1Department of Colon and Rectal Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
*Corresponding author: Chan Wook Kim,
Department of Colon and Rectal Surgery, Asan Medical Center, University of Ulsan
College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea, Tel:
82-2-3010-3928, Fax: 82-2-3010-6710, E-mail:
crscwkim@amc.seoul.kr
• Received: September 30, 2022 • Accepted: October 4, 2022
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
The rate of colorectal cancer (CRC) has altered. Early-onset CRC patients are
increasing, and it is one of the main causes of cancer-related death. Based on
epidemiologic change, the CRC screening program needs to be changed. To increase
compliance, non-invasive screening techniques are developed. Although CRC
survival has increased, the oncologic prognosis of metastatic CRC is remains
poor. Even in metastatic CRC, which is the most difficult to treat, attempts are
being made to increase the survival rate by active surgical therapy with the
creation of chemotherapeutic regimens and targeted treatment based on genomic
information. Due to the introduction of aggressive chemotherapy regimens,
targeted therapy based on genomic features, and improvements in surgical
technique, the role of surgical treatment in metastatic CRC has expanded.
Metastatic CRC surgery was indicated for liver, lung, and even peritoneal
seeding. Local ablation therapy was also effectively used for liver and lung
metastasis. Cytoreductive surgery and intraperitoneal chemotherapy were tried
for peritoneal seeding and demonstrated good results in a subgroup of patients,
although the right indication was carefully assessed. At the same time, one of
the key goals of treatment for CRC was to maintain functional outcomes.
Neoadjuvant treatment, in particular, helped rectal cancer patients preserve
functional results while maintaining oncologic safety. Rectal cancer organ
preservation techniques are now being researched heavily in a variety of
neoadjuvant treatment settings, including immunotherapy and whole neoadjuvant
therapy. Precision medicine based on patient and disease characteristics is
currently being used for the diagnosis and treatment of CRC.
In 2019, cancer is the leading cause of death in Korea, and colorectal cancer (CRC)
is one of the most prevalent malignancies worldwide [1,2]. CRC is the second leading
cause of cancer-related death and the third most prevalent malignancy globally
[2]. Thyroid, lung, stomach, colorectal,
and breast cancer were the five most frequently diagnosed malignancies in Korea in
2019 according to statistics from the National Cancer Registration Project of the
Central Cancer Registry of Korea. After stomach and lung cancer in males and breast
and thyroid cancer in women, CRC is the third most frequent malignancy in both sexes
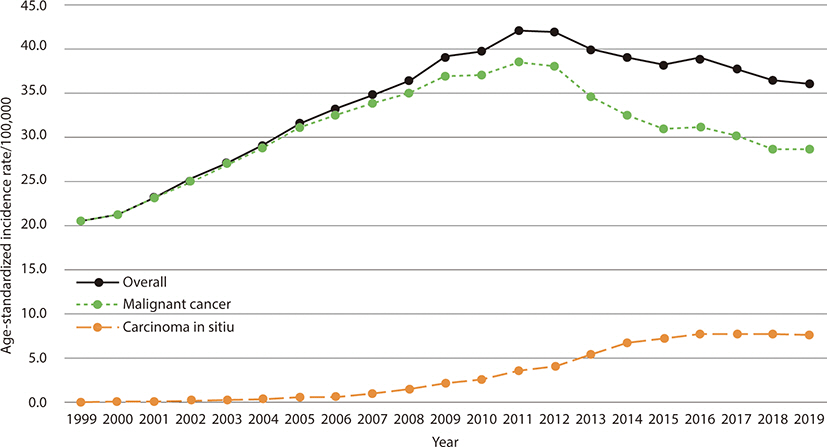
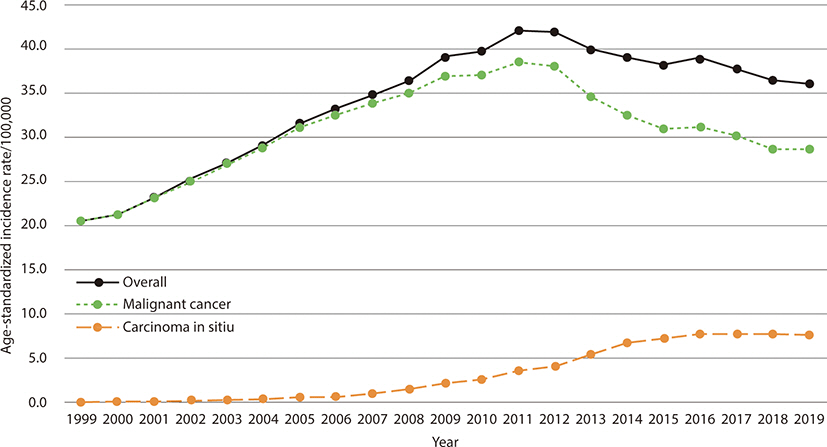
[1]. Since 1999, the incidence of CRC has
been consistently rising; however, it has been slowly declining since about 2011.
Both rectal and colon cancers exhibit the same incidence trend (Fig. 1). Although adenocarcinoma makes up the majority of CRC
cases, neuroendocrine tumors are the most common non-adenocarcinoma [3]. A feature worth observing is the lowering of
the age of onset, and it has been observed that in industrialized nations, the
prevalence of early-onset CRC in those under 50 is rising, increasing social
awareness It is very obvious that CRC incidence is rising among the elderly. The
growing older population in good health appears to be the cause. A national
investigation on the treatment strategy for advanced CRC seems necessary given the
current trend toward an aging society [1,2,4].
Fig. 1.
Age-standardized incidence rates of colorectal cancer in Korea,
1999–2019. Adapted from Kang et al. [1] with CC-BY-NC.
Overall survival (OS) rates for CRC patients in Korea are extremely high, and the
relative OS rate for CRC patients is reported to be 74.3% of patients diagnosed
between 2015 and 2019 [1]. In Korea, the OS
rate of CRC varies by gender, with men having a greater rate than women. The
increased survival rate in men is thought to be due to the average age of CRC
diagnosis being older in women than in men and the presence of more right-sided CRC
in women, despite the fact that the precise mechanism is unknown [1,2,5]. Although the survival rate for CRC in stages
I-III is increasing, there is still an issue because the increase in the OS rate for
CRC with metastatic disease is not significant.
Advances in Colorectal Cancer Screening and Diagnosis
The cost, compliance, sensitivity, and specificity of the test, as well as other
factors, are taken into account while choosing the screening test to be used. Fecal
occult blood test, an immunochemical test method, is now employed in Korea as the
first line screening test for national health screening. Although there is still
debate regarding the accuracy of the diagnosis of polyps or CRC, the non-invasive
test has the significant advantage of high compliance. There will not be any debate
on the importance of colonoscopy in the timely diagnosis and treatment of
precancerous lesions and early CRC. Due to the invasiveness and low compliance of
the colonoscopy as a primary screening test, it is crucial to weigh this option
[6,7]. Fecal occult blood testing every one to two years for asymptomatic
persons aged 45 to 80 is the current CRC screening prescription in Korea, and
colonoscopies are only occasionally conducted according on individual risk. The
question of whether colonoscopy can be used as a primary screening test is being
investigated in Korea as a pilot project, but it is still necessary to make
decisions about potential complications and costs, whether the examination can be
restricted based on bowel preparation, and how to assess the operator's
skill. In particular, the screening test may only be used and assessed for
effectiveness after extensive research and development on how to improve patient
compliance.
More accurate non-invasive screening methods have been developed in an effort to
replace the fecal occult blood test, which is the current screening method [8–10] (Table 1). The test that
seeks to identify tumor epithelial DNA in feces in order to diagnose CRC is now
coming the closest to clinical application. An assay for mutant KRAS, methylation
BMP3, methylated NDRG4, and a fecal immunochemical test for hemoglobin were all
included in the FDA-approved multi-target fecal DNA test [8]. In a research involving 9,989 average-risk people having
colonoscopy, the multi-target fecal DNA test demonstrated better sensitivity for the
diagnosis of CRC (92% vs. 74%) and advanced adenoma (42% vs. 24%) when compared with
fecal immunochemical test test. In 2018, the Ministry of Food and Drug Safety in
Korea approved the EarlyTect fecal DNA test (Genomic Tree, Daejun, Korea), which
only examines the methylation of one gene, the syndecan-2 gene [10]. The findings are significant since we are
carrying out a prospective multicenter study with a focus on the asymptomatic
general population over 60 or in the high-risk category. Due to its excellent
disease prediction, non-invasiveness, and high compliance, this fecal DNA detection
test is projected to be used as a screening tool. The poor identification rate of
pre-cancerous lesions is a challenge; thus it is important to watch with greater
skepticism what kind of outcomes will be seen in the long-term impact of CRC
prevention in the future.
Table 1.
Clinically available non-invasive screening method with stool DNA
detection for colorectal cancer diagnosis
NDRG4, N-myc downstream-regulated gene 4;
BMP3, bone morphogenetic protein 3;
KRAS, Kirsten rat sarcoma virus;
SDT2, synthecan 2.
Changes to CRC screening are required in light of the rising incidence of CRC in
people under the age of 50 [1,2,11] and
the growing elderly population. Although the US Preventive Services Task Force and
the Multi-Specialty Task Force currently recommend starting screening at age 50, the
American Cancer Society published guidelines in 2018 with a qualified recommendation
to lower the starting age for CRC screening from 50 to 45 years of age in the
average-risk adult population [12]. Few
empirical studies have been conducted on the effectiveness of screening in younger,
average-risk persons [13,14], and it is unknown which screening method
is best for this age group.
According to the US Preventive Services Task Force's most recent CRC screening
recommendation for individuals aged 76 to 85, the choice to test for CRC should be
made individually, taking into account the patient's general health and
screening history [15]. According to the
recommendation, screening is best recommended for people who have never been
screened, are healthy enough to get treatment if CRC is found, and do not have
significantly shortened life expectancies. Due to conflicting sources of death,
screening is not advised for persons 86 years of age and older. Although further
research is needed, healthcare professionals should participate in shared
decision-making when evaluating people over 75 years old and take into account
factors like life expectancy, patient risk, values, and preferences. It is crucial
to advise when to halt screening in future research.
Development Surgical Treatment of Metastatic Colorectal Cancer
Despite a significant improvement in treatment outcomes for CRC, metastatic CRC
therapy outcomes remain remarkably poor [1,2]. Therefore, we have worked
hard to actively treat patients with metastatic disease in an effort to increase the
OS of CRC patients.
Chemotherapy is the major treatment for CRC that has spread to other organs, and
surgery is only occasionally employed. However, with advancements in systemic
therapy, increased use of genetic information, and the development of surgical
techniques, more individuals with metastatic CRC can benefit from curative-intent
surgical surgery [16–18].
Liver metastasis, common metastasis of CRC, is known as metastatic CRC that can
improve the prognosis with surgery. Liver resection with or without local ablation
therapy, such as radiofrequency ablation and stereotatic radiation (SBRT), can be
used for curative treatment in CRC patients with liver metastases [19–21]. Numerous prognostic factors and key drivers of resectability have
included the size and location of liver metastases, as well as their distribution
throughout the liver and the existence of extrahepatic metastatic lesions [20,22,23]. However, today, even in
situations with multiple liver metastases, surgery is used when the likelihood of
resection is verified through earlier chemotherapy, and in some instances, secondary
resection is carried out in specific patients [23–25]. In metastatic CRC
patients with bi-lobar liver metastases and limited functional liver remnants,
portal vein embolization can be used with CRC surgery to assure tumor regression and
hepatic hypertrophy (FLR). The two-stage hepatectomy would also enable the total
removal of bi-lobar liver metastases and FLR regulation. To get around the drawback
of liver resection in CRC patients with a small FLR and numerous liver metastases,
associating liver partition and portal vein ligation for phased hepatectomy (ALPPS)
was created. According to reports, there was no discernible difference between ALPPS
and two-stage hepatectomy in terms of postoperative morbidities and fatalities,
although ALPPS had improved survival outcomes in randomized controlled trials [25,26].
Different strategies would be taken into consideration for individuals with
synchronous liver metastases depending on their general health, the likelihood of
curative resection, and extra-hepatic metastasis. There have been recommendations
for simultaneous resection, liver-first strategy, and bowel first approach. Although
a simultaneous liver and colon resection has advantages over a
liver-first/bowel-first approach in terms of avoiding two surgeries, expediting the
start of chemotherapy, and lowering the risk of cancer dissemination, postoperative
complications and increased surgical stress are still a concern [27–29].
Surgical treatment for lung metastases and peritoneal metastases is developing in
addition to liver metastases. Surgery can be beneficial for pulmonary metastasis, a
metastatic lesion that is similar to liver metastasis in terms of how well it
responds to treatment [30,31]. A five-year OS rate of more than 50% was
observed after pulmonary metastasectomy in a systematic analysis of surgical removal
of pulmonary metastases in CRC patients [31].
Now, pulmonary oligo-metastasis and solitary lesions are frequently treated with
video-assisted thoracoscopic surgery. In a recent meta-analysis, there was no
discernible difference in the rates of OS and recurrence-free survival between open
thoracotomy and video-assisted thoracoscopic surgery for pulmonary metastasectomy
[32]. Additionally, SBRT is beginning to
show promise in the management of lung metastases. The examination of a sizable
multi-center database revealed that OS was enhanced by SBRT for oligo-metastatic
CRC. Retrospective analysis of 381 oligo-metastatic CRC lesions in 235 CRC patients
revealed that those who underwent SBRT had two-year OS rates of 76.1% and five-year
OS rates of 35.9% [21,33]. The advancement of non-surgical local therapy benefits the
active management of lung metastases as well.
It is known that peritoneal metastasis occurs in about 5%–15% of CRC patients,
and the metastasis of CRC is known to have the worst prognosis [16]. Surgery has a very small part in the
management of peritoneal metastases; the primary therapy is palliative chemotherapy.
However, the role of surgery has been consistently examined in patients with limited
peritoneal metastases, and efforts to increase the survival rate have persisted
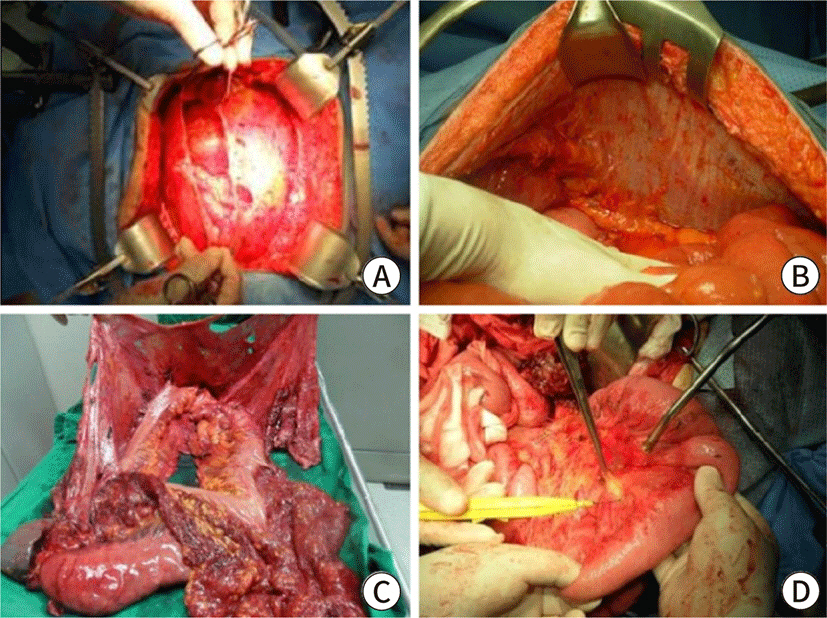
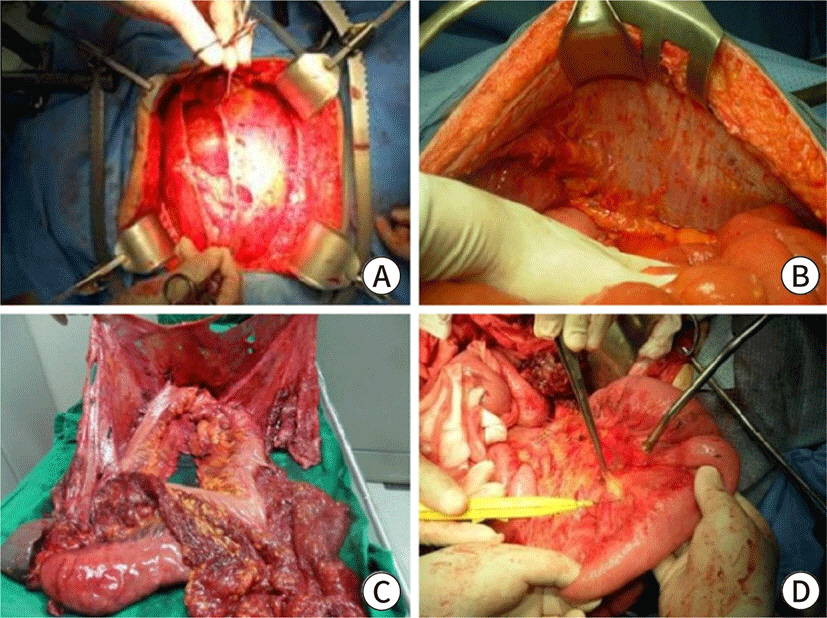
through active treatment with cytoreductive surgery (CRS) and hyperthermic
intraperitoneal chemotherapy (HIPEC) [16,34–36] (Fig.
2). In some patients with peritoneal metastases, CRS/HIPEC may enhance
oncological outcomes, according to long-term randomized controlled trials and
meta-analyses [35,36]. Effectiveness of HIPEC has been questioned, though, with
the advent of systemic chemotherapy [37], and
it is thought that this is due to resistance to the anticancer medications that are
currently being employed. As a result, progress in treating metastatic CRC,
particularly in raising the survival rate, has stalled. Instead, doctors are still
choosing anticancer drugs that are sensitive to the disease and using precision
medicine when it is necessary. It appears to be a solution for the treatment of
peritoneal metastasis [38]. In order to
effectively treat metastatic CRC in the future, new medications will need to be
created and used, with treatment decisions based on more precise genetic data. In
addition, the role of sophisticated multidisciplinary treatment involving
professionals will be critical for improving oncological outcomes in order to
increase the potential of curing as well as controlling the disease by performing
surgical treatment and other local treatments at the right moment.
Fig. 2.
Cytoreductive surgery for patients with peritoneal carcinomatosis from
colorectal cancer. Peritoectomy process at (A) pelvic cavity, (B) left upper
quadrant, (C) intestinal organs, (D) and small bowel mesentery. Adapted from
Kim and Kim 2021 [16] with
CC-BY-NC.
Paradigm Shift of Rectal Cancer Treatment
Neoadjuvant chemoradiotherapy (nCRT) altered the idea of surgical excision in the
treatment of rectal cancer. Surgery has always been and continues to be regarded as
the most crucial and necessary step for cure of CRC [39]. Although it is known that there is no change in the OS or
recurrence-free survival rates when compared to postoperative radiation therapy or
surgical resection alone, radiation therapy prior to rectal cancer surgery boosts
the full resection rate of rectal cancer and lowers the local recurrence rate [40]. Despite this drawback, finding total or
nearly complete rectal cancer regression to nCRT allowed even individuals with
early-stage advanced rectal cancer to use an organ-preserving method. Although
radical resection of rectal cancer has improved functional outcomes and greater
sphincter preservation due to technical advancements [41,42], organ
preservation strategies have grown in popularity due to its obvious functional
benefits when compared to oncologic outcomes [43–45]. When the results
of representative trials, which showed good oncologic outcomes following organ
preservation [44,45], were compared to the outcomes of radical resection for
patients who respond well to nCRT, interest in organ preservation of rectal cancer
has sharply increased. Many initiatives have been made in an effort to increase the
number of patients who fully respond to nCRT. The greatest barrier to incorporating
organ preservation techniques into actual clinical practice, meanwhile, continues to
be the poor accuracy of response evaluation to nCRT. It also has to do with the
diagnosis of local regrowth, a rare variation of local recurrence in rectal cancer
treated with organ preservation techniques. However, the salvage percentage for
these patients was observed to vary [46,47]. Local regrowth occurred in 20%–30%
of patients who undergo organ preservation [44–46]. In this context,
we must be careful not to reduce the likelihood of a cure by improperly implementing
an organ preservation strategy.
In the era of advanced rectal cancer treatment, trials to enhance distant metastasis
control are ongoing, along with enhancing quality of life by including comprehensive
neoadjuvant treatment (TNT) [48,49]. TNT, however, has not yet demonstrated any
advantages in terms of controlling distant metastases, although showing a rise in
clinical near-complete responders. After nCRT, distant metastasis is still a
significant oncologic issue, therefore we need to wait and critically examine
long-term results [50]. The emphasis on
striking a balance between quality of life and oncologic outcomes for the treatment
of rectal cancer will continue.
Conclusion
A significant cancer subtype that continues to endanger public health is CRC.
Although the screening program is now run well, there is ongoing concern about how
to increase compliance and practically apply non-invasive tests. The screening
program must be revised to reflect epidemiologic shift as the prevalence of
young-age CRC grew and, on the other hand, elderly CRC patients increased due to an
increase in life expectancy. Physicians and patients are more interested in finding
ways to balance quality of life and oncologic outcomes, and surveillance is more
crucial to find cancer as early as feasible in order to preserve function without
impairing oncologic results.
Active treatment for metastatic CRC has been carried out to break the CRC survival
plateau. The role of surgical treatment has increased for metastatic CRC along with
systemic treatment and targeted treatment based on genomic features of individuals.
On the other hand, one of the most significant changes in the period of surgical
therapy of CRC is the judicious deferral of surgical treatment, including
nCRT/TNT.
The overall trend in CRC treatment is toward precision medicine, which protects the
patient's quality of life while also ensuring the best oncological treatment
outcomes by taking into account the patient's unique traits, way of life, and
genetic characteristics. As a result, the trend in treatment showed development at
both ends: for rectal cancer, which responds well to neoadjuvant therapy, efforts
are rising in the direction of organ preservation, and for metastatic CRC, which had
previously undergone rather harsh treatment. It will be able to offer a new
development direction for CRC treatment when the financial support to move from the
current standard, which concentrated on standard treatment to enhance the overall
treatment outcome, to precision treatment and the improvement of the system come
together.
Acknowledgements
Not applicable.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Author Contribution
The article is prepared by a single author.
Ethics Approval and Consent to Participate
Not applicable.
References
1. Kang MJ, Won YJ, Lee JJ, Jung KW, Kim HJ, Kong HJ, et al. Cancer statistics in Korea: incidence, mortality, survival, and
prevalence in 2019. Cancer Res Treat 2022;54(2):330-344.
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence
and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71(3):209-249.
3. Nam S, Kim D, Jung K, Choi YJ, Kang JG. Analysis of the incidence and clinical features of colorectal
nonadenocarcinoma in Korea: a national cancer registry-based
study. Ann Coloproctol 2020;36(6):390-397.
4. Lee SM, Shin JS. Colorectal cancer in octogenarian and nonagenarian patients:
clinicopathological features and survivals. Ann Coloproctol 2020;36(5):323-329.
5. Siegel RL, Miller KD, Sauer AG, Fedewa SA, Butterly LF, Anderson JC, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin 2020;70(3):145-164.
6. Shaukat A, Kahi CJ, Burke CA, Rabeneck L, Sauer BG, Rex DK. ACG clinical guidelines: colorectal cancer screening
2021. Am J Gastroenterol 2021;116(3):458-479.
7. Sohn DK, Kim MJ, Park Y, Suh M, Shin A, Lee HY, et al. The Korean guideline for colorectal cancer
screening. J Korean Med Assoc 2015;58(5):420-432.
8. Imperiale TF, Ransohoff DF, Itzkowitz SH, Turnbull BA, Ross ME. Fecal DNA versus fecal occult blood for colorectal-cancer
screening in an average-risk population. N Engl J Med 2004;351(26):2704-2714.
9. Alhadi SC, Zain WZW, Zahari Z, Hashim MNM, Aziz SHSA, Zakaria Z, et al. The use of M2-pyruvate kinase as a stool biomarker for detection
of colorectal cancer in tertiary teaching hospital: a comparative
study. Ann Coloproctol 2020;36(6):409-414.
10. Han YD, Oh TJ, Chung TH, Jang HW, Kim YN, An S, et al. Early detection of colorectal cancer based on presence of
methylated syndecan-2 (SDC2) in stool DNA. Clin Epigenetics 2019;11(1):51
11. Meester RGS, Peterse EFP, Knudsen AB, de Weerdt AC, Chen JC, Lietz AP, et al. Optimizing colorectal cancer screening by race and sex:
microsimulation analysis II to inform the American Cancer Society colorectal
cancer screening guideline. Cancer 2018;124(14):2974-2985.
12. Liang PS, Allison J, Ladabaum U, Martinez ME, Murphy CC, Schoen RE, et al. Potential intended and unintended consequences of recommending
initiation of colorectal cancer screening at age 45 years. Gastroenterology 2018;155(4):950-954.
13. Mannucci A, Zuppardo RA, Rosati R, Leo MD, Perea J, Cavestro GM. Colorectal cancer screening from 45 years of age: thesis,
antithesis and synthesis. World J Gastroenterol 2019;25(21):2565-2580.
14. Imperiale TF, Kahi CJ, Rex DK. Lowering the starting age for colorectal cancer screening to 45
years: who will come… and should they? Clin Gastroenterol Hepatol 2018;16(10):1541-1544.
15. US Preventive Services Task Force. Screening for colorectal cancer US preventive services task force
recommendation statement. J Am Med Assoc 2021;325(19):1965-1977.
18. Torky R, Alessa M, Kim HS, Sakr A, Zakarneh E, Sauri F, et al. Characteristics of patients presented with metastases during or
after completion of chemoradiation therapy for locally advanced rectal
cancer: a case series. Ann Coloproctol 2021;37(3):186-191.
19. Ruers T, Punt C, Van Coevorden F, Pierie JPEN, Borel-Rinkes I, Ledermann JA, et al. Radiofrequency ablation combined with systemic treatment versus
systemic treatment alone in patients with non-resectable colorectal liver
metastases: a randomized EORTC Intergroup phase II study (EORTC
40004). Ann Oncol 2012;23(10):2619-2626.
21. Sheikh S, Chen H, Sahgal A, Poon I, Erler D, Badellino S, et al. An analysis of a large multi-institutional database reveals
important associations between treatment parameters and clinical outcomes
for stereotactic body radiotherapy (SBRT) of oligometastatic colorectal
cancer. Radiother Oncol 2022;167:187-194.
22. Nakamura Y, Hokuto D, Koyama F, Matsuo Y, Nomi T, Yoshikawa T, et al. The prognosis and recurrence pattern of right- and left-sided
colon cancer in stage II, stage III, and liver metastasis after curative
resection. Ann Coloproctol 2021;37(5):326-336.
24. Park SH, Shin JK, Lee WY, Yun SH, Cho YB, Huh JW, et al. Clinical outcomes of neoadjuvant chemotherapy in colorectal
cancer patients with synchronous resectable liver ketastasis: a propensity
score matching analysis. Ann Coloproctol 2021;37(4):244-252.
26. Hasselgren K, Røsok BI, Larsen PN, Sparrelid E, Lindell G, Schultz NA, et al. ALPPS improves survival compared with TSH in patients affected of
CRLM: survival analysis from the randomized controlled trial
LIGRO. Ann Surg 2021;273(3):442-448.
27. Vallance AE, van der Meulen J, Kuryba A, Charman SC, Botterill ID, Prasad KR, et al. The timing of liver resection in patients with colorectal cancer
and synchronous liver metastases: a population-based study of current
practice and survival. Colorectal Dis 2018;20(6):486-495.
28. Slesser AAP, Simillis C, Goldin R, Brown G, Mudan S, Tekkis PP. A meta-analysis comparing simultaneous versus delayed resections
in patients with synchronous colorectal liver metastases. Surg Oncol 2013;22(1):36-47.
30. Kim JY, Park IJ, Kim HR, Kim DK, Lee JL, Yoon YS, et al. Post-pulmonary metastasectomy prognosis after curative resection
for colorectal cancer. Oncotarget 2017;8:36566-36577.
31. Pfannschmidt J, Dienemann H, Hoffmann H. Surgical resection of pulmonary metastases from colorectal
cancer: a systematic review of published series. Ann Thorac Surg 2007;84(1):324-338.
32. Meng D, Fu L, Wang L, Dai Y, Lv W, Zhang J, et al. Video-assisted thoracoscopic surgery versus open thoracotomy in
pulmonary metastasectomy: a meta-analysis of observational
studies. Interact Cardiovasc Thorac Surg 2016;22(2):200-206.
33. Mitry E, Guiu B, Cosconea S, Jooste V, Faivre J, Bouvier AM. Epidemiology, management and prognosis of colorectal cancer with
lung metastases: a 30-year population-based study. Gut 2010;59(10):1383-1388.
34. Roh SJ, Park SC, Choi J, Lee JS, Lee DW, Hong CW, et al. Cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy with mitomycin C used for colorectal peritoneal
carcinomatosis. Ann Coloproctol 2020;36(1):22-29.
35. Goéré D, Glehen O, Quenet F, Guilloit JM, Bereder JM, Lorimier G, et al. Second-look surgery plus hyperthermic intraperitoneal
chemotherapy versus surveillance in patients at high risk of developing
colorectal peritoneal metastases (PROPHYLOCHIP-PRODIGE 15): a randomised,
phase 3 study. Lancet Oncol 2020;21(9):1147-1154.
37. Quénet F, Elias D, Roca L, Goéré D, Ghouti L, Pocard M, et al. Cytoreductive surgery plus hyperthermic intraperitoneal
chemotherapy versus cytoreductive surgery alone for colorectal peritoneal
metastases (PRODIGE 7): a multicentre, randomised, open-label, phase 3
trial. Lancet Oncol 2021;22(2):256-266.
38. Mendelaar PAJ, Smid M, van Riet J, Angus L, Labots M, Steeghs N, et al. Whole genome sequencing of metastatic colorectal cancer reveals
prior treatment effects and specific metastasis features. Nat Commun 2021;12:3269
40. Sauer R, Liersch T, Merkel S, Fietkau R, Hohenberger W, Hess C, et al. Preoperative versus postoperative chemoradiotherapy for locally
advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized
phase III trial after a median follow-up of 11 years. J Clin Oncol 2012;30(16):1926-1933.
41. Piozzi GN, Kim SH. Robotic intersphincteric resection for low rectal cancer:
technical controversies and a systematic review on the perioperative,
oncological, and functional outcomes. Ann Coloproctol 2021;37(6):351-367.
42. Eldamshety O, Kotb S, Khater A, Roshdy S, Elnahas W, Zahi MS, et al. Early and late functional outcomes of anal sphincter-sparing
procedures with total mesorectal excision for anorectal
adenocarcinoma. Ann Coloproctol 2020;36(3):148-154.
43. Huh JW, Maeda K, Liu Z, Wang X, Roslani AC, Lee WY. Current status of “Watch-and-Wait” rectal cancer
treatment in Asia-Pacific countries. Ann Coloproctol 2020;36(2):70-77.
44. Garcia-Aguilar J, Patil S, Kim JK, Yuval JB, Thompson H, Verheij F, et al. Preliminary results of the organ preservation of rectal
adenocarcinoma (OPRA) trial. J Clin Oncol 2020;38:4008
45. Dossa F, Chesney TR, Acuna SA, Baxter NN. A watch-and-wait approach for locally advanced rectal cancer
after a clinical complete response following neoadjuvant chemoradiation: a
systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2017;2(7):501-513.
46. van der Valk MJM, Hilling DE, Bastiaannet E, Meershoek-Klein Kranenbarg E, Beets GL, Figueiredo NL, et al. Long-term outcomes of clinical complete responders after
neoadjuvant treatment for rectal cancer in the International Watch &
Wait Database (IWWD): an international multicentre registry
study. Lancet 2018;391(10139):2537-2545.
47. Kong JC, Guerra GR, Warrier SK, Ramsay RG, Heriot AG. Outcome and salvage surgery following "Watch and
Wait" for rectal cancer after neoadjuvant therapy: a systematic
review. Dis Colon Rectum 2017;60(3):335-345.
48. Giunta EF, Bregni G, Pretta A, Deleporte A, Liberale G, Bali AM, et al. Total neoadjuvant therapy for rectal cancer: making sense of the
results from the RAPIDO and PRODIGE 23 trials. Cancer Treat Rev 2021;96:102177
49. Bahadoer RR, Dijkstra EA, van Etten B, Marijnen CAM, Putter H, Kranenbarg EM, et al. RAPIDO collaborative investigators. Short-course radiotherapy
followed by chemotherapy before total mesorectal excision (TME) versus
preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in
locally advanced rectal cancer (RAPIDO): a randomised, open-label, phase 3
trial. Lancet Oncol 2021;22(1):29-42.
50. Oh SG, Park IJ, Seo J, Kim YI, Lim SB, Kim CW, et al. Beware of early relapse in rectal cancer patients treated with
preoperative chemoradiotherapy. Ann Coloproctol 2020;36(6):382-389.
Translational Validation of a Novel Multi-Locus ctDNA Methylation Assay for Early Detection and Stratification of Colorectal Cancer: An Exploratory Prospective, Case-Control Study Hayoung Lee, Jae Cheol Kang, In Ja Park, Gwang-un Kim, Hwi Hyun, Na Young Min, Sungwon Jeon, Byoung-Chul Kim International Journal of Molecular Sciences.2026; 27(13): 5738. CrossRef
The delayed cancer treatment and economic inequality in Korea: results of common cancers by the time-to-surgery
Noorhee Son, Woo-Ri Lee, Dong-Woo Choi, Kyu-Tae Han Epidemiology and Health.2025; 47: e2025056. CrossRef
Enhancing the anti-cancer potential of resveratrol through cocrystal technology in colorectal cancerous rats Durga Polati, Prasad Neerati Scientific Reports.2025;[Epub] CrossRef
Weighing the benefits of lymphadenectomy in early-stage colorectal cancer Seung Min Baik, Ryung-Ah Lee Annals of Surgical Treatment and Research.2023; 105(5): 245. CrossRef
Update on Diagnosis and Treatment of Colorectal
Cancer
Fig. 1.
Age-standardized incidence rates of colorectal cancer in Korea,
1999–2019. Adapted from Kang et al. [1] with CC-BY-NC.
Fig. 2.
Cytoreductive surgery for patients with peritoneal carcinomatosis from
colorectal cancer. Peritoectomy process at (A) pelvic cavity, (B) left upper
quadrant, (C) intestinal organs, (D) and small bowel mesentery. Adapted from
Kim and Kim 2021 [16] with
CC-BY-NC.
Fig. 1.
Fig. 2.
Update on Diagnosis and Treatment of Colorectal
Cancer
Clinically available non-invasive screening method with stool DNA
detection for colorectal cancer diagnosis