
| You Won Choi | 7 Articles |
|
[English]
[English]
Nontuberculous mycobacterial infections, which are often acquired from environmental sources such as water and soil, exhibit a variety of cutaneous manifestations that frequently lead to misdiagnoses and delays in treatment. A 77-year-old woman presented with multiple skin lesions in a sporotricoid distribution on her right leg, which persisted despite standard antibiotic treatments. Based on the skin biopsy, revealing granulomatous inflammation with acid-fast bacilli, and PCR testing, a nontuberculous mycobacterial infection was diagnosed. Antimycobacterial drug combinations, including clarithromycin, isoniazid, and rifampicin for 4 months, complete the skin lesion's clearance. This case underscores the need for heightened suspicion and the use of appropriate diagnostic techniques, including tissue biopsies and molecular methods such as PCR. Citations Citations to this article as recorded by
[English]
[English]
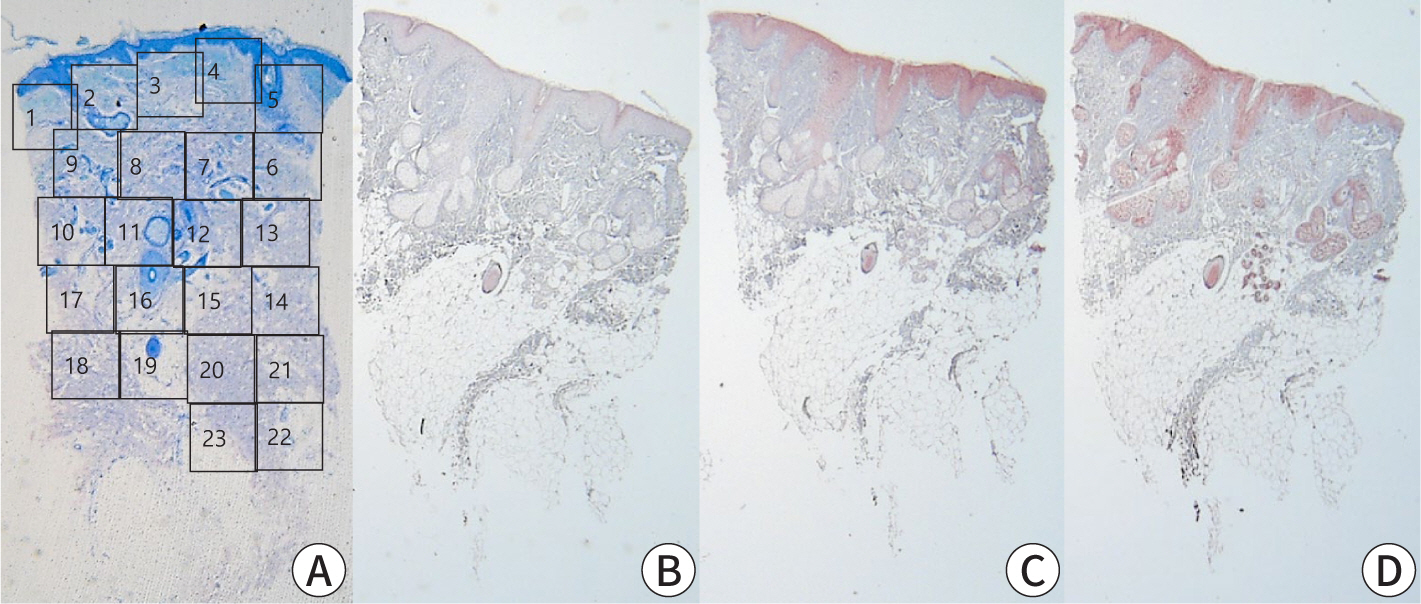
Pancreatic panniculitis is a rare skin complication in which subcutaneous fat necrosis occurs in association with pancreatic disorders, most commonly acute or chronic pancreatitis. Erythematous subcutaneous nodules develop on the legs and spontaneously ulcerate or exude an oily substance. A 32-year-old Korean female patient presented with a 2-week-history of tender nodules with erythematous crusts on her left shin. She had a history of alcoholic liver cirrhosis and, 5 weeks earlier, had been diagnosed with acute pancreatitis. The histopathologic findings from a skin biopsy were consistent with lobular panniculitis, without signs of vasculitis, and diffuse fat necrosis. Basophilic calcium deposits were present in the dermis and subcutaneous fat. These findings were suggestive of pancreatic panniculitis. The skin lesion had a chronic course corresponding to repeated exacerbations of the patient’s pancreatitis. Thus, in the differential diagnosis of subcutaneous nodules, clinicians should consider pancreatic panniculitis as a cutaneous manifestation of pancreatic disease. Citations Citations to this article as recorded by
[English]
[English]
Drug eruptions are common problems in hospital inpatients and outpatients. Cutaneous drug reactions range from mild to severe and from those localized only to skin to those associated with systemic disease. Cutaneous drug reactions are also a challenging diagnostic problem since they can mimic a large variety of skin diseases, including viral exanthem, collagen vascular disease, neoplasia, bacterial infection, psoriasis, and autoimmune blistering disease, among others. Furthermore, determining a particular medication which caused an eruption is often difficult when the patient is taking multiple drugs. In this review, clinical manifestations of adverse cutaneous drug reactions are described. A morphologic approach to drug eruption includes those that are classified as exanthematous eruption, urticaria, pustular eruption, bullous eruption, fixed drug eruption, photosensitive eruption, skin necrosis, lichenoid eruption, cutaneous pseudolymphoma, lupus erythematosus, and hand-foot syndrome. And also, recently reported cutaneous adverse reactions associated with newly developed drugs, such as epidermal growth factor receptor inhibitors, low molecular weight tyrosine kinase inhibitors, tumor necrosis factor-alpha antagonists, sirolimus and granulocyte colony-stimulating factor, are discussed. Citations Citations to this article as recorded by
[English]
Urticaria is multifactorial disease. Type 1 hypersensitivity reaction plays an important role in developing or aggravating the disease, so determining of the causative allergens and avoiding them from patient's environment are helpful in treating the disease. The purpose of this study is to estimate the positive rate of each allergens in urticaria patients and to assess the differences by sex, age, year, residence type and the duration of the disease. We retrospectively reviewed the medical records of 304 patients with urticaria who underwent skin prick test and 707 patients with urticaria who underwent serum allergen test at the department of dermatology in Mok-Dong Hospital, Ewha Womans University for 10 years from March 1998 to April 2008. In skin prick test, the positive rates of major allergen were D.farinae 52.0%, D.pteronyssinus 47.7%, cockroach mix 27.3%, weeds 15.8%, shellfish 15.1% in that order. D.farinae, D.pteronyssinus and cockroach mix had the highest positive rates in acute and chronic urticaria, but the rates in acute urticaria were much lower than those in chronic urticaria. In serum allergen test, the positive rates of major allergen were D.farinae 31.8%, D.pteronyssinus 24.5%, housedust 24.0%, acarus siro 11.0%, cat fur 9.3%. D.farinae and D.pteronyssinus showed the highest positive rates in 20s and cockroach mix in 40s. Some allergens had statistically significant differences of positive rates by each parameter. Therefore identifying and analysing allergen trends would play an important role in deprivation therapy in urticaria patients.
|
|
 , Yoon Jin Choi
, Yoon Jin Choi