1-weighted, (B) arterial phase,
(C) portal phase, (D) transitional phase, (E) hepatobiliary phase,
(F) T2-weighted, and (G) diffusion-weighted (b=800 s/mm2)
images and (H) apparent diffusion coefficient map. Staining: (I)
hematoxylin-eosin, (J) C-reactive protein (CRP) immunohistochemical,
and (K) mucicarmine staining (I–K, original magnification
×200). The gadoxetic acid-enhanced MRI reveals a 1.5-cm round
mass in the subcapsular area of the right liver. The mass exhibits
hyperenhancement in the arterial phase (B), does not show washout in
the portal phase (C), and appears hypointense in the hepatobiliary
phase (E). Pathological examination confirmed the lesion as a small
duct iCCA with positive CRP expression (J) and the absence of mucin
under mucicarmine staining (K).
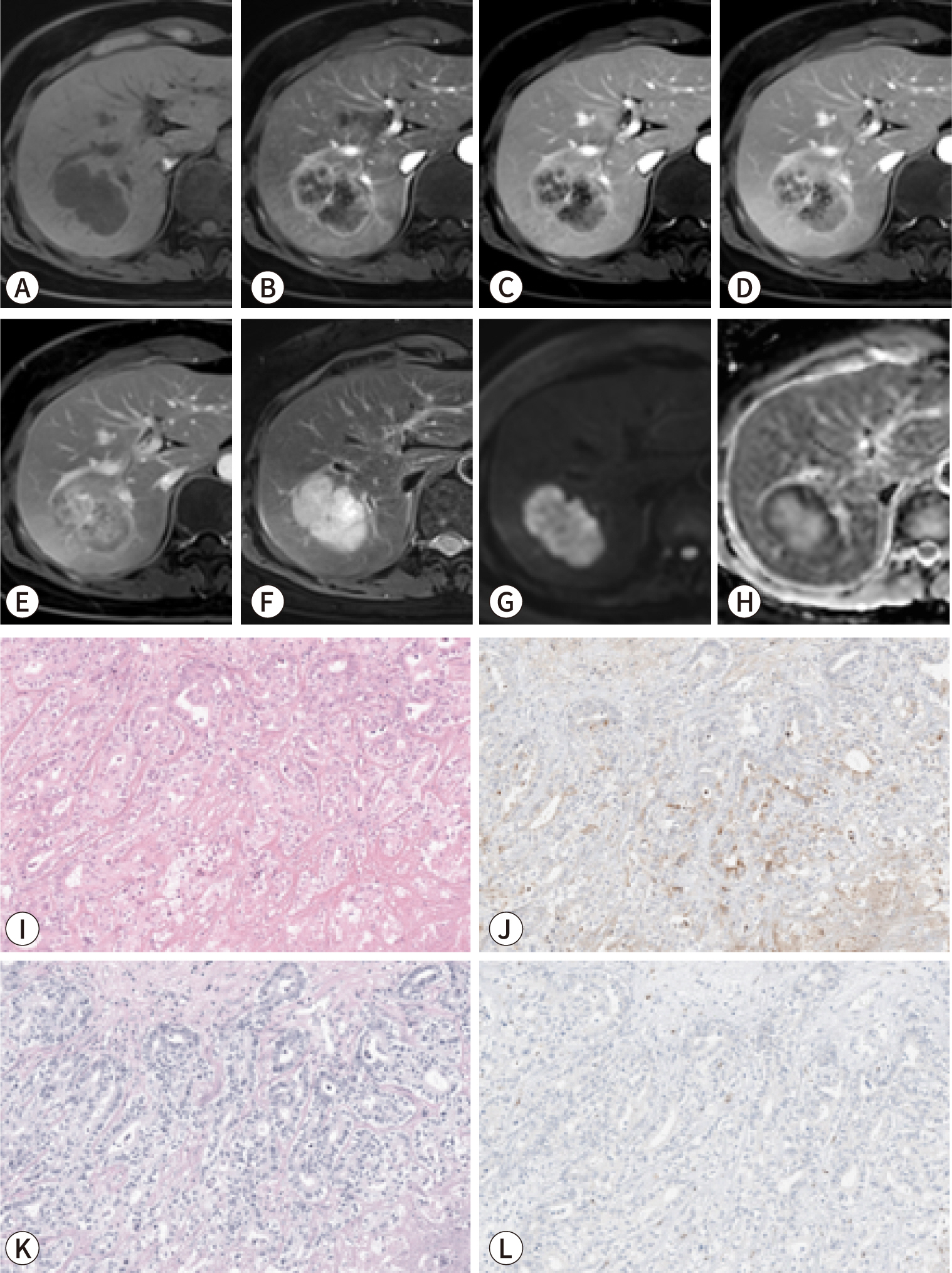
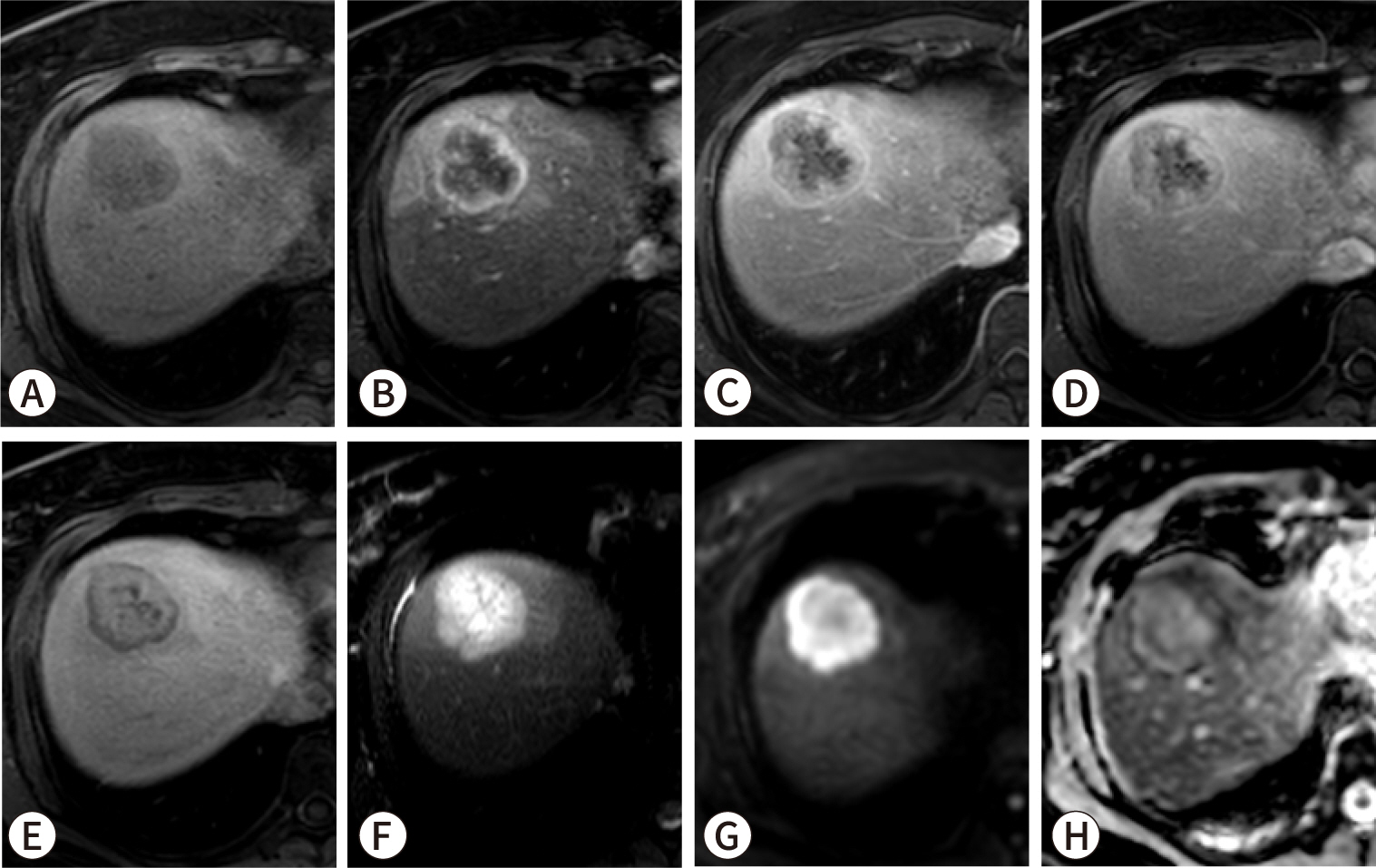
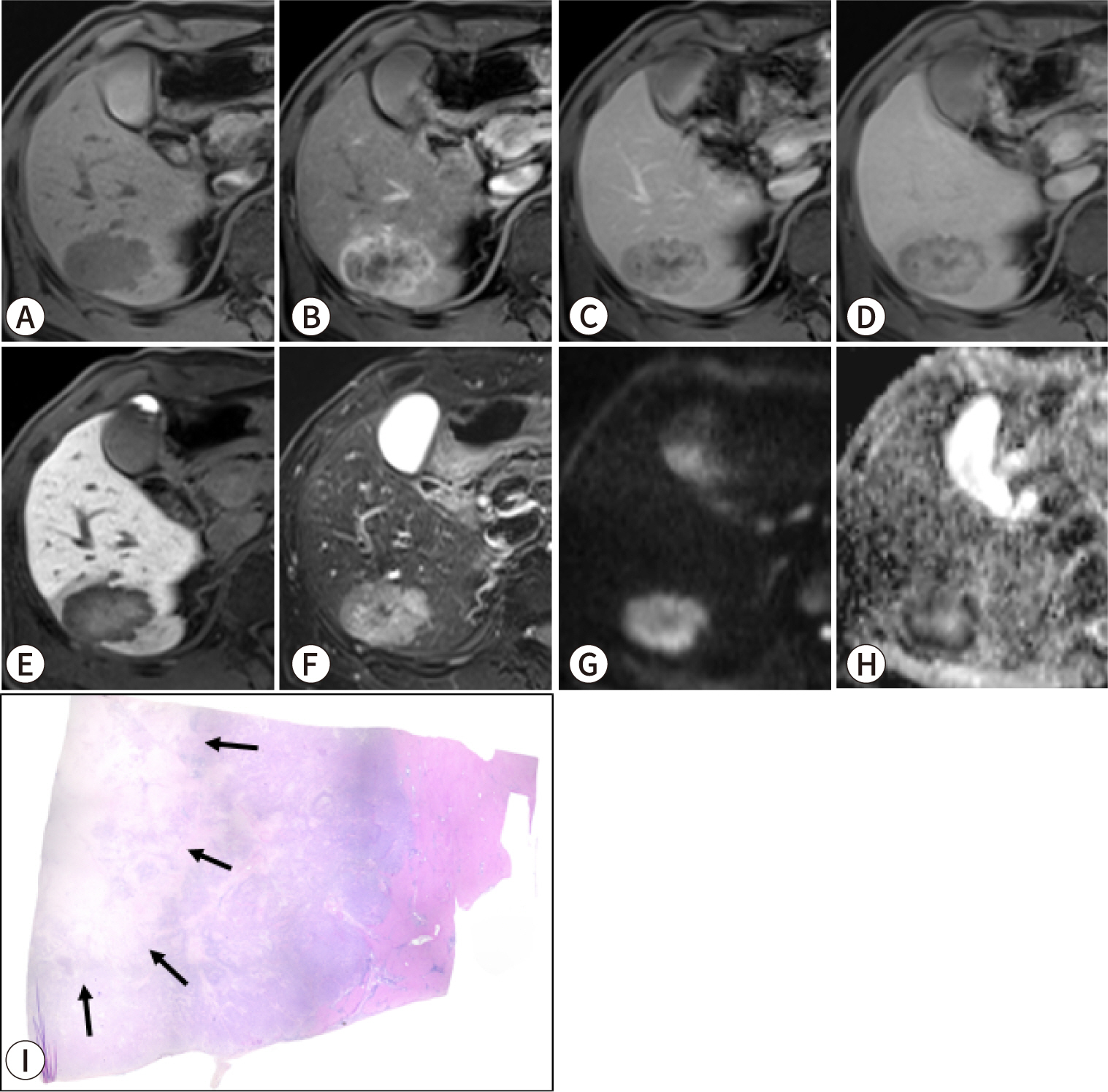
Fig. 2.
A 51-year-old female patient with small duct-type intrahepatic
cholangiocarcinoma (iCCA). Gadobutrol-enhanced MRI: (A) pre-contrast
T1-weighted, (B) arterial phase, (C) portal phase, (D) equilibrium
phase, (E) 15-minute delayed phase, (F) T2-weighted, and (G)
diffusion-weighted (b=800 s/mm2) images and (H) apparent
diffusion coefficient (ADC) map. Staining: (I) hematoxylin-eosin,
(J) C-reactive protein (CRP) immunohistochemical, (K) Alcian
blue/periodic acid-Schiff (AB/PAS), and (L) S100 calcium-binding
protein P (S100P) immunohistochemical staining (I–L, original
magnification ×200). The mass exhibits rim hyperenhancement
in the arterial phase (B) and a progressive centripetal pattern of
contrast filling in the portal (C), equilibrium (D), and delayed (F)
phases. It also displays moderate hyperintensity on the T2-weighted
image (F), and restriction on both the diffusion-weighted image and
the ADC map (G,H). No significant bile duct dilatation is evident in
the peritumoral area. The patient underwent right lobectomy, and a
diagnosis of small duct iCCA was confirmed through
immunohistochemical and special staining techniques. Specifically,
on pathologic examination, the lesion displayed positive CRP
expression (J), absence of mucin on AB/PAS staining (K), and
negative staining for S100P expression (L).
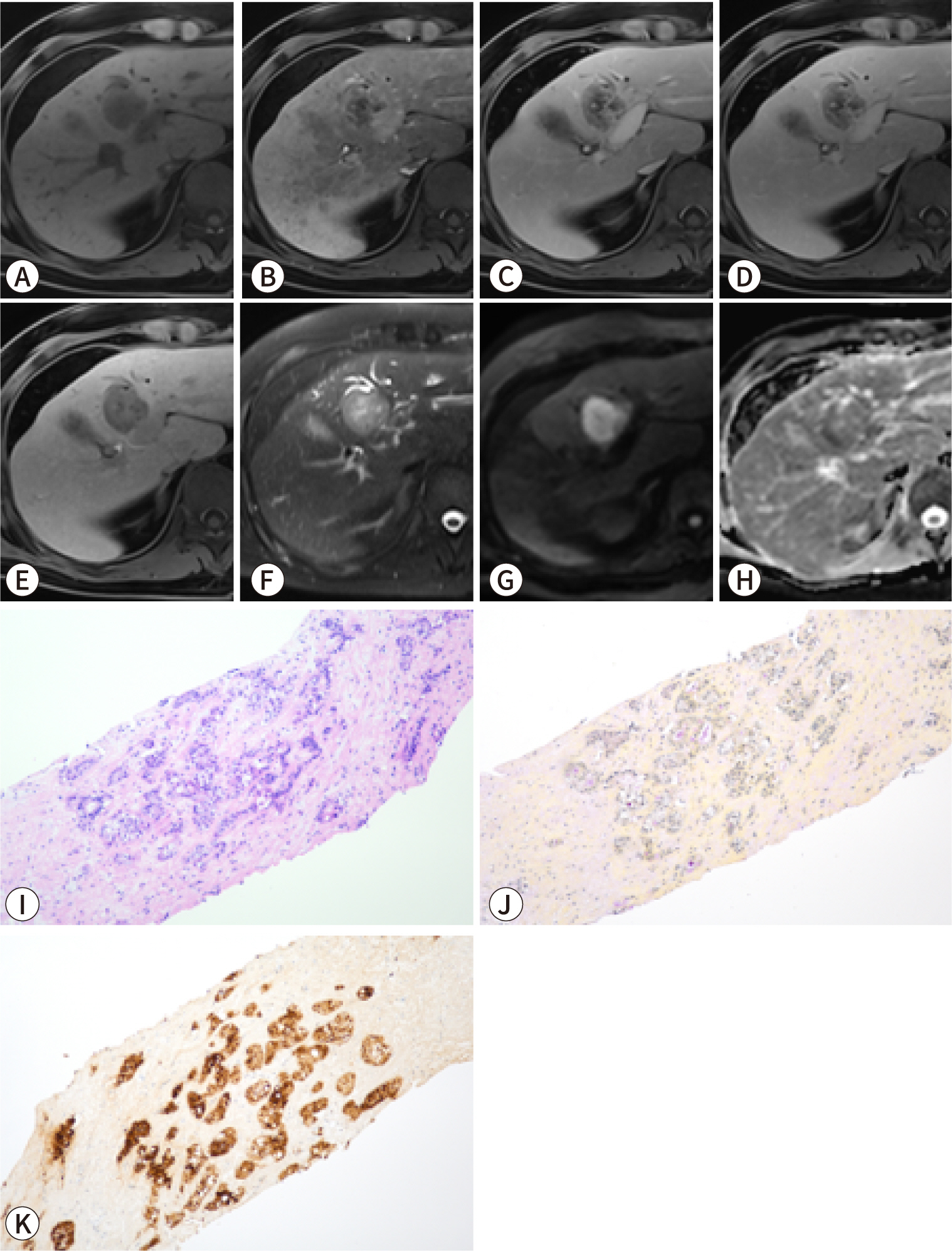
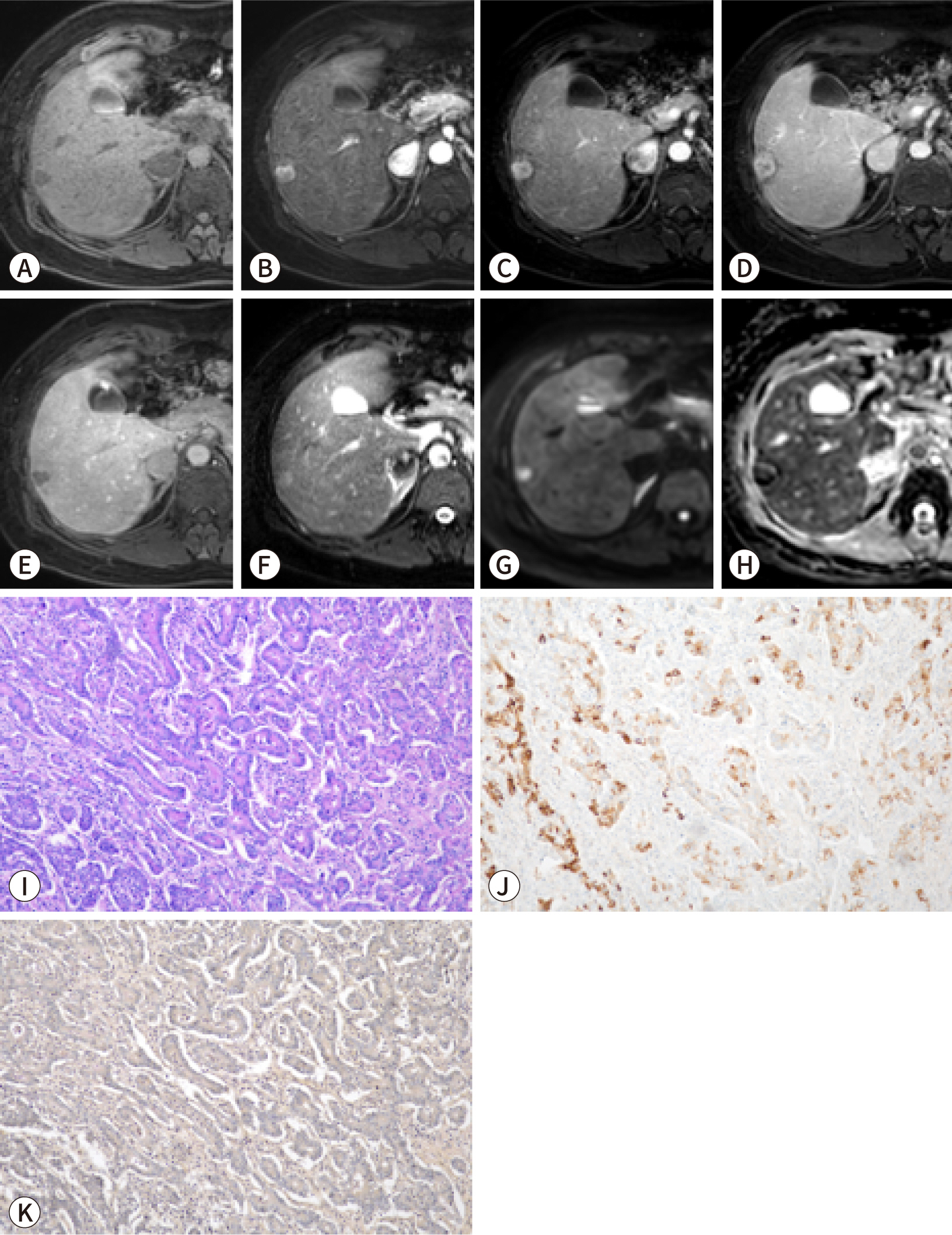
Fig. 3.
A 52-year-old male patient with large duct-type intrahepatic
cholangiocarcinoma (iCCA). Gadoxetic acid-enhanced MRI: (A)
pre-contrast T1-weighted, (B) arterial phase, (C) portal phase, (D)
transitional phase, (E) hepatobiliary phase, (F) T2-weighted, and
(G) diffusion-weighted (b=800 s/mm2) images and (H)
apparent diffusion coefficient (ADC) map. Staining: (I)
hematoxylin-eosin, (J) mucicarmine, and (K) S100 calcium-binding
protein P (S100P) immunohistochemical staining (I–K, original
magnification ×200). A well-defined 3.2-cm mass is evident in
segment 4 of the liver. The mass exhibits diffuse hypovascularity in
the arterial phase (B); hypointensity in the portal (C),
transitional (D), and hepatobiliary phases (E); adjacent bile duct
dilatation on the T2-weighted image (F); and restricted diffusion on
both the diffusion-weighted image and the ADC map (G,H). The patient
underwent percutaneous biopsy, and a diagnosis of large duct iCCA
was confirmed through immunohistochemical and special staining
techniques. Specifically, the tumor displayed positive expression of
both mucin (J) and S100P (K).
The imaging findings of the two types of iCCA closely align with their
pathogenesis and associated liver or bile duct diseases. SD-iCCA is
frequently accompanied by chronic hepatitis or cirrhosis, whereas LD-iCCA is
commonly associated with chronic bile duct diseases such as primary
sclerosing cholangitis, hepatolithiasis, or Clonorchis
sinensis infection [50–53].
Enhancement pattern of the tumor
The arterial enhancement pattern of iCCA is recognized as a key imaging-based
prognostic marker. Studies have shown that iCCA with arterial phase
hyperenhancement is associated with less invasive histopathological features
and better overall survival compared to iCCA with either diffuse
hypoenhancement or rim enhancement during the arterial phase (Fig. 1) [54–56].
Radiopathologic correlation studies have additionally established that MVD
is linked to arterial enhancement patterns. iCCA with low MVD typically
displays low arterial phase enhancement on imaging; furthermore, low MVD is
associated with a poor prognosis, along with aggressive pathological
features such as tumor multiplicity, MiVI, lymph node metastasis, and low
infiltration of CD8+ tumor-infiltrating lymphocytes [57,58].
Moreover, the enhancement pattern of iCCA is suspected to be associated with
its subclassification. SD-iCCA often exhibits arterial hyperenhancement,
resembling that seen in HCC or combined hepatocellular-CCA [59]. The arterial enhancement patterns
in LD-iCCA are more variable, ranging from diffuse hyperenhancement to rim
hyperenhancement and diffuse hypoenhancement [48].
Intratumoral fibrous stroma
Most iCCAs exhibit some degree of fibrous stroma. When scirrhous fibrous
stroma comprises more than 70% of the tumor area, the iCCA is classified as
scirrhous. Scirrhous iCCA is linked to a higher incidence of lymphatic and
perineural invasion and is associated with significantly worse survival
outcomes compared to non-scirrhous iCCA [60].
Intratumoral fibrosis can be assessed using dynamic CT or MRI.
Radiopathologic correlation studies have demonstrated that regions of
delayed enhancement are indicative of contrast retention within the fibrous
stroma of the tumor [61–63]. Furthermore, the degree of delayed
enhancement has been recognized as a prognostic marker for poor outcomes in
patients with MF-iCCA. Specifically, iCCAs that exhibit delayed enhancement
in more than two-thirds of the tumor on dynamic CT are associated with
scirrhous iCCA, a higher incidence of perineural invasion, and relatively
low overall survival [64].
Similarly, on gadoxetic acid-enhanced MRI, central intratumoral enhancement
observed during the hepatobiliary phase reflects the presence of fibrous
stroma within an iCCA lesion (Fig. 4)
[65,66]. During this phase, iCCAs containing fibrous stroma
exhibit an ill-defined hyperintense region set against a peripheral
hypointense area. This pattern is often described as the
“EOB-cloud,” a term derived from the chemical name of
gadoxetic acid, gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid
(Gd-EOB-DTPA) [66,67]. This cloud-like appearance results
from the extracellular accumulation of contrast in the central fibrous
stroma, while the periphery of the tumor typically contains a higher
proportion of tumor tissue and less fibrosis. Notably, MF-iCCAs in which
more than 50% of the area appears hyperintense or isointense during the
hepatobiliary phase tend to exhibit comparatively poor disease-free and
overall survival [68].
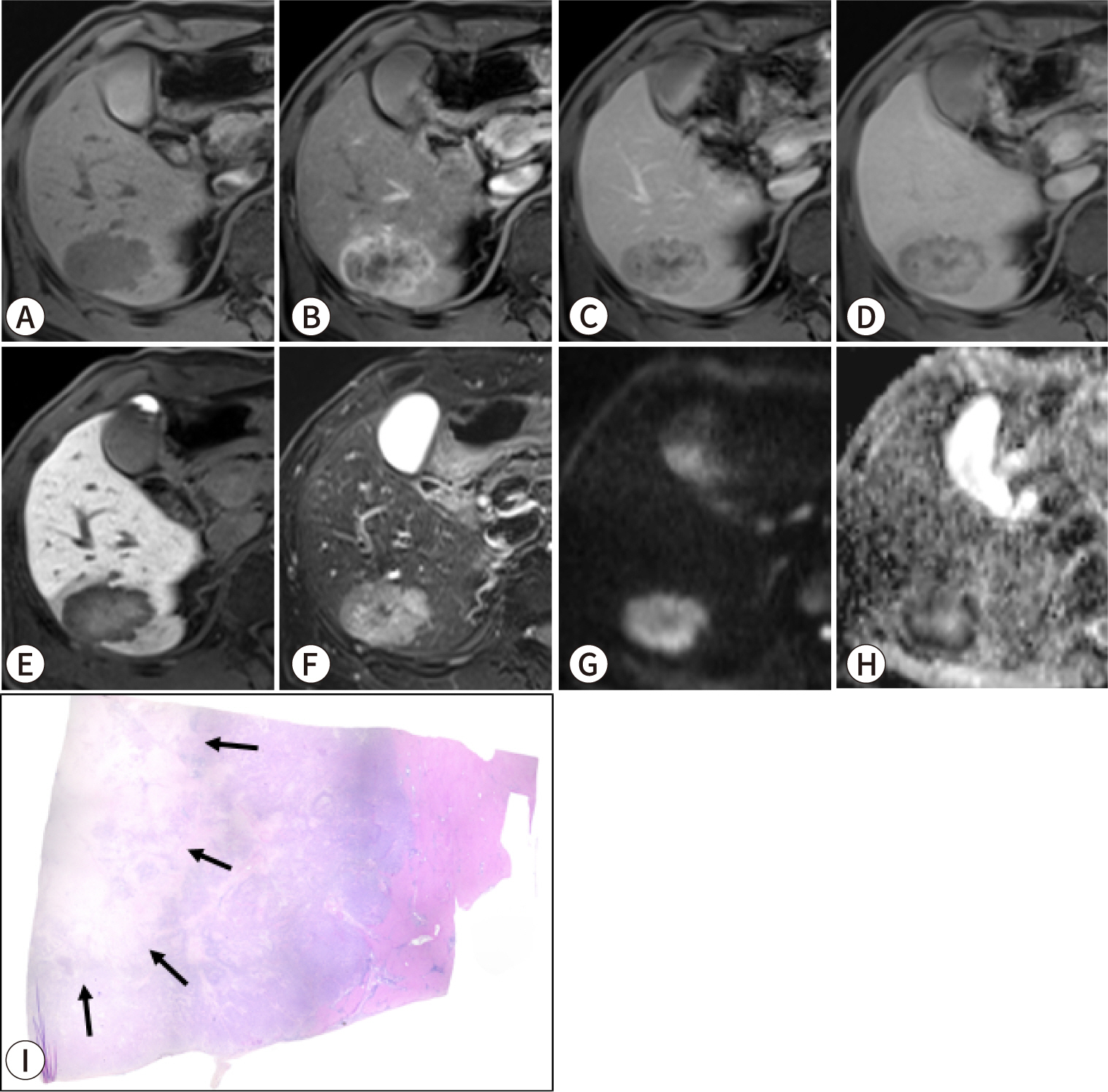
Fig. 4.
A 63-year-old male patient with intrahepatic cholangiocarcinoma
(iCCA) exhibiting a dense fibrous stroma. Gadoxetic acid-enhanced
MRI: (A) pre-contrast T1-weighted, (B) arterial phase, (C) portal
phase, (D) transitional phase, (E) hepatobiliary phase, (F)
T2-weighted, and (G) diffusion-weighted (b=800 s/mm2)
images and (H) apparent diffusion coefficient map. (I) Scan view
image of hematoxylin-eosin staining. MRI revealed an approximately
4.5-cm lobulated mass in the right posterior liver. The mass
exhibited thin-rim hyperenhancement in the arterial phase (B),
peripheral washout with progressive central enhancement in the
portal (C) and transitional (D) phases, and an
“EOB-cloud” appearance in the hepatobiliary phase (E),
as well as targetoid diffusion restriction (G,H). The patient
underwent extended right posterior sectionectomy, and the diagnosis
of iCCA was confirmed. The pathology specimen (I) displayed a dense
fibrotic area, corresponding to the “EOB-cloud area”
observed on MRI.
Imaging-based prognosis prediction model for intrahepatic
cholangiocarcinoma
Recent research has progressed from correlating imaging findings with
histopathologic characteristics associated with prognosis to creating models
that directly predict prognosis from imaging findings. These imaging-based
prognostic models can offer insights into patient outcomes before treatment is
initiated, potentially informing critical decisions about therapeutic
strategies.
A multicenter study proposed a preoperative prognostic model for resectable iCCA
that includes serum CA19-9 levels and three MRI findings: tumor multiplicity,
lymph node metastasis, and bile duct invasion [69]. In predicting overall survival, this imaging-based model
demonstrated comparable discriminatory performance to traditional pathologic
staging systems, such as the eighth edition AJCC TNM system, the MEGNA score,
and Nathan staging [69–71]. Another recent study introduced a more
sophisticated prognostic model for resectable iCCA, combining two serum markers
(CA19-9 >300 IU/mL and albumin ≤40 g/L) and six imaging findings
[72]. This model outperformed
pathologic staging systems, including the eighth edition AJCC and the MEGNA
score, in predicting disease-specific and disease-free survival [72].
Imaging-based models have also been reported for predicting the prognosis of
unresectable iCCA. The Fudan score, originally developed from a cohort of
patients with resectable iCCA, has been shown to be effective for prognostic
prediction in unresectable iCCA as well [73]. This score includes five variables: tumor diameter, the number
of intrahepatic tumors, the type of tumor boundary, serum alkaline phosphatase
levels, and CA19-9 levels. A recent study proposed a modified scoring system for
unresectable iCCA by incorporating an additional unfavorable prognostic
factor—high ADC—which improved the model’s performance in
predicting survival [74].
Utilizing imaging findings for treatment decision-making in intrahepatic
cholangiocarcinoma
Imaging is vital in the treatment decision-making process for iCCA, as it aids not
only in assessing resectability but also in determining the need for lymphadenectomy
during hepatic resection, deciding whether to administer neoadjuvant therapy, and
selecting targeted therapies.
Lymphadenectomy
Lymphadenectomy plays a crucial role in accurate staging and may reduce the risk
of recurrence; however, its impact on survival remains unclear. Although the
practice of lymph node dissection in patients with clinically positive lymph
nodes (cN+) has gained broader acceptance, the routine dissection of lymph nodes
in patients who lack clear evidence of lymph node metastases (clinically
negative lymph nodes, cN–) remains a topic of ongoing debate [75,76].
The AJCC staging system, EASL-ILCA guidelines, and National Comprehensive Cancer
Network (NCCN) clinical practice guidelines all endorse the routine dissection
of lymph nodes. The AJCC and EASL-ILCA guidelines specifically recommend the
removal of a minimum of six lymph nodes to ensure thorough nodal staging. In
comparison, the NCCN guidelines simply advises regional lymphadenectomy of the
porta hepatis [2,22,77]. Conversely,
Japanese guidelines do not provide a specific recommendation concerning routine
lymph node dissection [78].
In clinical practice, lymph node dissection is performed in about half of
patients, largely based on the surgeon’s discretion [79,80]. When deciding whether to perform lymph node dissection, imaging
findings play a key role. One study revealed that a risk score combining serum
carcinoembryonic antigen level (≥7 ng/mL), lymph nodes deemed suspicious
on MRI, and MRI evidence of bile duct invasion was significantly correlated with
the presence of pathological lymph node metastasis (Fig. 5) [46].
Moreover, among patients who had a high risk score but did not undergo lymph
node dissection, the researchers observed a higher likelihood of nodal
recurrence within 3 months after surgery [46]. Imaging results can therefore be instrumental in stratifying
the risk of lymph node metastasis, thus guiding the decision of whether to
perform lymph node dissection in patients at high risk.
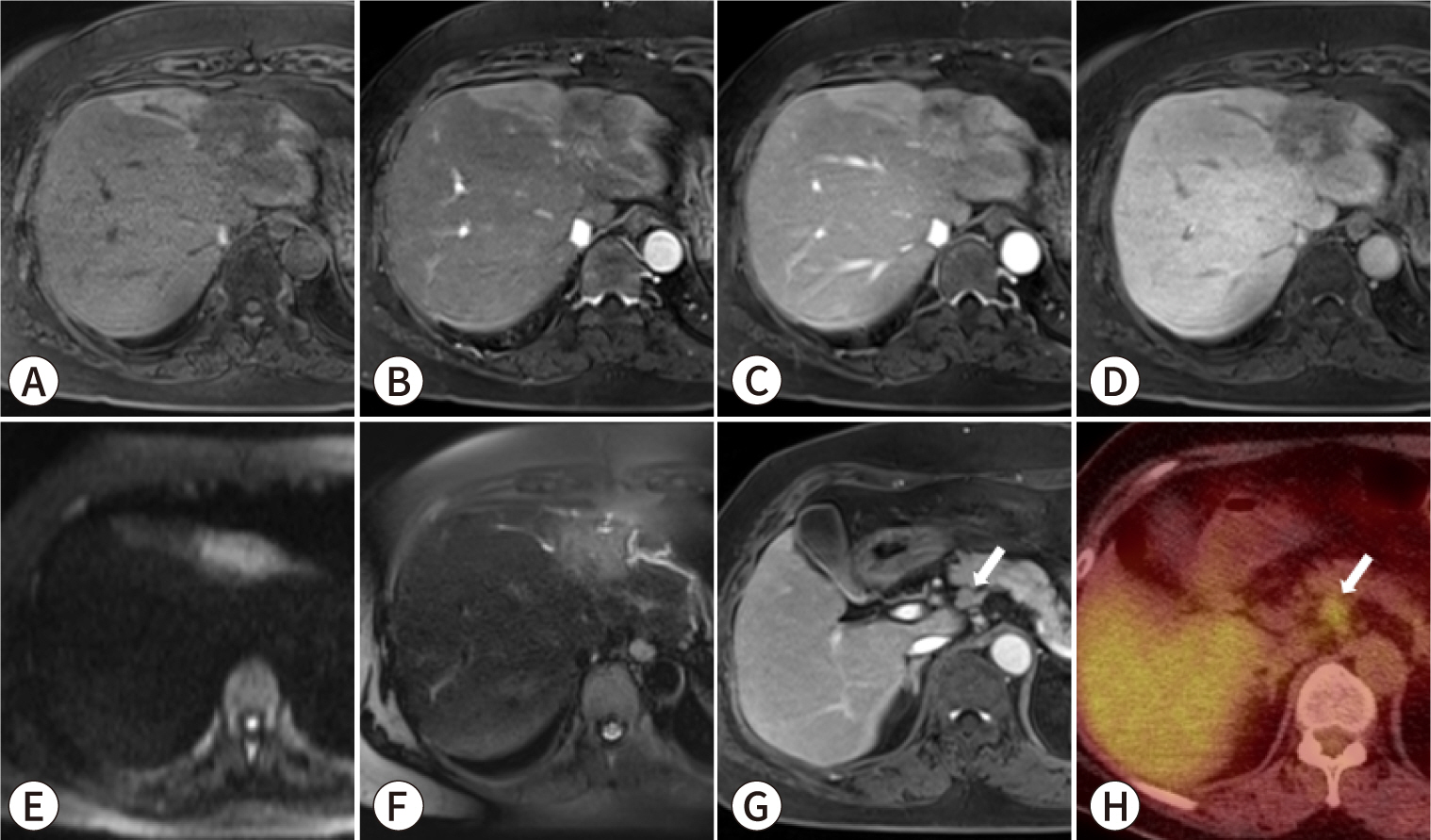
Fig. 5.
A 64-year-old female patient with intrahepatic cholangiocarcinoma
(iCCA) and lymph node metastasis. Gadoxetic acid-enhanced MRI,
comprising (A) pre-contrast T1-weighted, (B) arterial phase, (C) portal
phase, (D) hepatobiliary phase, (E) diffusion-weighted (b=800
s/mm2), and (F) T2-weighted images, reveals a 3.5-cm
infiltrative, poorly enhancing mass in the left lobe, with adjacent bile
duct dilatation. Additionally, the (G) portal phase image and (H)
18F-fluorodeoxyglucose (18F-FDG) positron
emission tomography-CT display an enlarged lymph node with increased
18F-FDG uptake situated adjacent to the common hepatic
artery (white arrows). The patient underwent left hepatic lobectomy with
lymph node dissection, and pathological examination confirmed the
diagnosis of iCCA with regional lymph node metastases.
Neoadjuvant therapy
Currently, the literature includes no prospective evidence specifically
supporting neoadjuvant therapy for iCCA, and no randomized studies have directly
compared neoadjuvant chemotherapy followed by surgery with surgery alone.
However, two retrospective studies, both analyzing data from the US National
Cancer Database, yielded notable findings.
One study demonstrated that patients with a higher clinical T stage or clinical
lymph node metastasis who received neoadjuvant therapy had better survival
outcomes than those who underwent upfront surgery [81]. Similarly, another study found that although no
survival benefit was observed in a propensity score-matched analysis across all
stages of iCCA, neoadjuvant therapy did confer a survival advantage in patients
with more advanced disease (stages II-III) [82].
As a result, guidelines vary in their recommendations concerning neoadjuvant
therapy for iCCA. The EASL-ILCA guideline states that neoadjuvant systemic
chemotherapy can be considered for patients with surgically challenging yet
resectable disease, especially when an R1 resection is anticipated [2]. In contrast, neither the NCCN nor the
Japanese guidelines provide specific recommendations for neoadjuvant therapy in
the context of iCCA [77,78]. Well-designed prospective trials are
necessary to further evaluate the role of neoadjuvant treatment in this
context.
Collectively, neoadjuvant therapy has been demonstrated to confer a survival
benefit in cases with a high T stage, suspected nodal metastasis, or a high
likelihood of positive resection margins. Considering that imaging-based
prognostic models are highly effective at predicting postoperative outcomes, the
use of imaging to identify high-risk patients who might benefit from neoadjuvant
therapy could represent a viable strategy [72].
Molecular profiling for targeted therapy
In recent years, targeted therapy has become increasingly important in the
treatment of iCCA [83]. The standard
first-line treatment consists of a combination of gemcitabine, cisplatin, and
durvalumab. However, targeted therapies are emerging as a viable second-line
option for patients with specific genetic mutations [2,77]. These
therapies require molecular profiling, often performed through next-generation
sequencing, which can be expensive. Molecular profiling is typically recommended
for patients with advanced-stage disease who need systemic therapy and for
early-stage patients at high risk of recurrence. Imaging findings can be
instrumental in identifying and stratifying these high-risk patients.
Currently, approved targeted therapies are available for genetic factors
including isocitrate dehydrogenase 1 (IDH1) mutation,
fibroblast growth factor receptor 2 (FGFR2) fusion,
BRAF V600E mutation, microsatellite instability-high and
mismatch repair-deficient cancers, and epidermal growth factor receptor 2
(HER2) overexpression [84–88]. Among these,
IDH1 mutation and FGFR2 fusion are
particularly impactful due to their comparatively high incidence [77]. These mutations are predominantly
observed in SD-iCCA [18]. Studies have
shown that iCCA with IDH1/2 mutations often presents with
pronounced arterial phase enhancement on imaging, a feature commonly associated
with SD-iCCA [89]. Given the higher
prevalence of targetable mutations such as IDH1 and
FGFR2 within the small duct type, molecular profiling may
be particularly promising when imaging findings suggest the presence of SD-iCCA
(Fig. 6). However, limited research is
available to support this recommendation.
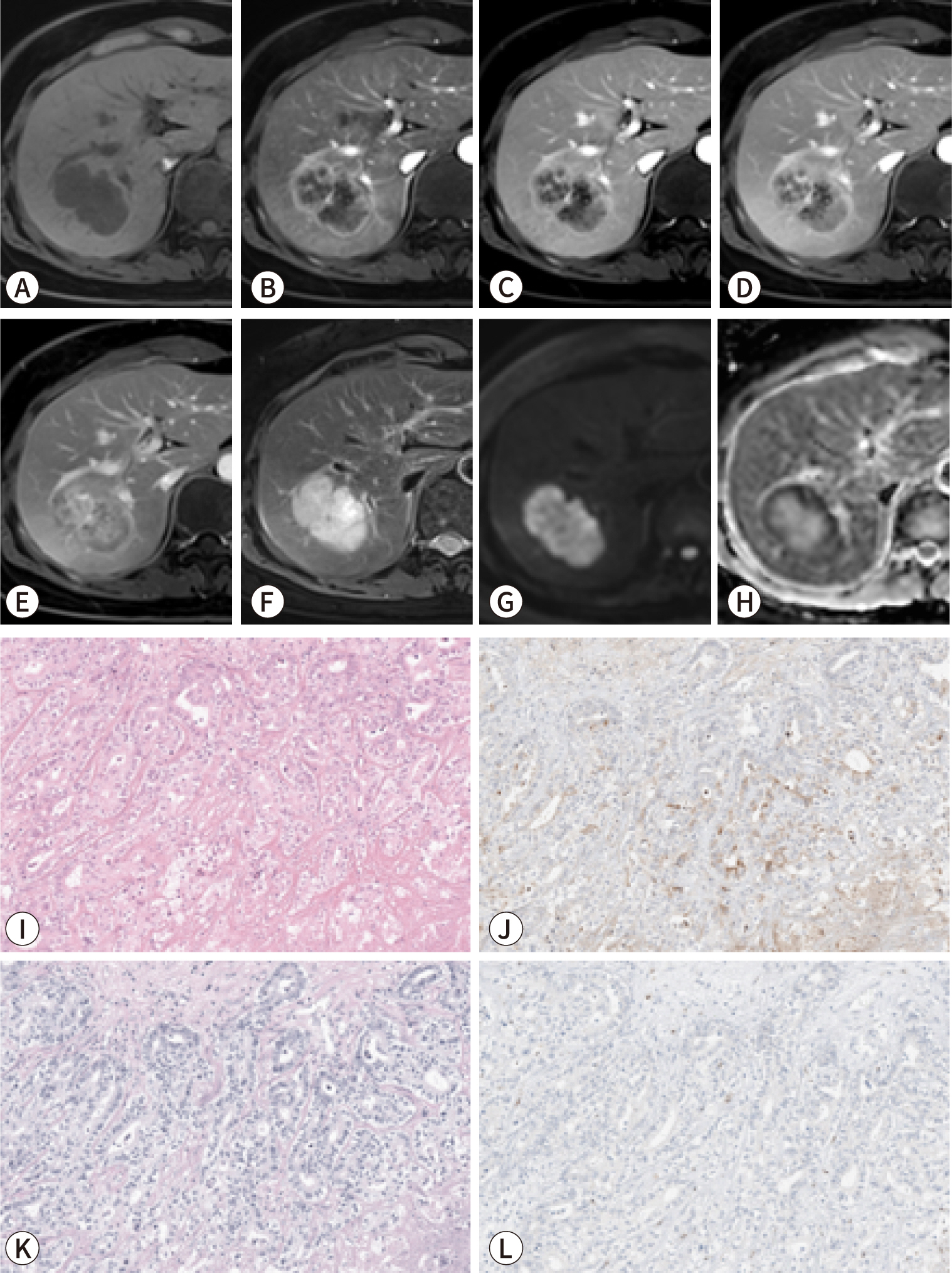
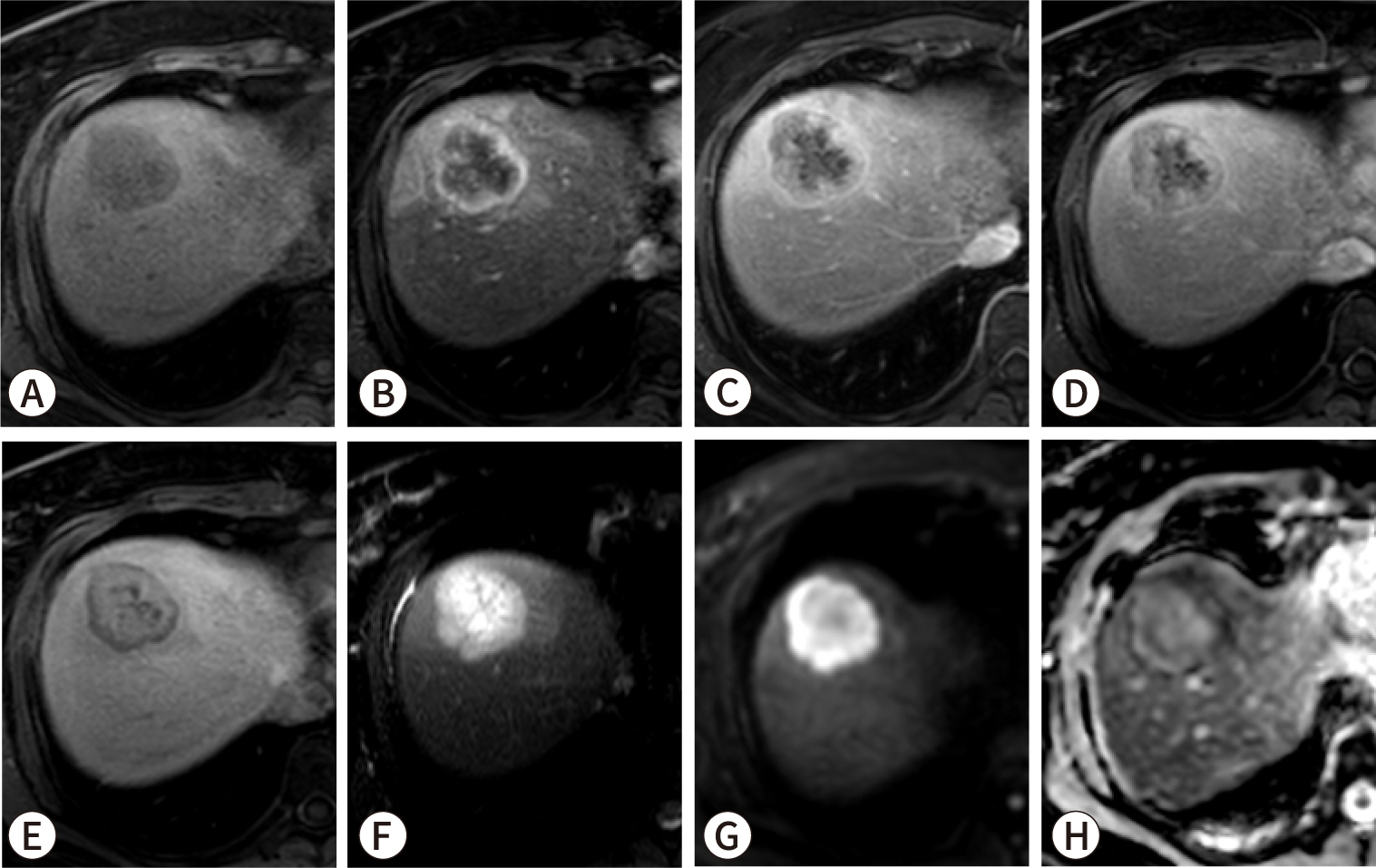
Fig. 6.
A 42-year-old female patient with intrahepatic cholangiocarcinoma
(iCCA) harboring an isocitrate dehydrogenase 1 (IDH1)
mutation. Gadoxetic acid-enhanced MRI, comprising (A) pre-contrast
T1-weighted, (B) arterial phase, (C) portal phase, (D) transitional
phase, (E) hepatobiliary phase, (F) T2-weighted, and (G)
diffusion-weighted (b=800 s/mm2) images, as well as (H)
apparent diffusion coefficient map, reveal a 4.5-cm well-defined mass in
the right liver dome. The mass exhibits rim hyperenhancement in the
arterial phase (B), a targetoid appearance in the transitional and
hepatobiliary phases (D,E), hyperintensity on the T2-weighted image (F),
and diffusion restriction (G,H). The lesion is situated peripherally in
the liver without evidence of adjacent biliary dilatation. The patient
underwent central lobectomy, and iCCA was confirmed. Next-generation
sequencing identified an IDH1 missense
mutation.
Conclusion
iCCA represents a serious and escalating global health concern, with a rising
incidence and persistently poor prognosis. However, advancements in pathology and
radiology have provided new insights into the disease. The histological
subclassification into SD-iCCA and LD-iCCA offers a valuable framework for
understanding the heterogeneity of iCCA and improving prognosis prediction.
Radiological studies that focus on various imaging findings, such as tumor size,
multiplicity, enhancement patterns, the presence of intratumoral fibrous stroma, and
suspicious lymph nodes, have demonstrated high utility in the pre-treatment
assessment of patients.
Importantly, imaging-based prognostic models for resectable iCCA have demonstrated
predictive accuracy comparable to that of traditional pathological staging systems.
Beyond predicting prognosis, imaging also offers critical insights that may inform
decisions about lymphadenectomy and neoadjuvant therapy. Furthermore, radiological
findings indicative of SD-iCCA could assist in identifying patients likely to harbor
clinically relevant mutations, such as IDH1 mutatios and
FGFR2 fusions.
These imaging-based approaches are essential for improving prognosis and tailoring
treatment strategies for patients with iCCA, thereby advancing personalized medicine
in this area. Nevertheless, to increase the utilization of imaging findings in
predicting prognosis and informing treatment decisions, higher-level evidence from
international multicenter prospective studies is necessary.
Authors' contributions
Project administration: Rhee H
Conceptualization: Rhee H
Methodology & data curation: Kang JG, Chung T, Kim DK, Rhee H
Funding acquisition: Rhee H
Writing – original draft: Kang JG, Rhee H
Writing – review & editing: Kang JG, Chung T, Kim DK, Rhee H
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant
funded by the Korea government (MSIT) (No. RS-2023-00208307).
Data availability
Not applicable.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Banales JM, Cardinale V, Carpino G, Marzioni M, Andersen JB, Invernizzi P, et al. Expert consensus document: cholangiocarcinoma: current knowledge
and future perspectives consensus statement from the European Network for
the Study of Cholangiocarcinoma (ENS-CCA). Nat Rev Gastroenterol Hepatol 2016;13(5):261-280.
2. European Association for the Study of the Liver. EASL-ILCA clinical practice guidelines on the management of
intrahepatic cholangiocarcinoma. J Hepatol 2023;79(1):181-208.
3. Banales JM, Marin JJG, Lamarca A, Rodrigues PM, Khan SA, Roberts LR, et al. Cholangiocarcinoma 2020: the next horizon in mechanisms and
management. Nat Rev Gastroenterol Hepatol 2020;17(9):557-588.
4. Yang JQ, Wang XG, Wu B. Incidence trend and prognosis of intrahepatic cholangiocarcinoma:
a study based on the SEER database. Transl Cancer Res 2023;12(11):3007-3015.
5. Seo N, Kim DY, Choi JY. Cross-sectional imaging of intrahepatic cholangiocarcinoma:
development, growth, spread, and prognosis. AJR Am J Roentgenol 2017;209(2):W64-W75.
6. Zhang Y, Uchida M, Abe T, Nishimura H, Hayabuchi N, Nakashima Y. Intrahepatic peripheral cholangiocarcinoma: comparison of dynamic
CT and dynamic MRI. J Comput Assist Tomogr 1999;23(5):670-677.
7. Kang Y, Lee JM, Kim SH, Han JK, Choi BI. Intrahepatic mass-forming cholangiocarcinoma: enhancement
patterns on gadoxetic acid–enhanced MR images. Radiology 2012;264(3):751-760.
9. Nam JG, Lee JM, Joo I, Ahn SJ, Park JY, Lee KB, et al. Intrahepatic mass-forming cholangiocarcinoma: relationship
between computed tomography characteristics and histological
subtypes. J Comput Assist Tomogr 2018;42(3):340-349.
10. Rhee H, Kim MJ, Park YN, An C. A proposal of imaging classification of intrahepatic mass-forming
cholangiocarcinoma into ductal and parenchymal types: clinicopathologic
significance. Eur Radiol 2019;29(6):3111-3121.
11. Bosman FT, Carneiro F, Hruban R, Theise N. WHO classification of tumours: digestive system tumours. 5th ed. Geneva: World Health Organization; 2019.
12. Komuta M. Intrahepatic cholangiocarcinoma: histological diversity and the
role of the pathologist. J Liver Cancer 2024;24(1):17-22.
13. Nakanuma Y, Sato Y, Harada K, Sasaki M, Xu J, Ikeda H. Pathological classification of intrahepatic cholangiocarcinoma
based on a new concept. World J Hepatol 2010;2(12):419-427.
14. Aishima S, Oda Y. Pathogenesis and classification of intrahepatic
cholangiocarcinoma: different characters of perihilar large duct type versus
peripheral small duct type. J Hepatobiliary Pancreat Sci 2015;22(2):94-100.
15. Jeon Y, Kwon SM, Rhee H, Yoo JE, Chung T, Woo HG, et al. Molecular and radiopathologic spectrum between HCC and
intrahepatic cholangiocarcinoma. Hepatology 2023;77(1):92-108.
16. Chung T, Rhee H, Nahm JH, Jeon Y, Yoo JE, Kim YJ, et al. Clinicopathological characteristics of intrahepatic
cholangiocarcinoma according to gross morphologic type: cholangiolocellular
differentiation traits and inflammation- and
proliferation-phenotypes. HPB 2020;22(6):864-873.
17. Nakanuma Y, Sasaki M, Sato Y, Ren X, Ikeda H, Harada K. Multistep carcinogenesis of perihilar cholangiocarcinoma arising
in the intrahepatic large bile ducts. World J Hepatol 2009;1(1):35-42.
19. Li Z, Nguyen Canh H, Takahashi K, Le Thanh D, Nguyen Thi Q, Yang R, et al. Histopathological growth pattern and vessel co-option in
intrahepatic cholangiocarcinoma. Med Mol Morphol 2024;57(3):200-217.
20. Sugita H, Nakanuma S, Gabata R, Tokoro T, Takei R, Okazaki M, et al. Clinicopathological features of cholangiolocarcinoma and impact
of tumor heterogeneity on prognosis: a single institution retrospective
study. Oncol Lett 2024;27(5):213
21. Hayashi A, Misumi K, Shibahara J, Arita J, Sakamoto Y, Hasegawa K, et al. Distinct clinicopathologic and genetic features of 2 histologic
subtypes of intrahepatic cholangiocarcinoma. Am J Surg Pathol 2016;40(8):1021-1030.
22. Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The eighth edition AJCC cancer staging manual: continuing to
build a bridge from a population-based to a more
"personalized" approach to cancer staging. CA Cancer J Clin 2017;67(2):93-99.
23. Kim Y, Moris DP, Zhang XF, Bagante F, Spolverato G, Schmidt C, et al. Evaluation of the 8th edition American Joint Commission on Cancer
(AJCC) staging system for patients with intrahepatic cholangiocarcinoma: a
surveillance, epidemiology, and end results (SEER) analysis. J Surg Oncol 2017;116(6):643-650.
24. Spolverato G, Bagante F, Weiss M, Alexandrescu S, Marques HP, Aldrighetti L, et al. Comparative performances of the 7th and the 8th editions of the
American Joint Committee on Cancer staging systems for intrahepatic
cholangiocarcinoma. J Surg Oncol 2017;115(6):696-703.
25. Kang SH, Hwang S, Lee YJ, Kim KH, Ahn CS, Moon DB, et al. Prognostic comparison of the 7th and 8th editions of the American
Joint Committee on Cancer staging system for intrahepatic
cholangiocarcinoma. J Hepatobiliary Pancreat Sci 2018;25(4):240-248.
26. Kim YY, Yeom SK, Shin H, Choi SH, Rhee H, Park JH, et al. Clinical staging of mass‐forming intrahepatic
cholangiocarcinoma: computed tomography versus magnetic resonance
imaging. Hepatol Commun 2021;5(12):2009-2018.
27. Hyder O, Hatzaras I, Sotiropoulos GC, Paul A, Alexandrescu S, Marques H, et al. Recurrence after operative management of intrahepatic
cholangiocarcinoma. Surgery 2013;153(6):811-818.
28. Ali SM, Clark CJ, Mounajjed T, Wu TT, Harmsen WS, Reid‐Lombardo KM, et al. Model to predict survival after surgical resection of
intrahepatic cholangiocarcinoma: the Mayo Clinic experience. HPB 2015;17(3):244-250.
29. Hwang S, Lee YJ, Song GW, Park KM, Kim KH, Ahn CS, et al. Prognostic impact of tumor growth type on 7th AJCC staging system
for intrahepatic cholangiocarcinoma: a single-center experience of 659
cases. J Gastrointest Surg 2015;19(7):1291-1304.
30. Doussot A, Gonen M, Wiggers JK, Groot-Koerkamp B, DeMatteo RP, Fuks D, et al. Recurrence patterns and disease-free survival after resection of
intrahepatic cholangiocarcinoma: preoperative and postoperative prognostic
models. J Am Coll Surg 2016;223(3):493-505e2.
35. Marion-Audibert AM, Vullierme MP, Ronot M, Mabrut JY, Sauvanet A, Zins M, et al. Routine MRI with DWI sequences to detect liver metastases in
patients with potentially resectable pancreatic ductal carcinoma and normal
liver CT: a prospective multicenter study. AJR Am J Roentgenol 2018;211(5):W217-W225.
36. Shao C, Chen J, Chen J, Shi J, Huang L, Qiu Y. Histological classification of microvascular invasion to predict
prognosis in intrahepatic cholangiocarcinoma. Int J Clin Exp Pathol 2017;10(7):7674-7681.
37. Hu LS, Weiss M, Popescu I, Marques HP, Aldrighetti L, Maithel SK, et al. Impact of microvascular invasion on clinical outcomes after
curative-intent resection for intrahepatic
cholangiocarcinoma. J Surg Oncol 2019;119(1):21-29.
39. Ma X, Liu L, Fang J, Rao S, Lv L, Zeng M, et al. MRI features predict microvascular invasion in intrahepatic
cholangiocarcinoma. Cancer Imaging 2020;20(1):40
40. Zhou Y, Zhou G, Zhang J, Xu C, Wang X, Xu P. Radiomics signature on dynamic contrast-enhanced MR images: a
potential imaging biomarker for prediction of microvascular invasion in
mass-forming intrahepatic cholangiocarcinoma. Eur Radiol 2021;31(9):6846-6855.
41. Kawarada Y, Yamagiwa K, Das BC. Analysis of the relationships between clinicopathologic factors
and survival time in intrahepatic cholangiocarcinoma. Am J Surg 2002;183(6):679-685.
43. Yamamoto Y, Turkoglu MA, Aramaki T, Sugiura T, Okamura Y, Ito T, et al. Vascularity of intrahepatic cholangiocarcinoma on computed
tomography is predictive of lymph node metastasis. Ann Surg Oncol 2016;23:Suppl 4. 485-493.
44. Meng ZW, Lin XQ, Zhu JH, Han SH, Chen YL. A nomogram to predict lymph node metastasis before resection in
intrahepatic cholangiocarcinoma. J Surg Res 2018;226:56-63.
46. Rhee H, Lim HJ, Han K, Yeom SK, Choi SH, Park JH, et al. A preoperative scoring system to predict lymph node metastasis in
intrahepatic cholangiocarcinoma. Hepatol Int 2023;17(4):942-953.
47. Huang X, Yang J, Li J, Xiong Y. Comparison of magnetic resonance imaging and 18-fludeoxyglucose
positron emission tomography/computed tomography in the diagnostic accuracy
of staging in patients with cholangiocarcinoma: a
meta-analysis. Medicine 2020;99(35):e20932.
48. Park S, Lee Y, Kim H, Yu MH, Lee ES, Yoon JH, et al. Subtype classification of intrahepatic cholangiocarcinoma using
liver MR imaging features and its prognostic value. Liver Cancer 2022;11(3):233-246.
55. Nanashima A, Abo T, Murakami G, Matsumoto A, Tou K, Takeshita H, et al. Intrahepatic cholangiocarcinoma: relationship between tumor
imaging enhancement by measuring attenuation and clinicopathologic
characteristics. Abdom Imaging 2013;38(4):785-792.
56. Min JH, Kim YK, Choi SY, Kang TW, Lee SJ, Kim JM, et al. Intrahepatic mass-forming cholangiocarcinoma: arterial
enhancement patterns at MRI and prognosis. Radiology 2019;290(3):691-699.
57. Yugawa K, Itoh S, Yoshizumi T, Iseda N, Tomiyama T, Toshima T, et al. Prognostic impact of tumor microvessels in intrahepatic
cholangiocarcinoma: association with tumor-infiltrating
lymphocytes. Mod Pathol 2021;34(4):798-807.
58. Vigano L, Soldani C, Franceschini B, Cimino M, Lleo A, Donadon M, et al. Tumor-infiltrating lymphocytes and macrophages in intrahepatic
cholangiocellular carcinoma. Impact on prognosis after complete
surgery. J Gastrointest Surg 2019;23(11):2216-2224.
59. Rhee H, Park JH, Park YN. Update on pathologic and radiologic diagnosis of combined
hepatocellular-cholangiocarcinoma. J Liver Cancer 2021;21(1):12-24.
60. Kajiyama K, Maeda T, Takenaka K, Sugimachi K, Tsuneyoshi M. The significance of stromal desmoplasia in intrahepatic
cholangiocarcinoma: a special reference of 'scirrhous-type'
and 'nonscirrhous-type' growth. Am J Surg Pathol 1999;23(8):892-902.
62. Yoshikawa J, Matsui O, Kadoya M, Gabata T, Arai K, Takashima T. Delayed enhancement of fibrotic areas in hepatic masses:
CT–pathologic correlation. J Comput Assist Tomogr 1992;16(2):206-211.
63. Valls C, Gumà A, Puig I, Sanchez A, Andía E, Serrano T, et al. Intrahepatic peripheral cholangiocarcinoma: CT
evaluation. Abdom Imaging 2000;25(5):490-496.
64. Asayama Y, Yoshimitsu K, Irie H, Tajima T, Nishie A, Hirakawa M, et al. Delayed-phase dynamic CT enhancement as a prognostic factor for
mass-forming intrahepatic cholangiocarcinoma. Radiology 2006;238(1):150-155.
65. Jeong HT, Kim MJ, Chung YE, Choi JY, Park YN, Kim KW. Gadoxetate disodium–enhanced MRI of mass-forming
intrahepatic cholangiocarcinomas: imaging-histologic
correlation. AJR Am J Roentgenol 2013;201(4):W603-W611.
66. Kim SH, Lee CH, Kim BH, Kim WB, Yeom SK, Kim KA, et al. Typical and atypical imaging findings of intrahepatic
cholangiocarcinoma using gadolinium ethoxybenzyl diethylenetriamine
pentaacetic acid-enhanced magnetic resonance imaging. J Comput Assist Tomogr 2012;36(6):704-709.
68. Koh J, Chung YE, Nahm JH, Kim HY, Kim KS, Park YN, et al. Intrahepatic mass-forming cholangiocarcinoma: prognostic value of
preoperative gadoxetic acid-enhanced MRI. Eur Radiol 2016;26(2):407-416.
69. Rhee H, Choi SH, Park JH, Cho ES, Yeom SK, Park S, et al. Preoperative magnetic resonance imaging-based prognostic model
for mass-forming intrahepatic cholangiocarcinoma. Liver Int 2022;42(4):930-941.
70. Nathan H, Aloia TA, Vauthey JN, Abdalla EK, Zhu AX, Schulick RD, et al. A proposed staging system for intrahepatic
cholangiocarcinoma. Ann Surg Oncol 2009;16(1):14-22.
71. Raoof M, Dumitra S, Ituarte PHG, Melstrom L, Warner SG, Fong Y, et al. Development and validation of a prognostic score for intrahepatic
cholangiocarcinoma. JAMA Surg 2017;152(5):e170117
72. Ji GW, Xu Q, Jiao CY, Lu M, Xu ZG, Zhang B, et al. Translating imaging traits of mass-forming intrahepatic
cholangiocarcinoma into the clinic: from prognostic to therapeutic
insights. JHEP Rep 2023;5(10):100839
73. Jiang W, Zeng ZC, Tang ZY, Fan J, Sun HC, Zhou J, et al. A prognostic scoring system based on clinical features of
intrahepatic cholangiocarcinoma: the Fudan score. Ann Oncol 2011;22(7):1644-1652.
74. Pandey A, Mohseni A, Shaghaghi M, Pandey P, Rezvani Habibabadi R, Hazhirkarzar B, et al. Incremental value of volumetric multiparametric MRI over Fudan
score for prognosis of unresectable intrahepatic cholangiocarcinoma treated
with systemic chemotherapy. Eur J Radiol 2024;170:111196
75. Sposito C, Droz dit Busset M, Virdis M, Citterio D, Flores M, Bongini M, et al. The role of lymphadenectomy in the surgical treatment of
intrahepatic cholangiocarcinoma: a review. Eur J Surg Oncol 2022;48(1):150-159.
76. Sposito C, Ratti F, Cucchetti A, Ardito F, Ruzzenente A, Di Sandro S, et al. Survival benefit of adequate lymphadenectomy in patients
undergoing liver resection for clinically node-negative intrahepatic
cholangiocarcinoma. J Hepatol 2023;78(2):356-363.
78. Kubo S, Shinkawa H, Asaoka Y, Ioka T, Igaki H, Izumi N, et al. Liver cancer study group of Japan clinical practice guidelines
for intrahepatic cholangiocarcinoma. Liver Cancer 2022;11(4):290-314.
79. Clark CJ, Wood-Wentz CM, Reid-Lombardo KM, Kendrick ML, Huebner M, Que FG. Lymphadenectomy in the staging and treatment of intrahepatic
cholangiocarcinoma: a population-based study using the National Cancer
Institute SEER database. HPB 2011;13(9):612-620.
80. Zhang XF, Chen Q, Kimbrough CW, Beal EW, Lv Y, Chakedis J, et al. Lymphadenectomy for intrahepatic cholangiocarcinoma: has nodal
evaluation been increasingly adopted by surgeons over time? A national
database analysis. J Gastrointest Surg 2018;22(4):668-675.
81. Mason MC, Massarweh NN, Tzeng CWD, Chiang YJ, Chun YS, Aloia TA, et al. Time to rethink upfront surgery for resectable intrahepatic
cholangiocarcinoma? Implications from the neoadjuvant
experience. Ann Surg Oncol 2021;28(11):6725-6735.
82. Utuama O, Permuth JB, Dagne G, Sanchez-Anguiano A, Alman A, Kumar A, et al. Neoadjuvant chemotherapy for intrahepatic cholangiocarcinoma: a
propensity score survival analysis supporting use in patients with high-risk
disease. Ann Surg Oncol 2021;28(4):1939-1949.
85. Zhu AX, Macarulla T, Javle MM, Kelley RK, Lubner SJ, Adeva J, et al. Final overall survival efficacy results of ivosidenib for
patients with advanced cholangiocarcinoma with IDH1 mutation: the phase 3
randomized clinical ClarIDHy trial. JAMA Oncol 2021;7(11):1669-1677.
86. Goyal L, Meric-Bernstam F, Hollebecque A, Valle JW, Morizane C, Karasic TB, et al. Futibatinib for FGFR2-rearranged intrahepatic
cholangiocarcinoma. N Engl J Med 2023;388(3):228-239.
88. Maio M, Ascierto PA, Manzyuk L, Motola-Kuba D, Penel N, Cassier PA, et al. Pembrolizumab in microsatellite instability high or mismatch
repair deficient cancers: updated analysis from the phase II KEYNOTE-158
study. Ann Oncol 2022;33(9):929-938.
89. Zhu Y, Chen J, Kong W, Mao L, Kong W, Zhou Q, et al. Predicting IDH mutation status of intrahepatic
cholangiocarcinomas based on contrast-enhanced CT features. Eur Radiol 2018;28(1):159-169.
Imaging differentiation of hepatocellular carcinoma, combined hepatocellular-cholangiocarcinoma, and intrahepatic cholangiocarcinoma: pitfalls and advances Jaeseung Shin, Taek Chung, Sang Yun Ha, Hyungjin Rhee Journal of Liver Cancer.2026; 26(1): 9. CrossRef
Diagnostic performance and generalizability of preoperative prediction models for lymph node metastasis in intrahepatic cholangiocarcinoma: a multimodal evidence synthesis Zhihao Zhang, Peng Lei, Jinhua Hu, Jiayu Wu, Qi Wu, Changhui Huang, Xiqi Zhu BMC Cancer.2026;[Epub] CrossRef
Advances in the imaging of liver cancer Ijin Joo, Jeong Min Lee, Maxime Ronot Journal of Hepatology.2026;[Epub] CrossRef
Preoperative Assessment of Bile Duct Cancer: The Role of Magnetic Resonance Imaging and Magnetic Resonance Cholangiopancreatography Bohyun Kim Investigative Magnetic Resonance Imaging.2026; 30(2): 75. CrossRef
Imaging findings of intrahepatic cholangiocarcinoma for prognosis
prediction and treatment decision-making: a narrative review
Fig. 1.
A 34-year-old female patient with liver cirrhosis and small
duct-type intrahepatic cholangiocarcinoma (iCCA). Gadoxetic
acid-enhanced MRI: (A) pre-contrast T1-weighted, (B) arterial phase,
(C) portal phase, (D) transitional phase, (E) hepatobiliary phase,
(F) T2-weighted, and (G) diffusion-weighted (b=800 s/mm2)
images and (H) apparent diffusion coefficient map. Staining: (I)
hematoxylin-eosin, (J) C-reactive protein (CRP) immunohistochemical,
and (K) mucicarmine staining (I–K, original magnification
×200). The gadoxetic acid-enhanced MRI reveals a 1.5-cm round
mass in the subcapsular area of the right liver. The mass exhibits
hyperenhancement in the arterial phase (B), does not show washout in
the portal phase (C), and appears hypointense in the hepatobiliary
phase (E). Pathological examination confirmed the lesion as a small
duct iCCA with positive CRP expression (J) and the absence of mucin
under mucicarmine staining (K).
Fig. 2.
A 51-year-old female patient with small duct-type intrahepatic
cholangiocarcinoma (iCCA). Gadobutrol-enhanced MRI: (A) pre-contrast
T1-weighted, (B) arterial phase, (C) portal phase, (D) equilibrium
phase, (E) 15-minute delayed phase, (F) T2-weighted, and (G)
diffusion-weighted (b=800 s/mm2) images and (H) apparent
diffusion coefficient (ADC) map. Staining: (I) hematoxylin-eosin,
(J) C-reactive protein (CRP) immunohistochemical, (K) Alcian
blue/periodic acid-Schiff (AB/PAS), and (L) S100 calcium-binding
protein P (S100P) immunohistochemical staining (I–L, original
magnification ×200). The mass exhibits rim hyperenhancement
in the arterial phase (B) and a progressive centripetal pattern of
contrast filling in the portal (C), equilibrium (D), and delayed (F)
phases. It also displays moderate hyperintensity on the T2-weighted
image (F), and restriction on both the diffusion-weighted image and
the ADC map (G,H). No significant bile duct dilatation is evident in
the peritumoral area. The patient underwent right lobectomy, and a
diagnosis of small duct iCCA was confirmed through
immunohistochemical and special staining techniques. Specifically,
on pathologic examination, the lesion displayed positive CRP
expression (J), absence of mucin on AB/PAS staining (K), and
negative staining for S100P expression (L).
Fig. 3.
A 52-year-old male patient with large duct-type intrahepatic
cholangiocarcinoma (iCCA). Gadoxetic acid-enhanced MRI: (A)
pre-contrast T1-weighted, (B) arterial phase, (C) portal phase, (D)
transitional phase, (E) hepatobiliary phase, (F) T2-weighted, and
(G) diffusion-weighted (b=800 s/mm2) images and (H)
apparent diffusion coefficient (ADC) map. Staining: (I)
hematoxylin-eosin, (J) mucicarmine, and (K) S100 calcium-binding
protein P (S100P) immunohistochemical staining (I–K, original
magnification ×200). A well-defined 3.2-cm mass is evident in
segment 4 of the liver. The mass exhibits diffuse hypovascularity in
the arterial phase (B); hypointensity in the portal (C),
transitional (D), and hepatobiliary phases (E); adjacent bile duct
dilatation on the T2-weighted image (F); and restricted diffusion on
both the diffusion-weighted image and the ADC map (G,H). The patient
underwent percutaneous biopsy, and a diagnosis of large duct iCCA
was confirmed through immunohistochemical and special staining
techniques. Specifically, the tumor displayed positive expression of
both mucin (J) and S100P (K).
Fig. 4.
A 63-year-old male patient with intrahepatic cholangiocarcinoma
(iCCA) exhibiting a dense fibrous stroma. Gadoxetic acid-enhanced
MRI: (A) pre-contrast T1-weighted, (B) arterial phase, (C) portal
phase, (D) transitional phase, (E) hepatobiliary phase, (F)
T2-weighted, and (G) diffusion-weighted (b=800 s/mm2)
images and (H) apparent diffusion coefficient map. (I) Scan view
image of hematoxylin-eosin staining. MRI revealed an approximately
4.5-cm lobulated mass in the right posterior liver. The mass
exhibited thin-rim hyperenhancement in the arterial phase (B),
peripheral washout with progressive central enhancement in the
portal (C) and transitional (D) phases, and an
“EOB-cloud” appearance in the hepatobiliary phase (E),
as well as targetoid diffusion restriction (G,H). The patient
underwent extended right posterior sectionectomy, and the diagnosis
of iCCA was confirmed. The pathology specimen (I) displayed a dense
fibrotic area, corresponding to the “EOB-cloud area”
observed on MRI.
Fig. 5.
A 64-year-old female patient with intrahepatic cholangiocarcinoma
(iCCA) and lymph node metastasis. Gadoxetic acid-enhanced MRI,
comprising (A) pre-contrast T1-weighted, (B) arterial phase, (C) portal
phase, (D) hepatobiliary phase, (E) diffusion-weighted (b=800
s/mm2), and (F) T2-weighted images, reveals a 3.5-cm
infiltrative, poorly enhancing mass in the left lobe, with adjacent bile
duct dilatation. Additionally, the (G) portal phase image and (H)
18F-fluorodeoxyglucose (18F-FDG) positron
emission tomography-CT display an enlarged lymph node with increased
18F-FDG uptake situated adjacent to the common hepatic
artery (white arrows). The patient underwent left hepatic lobectomy with
lymph node dissection, and pathological examination confirmed the
diagnosis of iCCA with regional lymph node metastases.
Fig. 6.
A 42-year-old female patient with intrahepatic cholangiocarcinoma
(iCCA) harboring an isocitrate dehydrogenase 1 (IDH1)
mutation. Gadoxetic acid-enhanced MRI, comprising (A) pre-contrast
T1-weighted, (B) arterial phase, (C) portal phase, (D) transitional
phase, (E) hepatobiliary phase, (F) T2-weighted, and (G)
diffusion-weighted (b=800 s/mm2) images, as well as (H)
apparent diffusion coefficient map, reveal a 4.5-cm well-defined mass in
the right liver dome. The mass exhibits rim hyperenhancement in the
arterial phase (B), a targetoid appearance in the transitional and
hepatobiliary phases (D,E), hyperintensity on the T2-weighted image (F),
and diffusion restriction (G,H). The lesion is situated peripherally in
the liver without evidence of adjacent biliary dilatation. The patient
underwent central lobectomy, and iCCA was confirmed. Next-generation
sequencing identified an IDH1 missense
mutation.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Imaging findings of intrahepatic cholangiocarcinoma for prognosis
prediction and treatment decision-making: a narrative review
Comparison of characteristics between small duct and large duct
iCCA