1Division of Infective Diseases, Department of Internal Medicine and AIDS Research Institute, Yonsei University College of Medicine, Seoul, Korea
*Corresponding author: Nam Su Ku,
Division of Infective Diseases, Department of Internal Medicine and AIDS
Research Institute, Yonsei University College of Medicine, 50-1, Yonsei-Ro,
Seodaemun-gu, Seoul 03722, Korea, E-mail:
smileboy9@yuhs.ac
• Received: June 15, 2024 • Revised: July 17, 2024 • Accepted: July 17, 2024
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
The availability of combined antiretroviral therapy has significantly reduced the
number of new HIV infections and the associated mortality, and HIV infection has
become a chronic disease with long-term survival. In Korea, more than 1,000 new
HIV infections have been registered annually since 2013. After peaking at 1,223
in 2019, the number of new infections decreased between 2020 and 2023. In 2023,
the majority of newly HIV-infected people were men, and the proportions of young
people under 40 years, homosexual contacts and foreigners increased. Acquired
immunodeficiency syndrome (AIDS)-related deaths from opportunistic infections
associated with immunosuppression and AIDS-defining cancers are gradually
decreasing, whereas non-AIDS defining comorbidities such as non-AIDS defining
cancers, cardiovascular disease and metabolic complications are emerging as
major causes of death. Since the introduction of zidovudine, approximately 30
antiretroviral drugs have been approved for the treatment of HIV infection.
Early and continuous antiretroviral treatment for all people living with HIV is
an effective strategy for maintaining viral suppression and preventing
transmission of HIV infection. In conclusion, achieving the
95–95–95 target among those living with HIV in Korea requires
multifaceted efforts to improve early diagnosis, early and proper treatment of
HIV infection including the management of chronic diseases, and adherence to
antiretroviral therapy.
Since the first report of acquired immunodeficiency syndrome (AIDS) in 1981, the
epidemiology of HIV has changed markedly worldwide [1]. Over the past 40 years, the global HIV epidemic has continued, and
successful treatments and prevention methods have been developed and disseminated
[1]. Before the introduction of
antiretroviral therapy (ART) in the late 1990s, HIV infection had a high mortality
rate and a devastating effect on people of almost every race, country and class
worldwide. The availability of combined ART (cART) has significantly reduced the
prevalence and mortality of HIV infection, which has become a chronic disease with
long-term survival [1].
The Joint United Nations Programme on HIV/AIDS (UNAIDS) has declared a fight against
HIV transmission. In 2014, the UNAIDS proposed the 90–90–90 target,
i.e., to diagnose 90% of people living with HIV (PLWH) worldwide, provide ART to 90%
of PLWH, and achieve viral suppression in 90% of PLWH, by 2020 [2]. The strategy was to diagnose HIV infection
early, before PLWH could become immunocompromised, and put them on ART to achieve
sustained viral suppression, thereby halting disease progression, improving
morbidity and survival, and reducing HIV transmission [2]. By 2020, the UNAIDS estimated that 84% of PLWH worldwide
have been diagnosed, 87% have been offered ART and 90% have achieved viral
suppression [2,3]. In December 2020, the UNAIDS raised the target to be achieved by
2025 to 95–95–95, with at least 86% of all PLWH achieving viral
suppression [3].
The Korean Centers for Disease Control and Prevention has set a goal of achieving
95–95–95 by 2030, with the aim of reducing the number of new
infections in 2030 by 50% compared to 2023 [4]. In this review, I summarize the epidemiology of HIV/AIDS and the use of
ART in Korea [5].
Methods
Ethics statement
As this is a literature review study, it does not require approval from an
institutional review board or individual consent.
Study design
The present study is a narrative review of studies obtained through a web-based
database search.
Literature search and strategy
The following search terms were used in PubMed and KoreaMed.
(Korea) AND {(HIV [tiab]) OR (human immunodeficiency virus [MESH terms]) OR (ADIS
[tiab]) OR (acquired immunodeficiency syndrome [MESH terms])}.
The epidemiology of Korean HIV/AIDS
In 1985, the first HIV infection in Korea was reported in a foreigner [6]. Subsequently, the number of new infections
has gradually increased every year, and since 1995, more than 100 cases have been
reported annually. Since 1999, the number of new infections has increased rapidly
every year, and since 2003, more than 500 new infections have been registered each
year. Since 2007, the upward trend has slowed, with 700–800 new infections
are still recorded each year [7]. In 2011, the
upward trend resumed, with more than 1,000 new infections registered yearly since
2013 [8]. After peaking at 1,223 in 2019, the
number of new infections decreased from 2020 to 2022 because of the coronavirus
disease 2019 (COVID-19) pandemic, with approximately 1,000 new infections registered
annually [9]. In 2023, there were 1,005 new
HIV infections, a decrease of 61 (5.7%) compared to 2022. However, a recent study
comparing HIV infection to diagnosis before and after the COVID-19 pandemic
suggested that the actual incidence of HIV infection may have decreased more than
the possibility that HIV diagnosis was delayed due to the COVID-19 pandemic because
the median time from HIV infection to diagnosis decreased from 5.68 years before to
5.41 years after the COVID-19 pandemic [10].
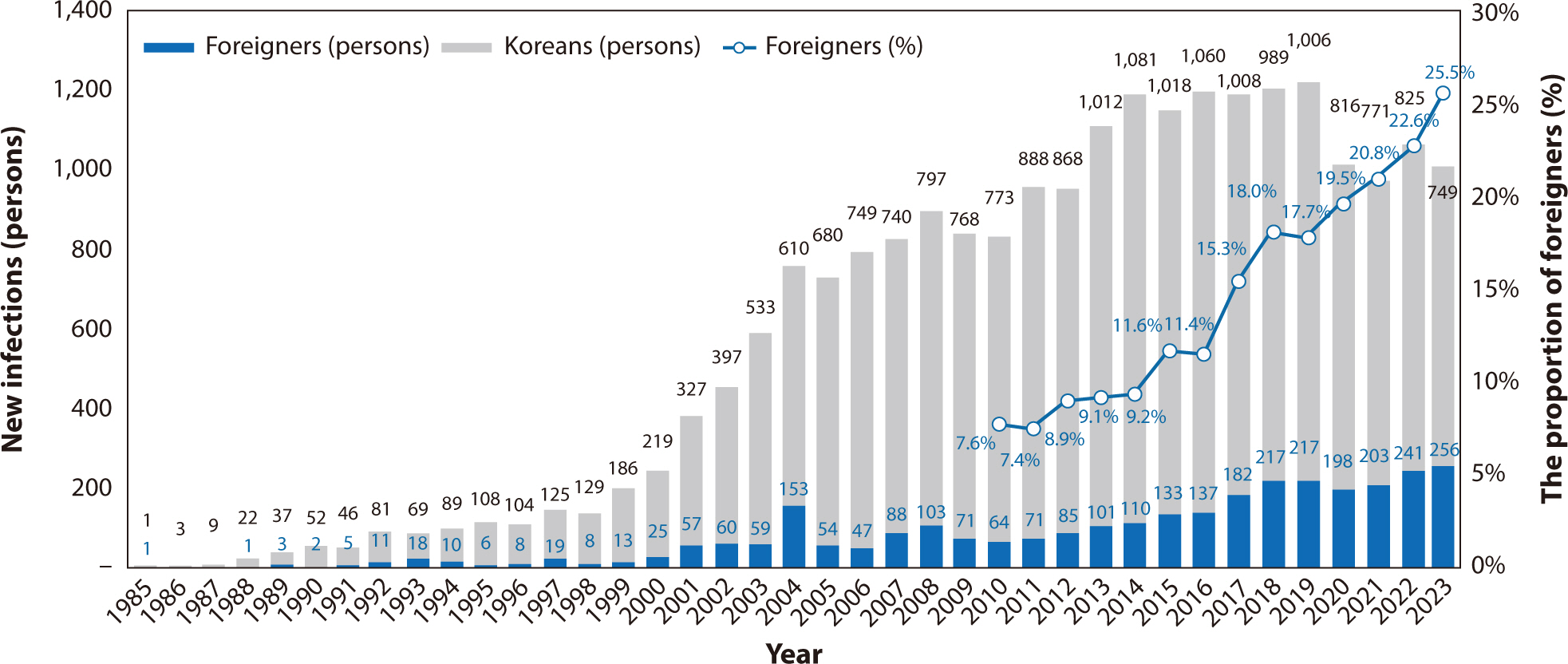
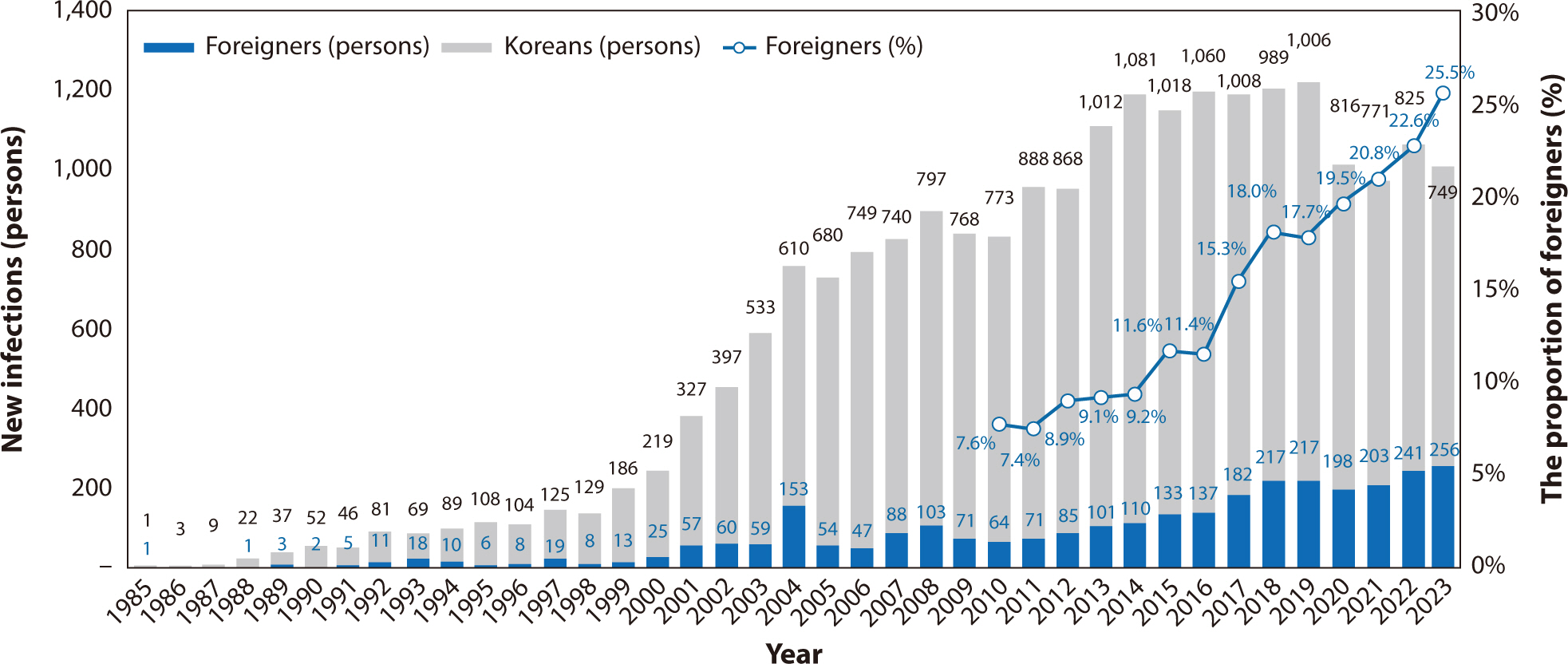
Over the past decade, there has been an average of 1,100 new cases per year, with
1,191 in 2014, 1,206 in 2018 and 1,005 in 2023, with no clear upward or downward
trend (Fig. 1) [11].
Fig. 1.
New human immunodeficiency virus infections in Korea according to year.
Adapted from Korea Centers for Disease Control and Prevention [10] with CC-BY.
After the first diagnosis in 1985, 19,745 cumulative domestic infections were
registered by the end of 2023, of which 18,495 (93.7%) were in men and 1,250 (6.3%)
in women [10]. In 2023, 130 new cases of AIDS
were registered, an incidence rate of 0.254 per 100,000 HIV-infected persons. 17.4%
of all notifications were of people living with AIDS [10]. Of the total number of infections, the average number of
Koreans with HIV infection over the past 5 years was 834. The proportion of
foreigners was 9.2% in 2014, 18.0% in 2018 and 25.5% in 2023, and increased each
year [11].
The age distribution of new infections has continued to show an increase in the
proportion of young people under the age of 40, from 53.3% in 2013 to 61.8% in 2017
and 81.0% in 2023 [11]. In particular, the
proportion of young people in their 20s and 30s increased from 576 (53.3%) in 2014
to 572 (57.8%) in 2018 and 478 (63.8%) in 2023 [11,12]. In addition, 158 (15.7%)
were in their 40s, 120 (11.9%) in their 50s, 55 (5.5%) their 60s and 16 (1.6%) were
≥70 years of age, with those aged ≥40 years accounting for 34.7% of
the total [11]. In 2023 there were new
infections in 903 men (89.9%) and 102 women (10.1%), for a gender ratio of 9:1
[11]. The proportion of men was 92.4% in
2014, 91.2% in 2018, and 89.9% in 2023, and showed a slightly decreasing trend.
According to an analysis of cases in which the transmission route of HIV infection
was identified, sexual contact was the most common mode of transmission, accounting
for 99.6% of infections, of which 54.3% were infected by homosexual contact and
42.0% by heterosexual contact in 2023 [11].
The proportion of transmission by homosexual contact increased from 53.8% in 2019 to
56.2% in 2020, 64.8% in 2021, and 65.4% in 2022 [11]. Although large numbers of transfusion and blood product-related
infections were identified early in the HIV epidemic in developed countries such as
the United States and Japan, only 46 such infections were identified in Korea, among
which 13 were from transfusions performed overseas, 17 from blood products, and 16
from transfusions performed in Korea [8,11]. To reduce the rate of HIV transmission by
blood transfusion, HIV antibody testing has been performed on blood donated in Korea
since 1987. In addition, nucleic acid amplification testing has been performed on
donated blood since February 2005 to prevent missed cases during the testing period.
As a result, no case of HIV infection via blood or blood products has been reported
since 2006 [11]. Infection via vertical
transmission occurred sporadically until 2014, with a total of nine cases reported
[8].
The number of deaths among Koreans has not changed significantly, with 142 in 2014,
136 in 2018 and 158 in 2023. There were 158 deaths among PLWH in 2023, an increase
of 16 compared to the previous year [11].
However, the causes of death among PLWH have changed; AIDS-related deaths from
opportunistic infections associated with immunosuppression and AIDS-defining cancers
are declining gradually, whereas chronic diseases such as non-AIDS-defining cancers,
liver disease, and cardiovascular disease (CVD) are emerging as important causes of
death among PLWH [13]. A study of causes of
death among PLWH using National Health Service data from 2004 to 2018 showed that
although AIDS was the most frequent (59%) cause of death, chronic conditions such as
non-AIDS-defining cancers (8.2%), suicide (7.4%), CVD (4.9%), and liver disease
(2.7%) were also important causes [14].
The prevalence of non-communicable diseases among PLWH is projected to increase from
29% in 2010 to 84% in 2030 [15]. The
proportion of AIDS-related deaths among PLWH is decreasing and the proportion of
deaths from non-AIDS causes is increasing [16]. These findings underscore the importance of treating non-AIDS
complications and comorbidities in addition to HIV infection.
Non-AIDS-defining comorbidities in Korean HIV/AIDS
Non-AIDS-defining comorbidities are increasing as a result of advances in
treatment and the aging of the patient population [17–19]. In
addition to conditions directly related to HIV infection (opportunistic
infections, AIDS-specific cancers, central nervous system infections, HIV
debilitating syndromes, and co-infection with hepatitis B or C), conditions that
are increasingly frequent in patients with HIV and are of clinical concern and
need to be treated together are defined as non-AIDS-defining comorbidities.
These include CVDs, metabolic complications, kidney diseases, psychiatric
disorders, malignancies, and so on [18].
This increase in comorbidities has led to the need for comprehensive internal
medicine care for patients with HIV, not just treatment of the infection. There
is also an increased need for consultative care with other specialists.
Because PLWH are living longer, the number of older patients is steadily
increasing in Korea, and chronic diseases such as malignancies, CVD and diabetes
are becoming important issues in HIV care [20]. In a study of the incidence of chronic diseases between PLWH
and the general population using data from the National Health Insurance
Service, PLWH had higher rates of malignancies, chronic kidney disease,
osteoporosis, diabetes, hyperlipidemia and depression than the general
population [21].
PLWH have higher rates of CVD, including myocardial infarction and hypertension,
compared to people without HIV [18,22], and the mortality rate after acute
myocardial infarction or stroke has been reported to be higher in PLWH [23]. A study with claims data from the
National Health Insurance of the Korea reported that acute coronary syndrome was
confirmed in 2.0% of PLWH, which was 1.3-fold higher than in the general
population. The overall mortality rate was 7.1% [24]. In a Korean study, the incidence of CVD in PLWH was 4.11 per
1,000 person-years and CVD was more common in the elderly and in patients with
diabetes mellitus [25]. Older PLWH should
be encouraged to adopt lifestyle modifications such as regular exercise and a
balanced diet.
HIV patients with diabetes need to avoid antiretroviral drugs that can worsen
diabetes, including proteinase inhibitors (PIs), which induce insulin resistance
and decrease insulin secretion [26].
Weight gain is reportedly greater among PLWH receiving integrase strand transfer
inhibitor (INSTI)-based cART as initial therapy [27,28]. In a Korean study,
individual INSTI-based regimens were associated with weight gain at the 24-month
follow up in both the treatment-naïve and treatment-experienced groups
[20].
In a meta-analysis, bone mineral density was found to be 6.4-fold lower and the
rate of osteoporosis 3.7-fold higher in PLWH than in individuals not infected
with HIV [29]; the rate of fractures has
been reported to be 60% higher [30]. In
addition to risk factors for osteopenia and osteoporosis in the uninfected
population, the risk of osteopenia associated with HIV medications, including
PIs and tenofovir, should be considered [29,31]. In a Korean study,
middle-aged men living with HIV had lower hip bone density and higher cortical
and trabecular bone deficit rates compared to controls [32]. This finding suggests the need for a tailored strategy
for the early detection and prevention of bone deficit in middle-aged men living
with HIV.
Although kidney diseases can be caused by HIV infection itself such as HIV
nephropathy, several antiretrovirals are associated with renal insufficiency,
including tenofovir disoproxil fumarate (TDF), and boosted atazanavir [33]. The most common renal insufficiency
observed in clinical practice is associated with the use of TDF [33,34]. In a Korean cohort study of renal insufficiency in male PLWH
based on a Korean HIV/AIDS cohort of 830 patients, 32 (3.9%) cases of renal
insufficiency occurred during 9,576 person-years of follow-up [35]. Diabetes mellitus, dyslipidemia,
exposure to tenofovir or non-nucleoside reverse transcriptase inhibitors
(NNRTIs) for >1 year, and AIDS-defining illness were risk factors for
renal insufficiency.
PLWH often experience psychological stigma, which is more severe in Korea than in
developed countries [36]. This stigma is
related to symptoms of both depression and anxiety. Brief screening for
depression is recommended for all PLWH [37]. Cognitive behavioral therapy for adherence and depression
performed by clinical psychologists is effective for treating depression in PLWH
[38]. A Korean study showed that a
nurse-delivered cognitive behavioral therapy for adherence and depression was
feasible and acceptable for PLWH and could improve their depression and quality
of life [39]. HIV-associated
neurocognitive disorder screening and the identification of modifiable factors
are needed to improve patient compliance with therapy [40]. Among 194 Korean PLWH, the prevalence of
HIV-associated neurocognitive disorders was 26.3%. Asymptomatic neurocognitive
impairment and minor neurocognitive disorder accounted for 52.9% and 47.1%,
respectively, of these patients [41].
Studies on cancer survival in PLWH using data from the National Health Insurance
Service found that cancer rates were approximately 1.7-fold higher in PLWH than
in the general population, with a decreasing trend in AIDS-related cancers and a
gradual increase in non-AIDS-related cancers [42–44]. The incidence
rates of HPV-related cancers, including cervical, anal, and oral cancers, were
4.98-, 104.2- and 2.97-fold higher, respectively, than in the general
population, and have increased recently [43–45]. Compared with
the general population, the incidence rates of lung and liver cancer were
higher, whereas that of stomach cancer tended to be lower, among PLWH [42–44]. These findings highlight the need for multifaceted cancer
prevention and early detection, including increased cancer screening, HPV
vaccination, and smoking cessation.
Antiretroviral therapy for HIV/AIDS in Korea
Zidovudine was the first treatment for HIV infection to be approved by the US
Food and Drug Administration (FDA), in 1987 [46]. Several agents were subsequently developed, and by the late
1990s it was recognized that long-term suppression of HIV was possible through a
combination of three drugs [47]. This
highly active ART is now the standard of care for HIV infection. To date, more
than 30 antiretrovirals have been approved by the US FDA: abacavir,
embricitabine, lamivudine, and tenofovir alafenamide, and TDF; the nucleoside
reverse transcriptase inhibitor (NRTI) class, which includes doravirine,
efarirenz, etravirine, nevirapine, and rilpivirine; the NNRTI class, which
includes atazanavir, darunavir, and lopinavir/ritonavir; the PI class, which
includes atazanavir, darunavir, and lopinavir/ritonavir; the INSTI class, which
includes bictegravir, dolutegravir, elvitegravir, raltegravir, and
carbotegravir; the fusion inhibitor class, which includes enfuvirtide; the CCR5
antagonist class, which includes maraviroc; the CD4 post-attachment inhibitor
class, which includes ibalizumab; the gp120 attachment inhibitor class, which
includes fostemsavir; and the capsid inhibitor class, which includes lenacapavir
[48]. In the past, each agent had to
be administered separately, resulting in large numbers of pills to be taken
daily; however, fixed-dose combinations of multiple drugs into a single
formulation have been used more recently.
ART was introduced in Korea in 1991 with zidovudine monotherapy, followed by
NRTIs such as didanosine, lamivudine, and stavudine as two-drug combination
regimens. The introduction of PIs such as indinavir and later nelfinavir in 1997
and NNRTIs such as efavirenz in 1999 led to the development of triple therapies
[49]. Subsequently, NRTIs such as
abacavir and tenofovir; PIs such as atazanavir, lopinavir/ritonavir, and
darunavir; and NNRTIs such as etravirine and rilpivirine were introduced. The
introduction of the raltegravir as a integrase inhibitor in 2010 and its
combination with elvitegravir in 2013 paved the way for single-tablet regimens
[50]. Since then, several
single-tablet regimens have been introduced, including dolutegravir,
bictegravir, and doravirine [50].
Long-acting injectable antiretrovirals are used in other nations and will soon
be introduced in Korea as a combination of carbotegravir and rilpivirine [51].
Continuous antiretroviral treatment can reduce viral replication in the blood to
below the detectable level, leading to long-term suppression of HIV. A study of
141 PLWH in Korea who had received antiretroviral treatment for at least 1 year
by 2005 found that 6 months after starting treatment, 73% of patients had
suppressed viral replication to ≤400 copies/mL [52]. Antiretroviral treatment can fail due to patient
non-adherence to the regimen, and HIV develops resistance-associated mutations.
The incidence of resistance mutations in Korea is low, but increasing, and
therefore requires attention [53]. Among
248 Korean PLWH, the rate of NNRTI resistance decreased between January 2010 and
December 2020 (by 15.3% during 2012–2014, 8.7% during 2015–2017,
and 2.4% during 2018–2020), whereas the rates of resistance to PIs and
INSTIs increased from 0% until 2018 to 3.5% and 8.2% during 2018–2020,
respectively [54]. Therefore, continuous
monitoring of the pattern of ART resistance is necessary.
Conclusion
The availability of cART has significantly reduced the prevalence and mortality of
HIV infection, which has become a chronic disease with long-term survival. Achieving
the 95–95–95 target among those living with HIV in Korea requires
multifaceted efforts to improve early diagnosis, early and proper treatment of HIV
infection including the management of chronic diseases, and adherence to ART.
Authors' contributions
All work was done by Nam Su Ku.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
2. Joint United Nations Programme on HIV/AIDS. 90-90-90: an ambitious treatment target to help end the AIDS epidemic
[Internet]. Geneva (CH): Joint United Nations Programme on HIV/AIDS; c2024 [cited 2024 Jan 13]. Available from: https://www.unaids.org/en/resources/909090
3. Frescura L, Godfrey-Faussett P, Ali Feizzadeh A, El-Sadr W, Syarif O, Ghys PD, et al. Achieving the 95 95 95 targets for all: a pathway to ending
AIDS. PLoS One 2022;17(8):e0272405.
4. Korea Centers for Disease Control and
Prevention. 2nd Strategies for the preventive management of HIV/AIDS
(2024-2028). Cheongju: Korea Centers for Disease Control and
Prevention; 2024.
5. Youn BB, Kang HC, Oh YW, Lee CH. A case report of an acquired immunodeficiency syndrome with
multiple problems, such as fever, dyspnea, abdominal pain, oral candidiasis
candida albicans esophagitis, etc. N Med J 1985;28:63-72.
6. Korea Centers for Disease Control and
Prevention. Annual report on the notified HIV/AIDS in Korea, 2010. Cheongju: Korea Centers for Disease Control and
Prevention; 2011.
7. Korea Centers for Disease Control and
Prevention. Annual report on the notified HIV/AIDS in Korea, 2022. Cheongju: Korea Centers for Disease Control and
Prevention; 2023.
8. Kim JM, Kim NJ, Choi JY, Chin BS. History of acquired immune deficiency syndrome in
Korea. Infect Chemother 2020;52(2):234-244.
9. Kim GS, Kim L, Baek S, Shim MS, Lee S, Kim JM, et al. Three cycles of mobile app design to improve HIV self-management:
a development and evaluation study. Digit Health 2024;10:20552076241249294
10. Korea Centers for Disease Control and
Prevention. Annual report on the notified HIV/AIDS in Korea, 2023. Cheongju: Korea Centers for Disease Control and
Prevention; 2024.
11. Ann HW, Jun S, Shin NY, Han S, Ahn JY, Ahn MY, et al. Characteristics of resting-state functional connectivity in
HIV-associated neurocognitive disorder. PLoS One 2016;11(4):e0153493.
12. Yoo M, Seong J, Yoon JG, Cha J, Chung YS, Kim K, et al. Characteristics of adolescents and young adults with HIV in the
Republic of Korea from 2010 through 2015. Sci Rep 2020;10(1):9384
13. Lewden C, Salmon D, Morlat P, Bévilacqua S, Jougla E, Bonnet F, et al. Causes of death among human immunodeficiency virus (HIV)-infected
adults in the era of potent antiretroviral therapy: emerging role of
hepatitis and cancers, persistent role of AIDS. Int J Epidemiol 2005;34(1):121-130.
14. Park B, Choi Y, Kim JH, Seong H, Kim YJ, Lee M, et al. Mortality and causes of death among individuals diagnosed with
human immunodeficiency virus in Korea, 2004–2018: an analysis of a
nationwide population-based claims database. Int J Environ Res Public Health 2022;19(18):11788
15. Smit M, Brinkman K, Geerlings S, Smit C, Thyagarajan K, Sighem A, et al. Future challenges for clinical care of an ageing population
infected with HIV: a modelling study. Lancet Infect Dis 2015;15(7):810-818.
16. Smith CJ, Ryom L, Weber R, Morlat P, Pradier C, Reiss P, et al. Trends in underlying causes of death in people with HIV from 1999
to 2011 (D:A:D): a multicohort collaboration. Lancet;2014;384(9939):241-248.
17. Wong C, Gange SJ, Moore RD, Justice AC, Buchacz K, Abraham AG, et al. Multimorbidity among persons living with human immunodeficiency
virus in the United States. Clin Infect Dis 2018;66(8):1230-1238.
18. Guaraldi G, Orlando G, Zona S, Menozzi M, Carli F, Garlassi E, et al. Premature age-related comorbidities among HIV-infected persons
compared with the general population. Clin Infect Dis 2011;53(11):1120-1126.
19. Hsu DC, Sereti I. Serious non-AIDS events: therapeutic targets of immune activation
and chronic inflammation in HIV infection. Drugs 2016;76(5):533-549.
20. Kim J, Nam HJ, Jung YJ, Lee HJ, Kim SE, Kang SJ, et al. Weight gain and lipid profile changes in Koreans with human
immunodeficiency virus undergoing integrase strand transfer inhibitor-based
regimens. Infect Chemother 2022;54(3):419-432.
21. Kim JH, Noh J, Kim W, Seong H, Kim JH, Lee WJ, et al. Trends of age-related non-communicable diseases in people living
with HIV and comparison with uninfected controls: a nationwide
population-based study in South Korea. HIV Med 2021;22(9):824-833.
22. High KP, Effros RB, Fletcher CV, Gebo K, Halter JB, Hazzard WR FM, et al. Workshop on HIV infection and aging: what is known and future
research directions. Clin Infect Dis 2008;47(4):542-553.
23. Okeke NL, Hicks CB, McKellar MS, Fowler VG Jr, Federspiel JJ. History of AIDS in HIV-infected patients is associated with
higher in-hospital mortality following admission for acute myocardial
infarction and stroke. J Infect Dis 2016;213(12):1955-1961.
24. Jung H, Lee E, Ro J, Lee JY, Bang J. Mortality after acute coronary syndrome in human immunodeficiency
virus infection with optimal adherence: a nationwide study. Infect Chemother 2023;55(4):471-478.
25. Bae JY, Kim SM, Choi Y, Choi JY, Kim SI, Kim SW, et al. Comparison of three cardiovascular risk scores among HIV-infected
patients in Korea: the Korea HIV/AIDS cohort study. Infect Chemother 2022;54(3):409-418.
27. Sax PE, Erlandson KM, Lake JE, McComsey GA, Orkin C, Esser S, et al. Weight gain following initiation of antiretroviral therapy: risk
factors in randomized comparative clinical trials. Clin Infect Dis 2020;71(6):1379-1389.
28. Norwood J, Turner M, Bofill C, Rebeiro P, Shepherd B, Bebawy S, et al. Brief report: weight gain in persons with HIV switched from
efavirenz-based to integrase strand transfer inhibitor-based
regimens. J Acquir Immune Defic Syndr 2017;76(5):527-531.
30. Triant VA, Brown TT, Lee H, Grinspoon SK. Fracture prevalence among human immunodeficiency virus
(HIV)-infected versus non-HIV-infected patients in a large U.S. healthcare
system. J Clin Endocrinol Metab 2008;93(9):3499-3504.
31. Bonjoch A, Figueras M, Estany C, Perez-Alvarez N, Rosales J, del Rio L, et al. High prevalence of and progression to low bone mineral density in
HIV-infected patients: a longitudinal cohort study. AIDS 2010;24(18):2827-2833.
32. Hong N, Kim JH, Treece G, Kim HC, Choi JY, Rhee Y. Cortical and trabecular bone deficit in middle‐aged men
living with HIV. J Bone Miner Res 2023;38(9):1288-1295.
33. Lucas GM, Ross MJ, Stock PG, Shlipak MG, Wyatt CM, Gupta SK, et al. Clinical practice guideline for the management of chronic kidney
disease in patients infected with HIV: 2014 update by the HIV Medicine
Association of the Infectious Diseases Society of America. Clin Infect Dis 2014;59(9):e96-e138.
34. Islam FM, Wu J, Jansson J, Wilson DP. Relative risk of renal disease among people living with HIV: a
systematic review and meta-analysis. BMC Public Health 2012;12:234
35. Kim JH, Jang H, Kim JH, Song JY, Kim SW, Kim SI, et al. The incidence and risk factors of renal insufficiency among
Korean HIV infected patients: the Korea HIV/AIDS cohort
study. Infect Chemother 2022;54(3):534-541.
36. Kim K, Jang S, Rim HD, Kim SW, Chang H, Woo J. Attachment insecurity and stigma as predictors of depression and
anxiety in people living with HIV. Psychiatry Investig 2023;20(5):418-429.
38. Safren SA, O'Cleirigh CM, Bullis JR, Otto MW, Stein MD, Pollack MH. Cognitive behavioral therapy for adherence and depression
(CBT-AD) in HIV-infected injection drug users: a randomized controlled
trial. J Consult Clin Psychol 2012;80(3):404-415.
39. Kim JH, Kim JM, Ye M, Lee JI, Na S, Lee Y, et al. Implementation of a nurse-delivered cognitive behavioral therapy
for adherence and depression of people living with HIV in
Korea. Infect Chemother 2022;54:733-743.
40. Zipursky AR, Gogolishvili D, Rueda S, Brunetta J, Carvalhal A, McCombe JA, et al. Evaluation of brief screening tools for neurocognitive impairment
in HIV/AIDS: a systematic review of the literature. AIDS 2013;27(15):2385-2401.
41. Ku NS, Lee Y, Ahn JY, Song JE, Kim MH, Kim SB, et al. HIV-associated neurocognitive disorder in HIV-infected Koreans:
the Korean NeuroAIDS project. HIV Med 2014;15(8):470-477.
42. Lee SO, Lee JE, Lee S, Lee SH, Kang JS, Son H, et al. Nationwide population-based incidence of cancer among patients
with HIV/AIDS in South Korea. Sci Rep 2022;12(1):9974
43. Park B, Ahn KH, Choi Y, Kim JH, Seong H, Kim YJ, et al. Cancer incidence among adults with HIV in a population-based
cohort in Korea. JAMA Netw Open 2022;5(8):e2224897.
44. Lee SO, Lee JE, Sim YK, Lee S, Ko WS, Kim J, et al. Changing trends in the incidence and spectrum of cancers between
1990 and 2021 among HIV-infected patients in Busan, Korea. J Infect Chemother 2023;29(6):571-575.
45. Lee CH, Lee SH, Lee S, Cho H, Kim KH, Lee JE, et al. Anal human papillomavirus infection among HIV-infected men in
Korea. PLoS One 2016;11(8):e0161460.
46. Fischl MA, Richman DD, Grieco MH, Gottlieb MS, Volberding PA, Laskin OL, et al. The efficacy of azidothymidine (AZT) in the treatment of patients
with AIDS and AIDS-related complex. N Engl J Med 1987;317(4):185-191.
47. Hammer SM, Squires KE, Hughes MD, Grimes JM, Demeter LM, Currier JS, et al. A controlled trial of two nucleoside analogues plus indinavir in
persons with human immunodeficiency virus infection and CD4 cell counts of
200 per cubic millimeter or less. N Engl J Med 1997;337(11):725-733.
49. Lee SH, Kim KH, Lee SG, Chen DH, Jung DS, Moon CS, et al. Trends of mortality and cause of death among HIV-infected
patients in Korea, 1990-2011. J Korean Med Sci 2013;28(1):67-73.
50. Shin YH, Park CM, Yoon CH. An overview of human immunodeficiency virus-1 antiretroviral
drugs: general principles and current status. Infect Chemother 2021;53(1):29-45.
51. Swindells S, Andrade-Villanueva JF, Richmond GJ, Rizzardini G, Baumgarten A, Masiá M, et al. Long-acting cabotegravir and rilpivirine for maintenance of HIV-1
suppression. N Engl J Med 2020;382(12):1112-1123.
52. Kim MS, Shin SY, Park YS, Kim YA, Ku NS, Kim JH, et al. Therapeutic response of HAART and analysis of related factors in
Korean HIV-infected persons. Infect Chemother 2007;39(3):142-150.
53. Kim MH, Song JE, Ahn JY, Kim YC, Oh DH, Choi H, et al. HIV antiretroviral resistance mutations among antiretroviral
treatment-naive and -experienced patients in South Korea. AIDS Res Hum Retroviruses 2013;29(12):1617-1620.
54. Oh SM, Bang J, Park SW, Lee E. Resistance trends of antiretroviral agents in people with human
immunodeficiency virus in Korea, 2012 - 2020. Infect Chemother 2023;55(3):328-336.
Progressive Multifocal Leukoencephalopathy in Patients with HIV—Case Series from Northeastern Romania Isabela Ioana Loghin, Marius Gabriel Dabija, Narcis Valentin Tănase, Șerban Alin Rusu, Ion Cecan, Victor Daniel Dorobăț, Carmen Mihaela Dorobăţ, Lucian Eva Journal of Clinical Medicine.2026; 15(3): 1232. CrossRef
Bayesian analysis of the prevalence and determinants of viral load suppression in South Africa Seyifemickael Amare Yilema, Alebachew Taye Belay, Najmeh Nakhaei Rad, Ding-Geng Chen Discover Public Health.2026;[Epub] CrossRef
İŞVERENİN BİLDİRİMSİZ FESİH HAKKI BAKIMINDAN “İŞÇİNİN HIV ENFEKSİYONUNUN” DEĞERLENDİRİLMESİ Muharrem Emre Ulusoy Hacettepe Hukuk Fakültesi Dergisi.2025; 15(2): 303. CrossRef
Unresolved policy on the new placement of 2,000 entrants at Korean
medical schools and this issue of Ewha Medical
Journal Sun Huh The Ewha Medical Journal.2024;[Epub] CrossRef
The epidemiology of HIV/AIDS and the use of antiretroviral therapy in
Korea: a narrative review
Fig. 1.
New human immunodeficiency virus infections in Korea according to year.
Adapted from Korea Centers for Disease Control and Prevention [10] with CC-BY.
Fig. 1.
The epidemiology of HIV/AIDS and the use of antiretroviral therapy in
Korea: a narrative review